
Abstract
Cluster headache (CH) – a severe, painful, and always unilateral syndrome – is characterized by periodicity and symptoms of both cranial parasympathetic activation (i.e. rhinorrhoea, lacrimation) and sympathetic deficit (i.e. meiosis, ptosis, and impaired sweating) (1). Dodick et al. (2) have suggested hypothalamus dysfunction as the primary CH mechanism.
In a previous report on angiographic changes during a CH attack, Ekbom and Greitz (3) described dilation of the ophthalmic artery and spasms in the extradural segment of the internal carotid artery on the same side as the headache.
In this report we will describe two case studies of patients with cluster-like headache resulting from vertebral artery dissections and lateral medullary infarctions. We present angiographic evidence of vascular activation during these headaches as well as evidence of cyclical attacks during cluster-like headache.
Case reports
Case 1
A 45-year-old female suffering from acute onset pain over the right side of her neck, accompanied by dizziness, numbness, and unsteadiness was admitted to our neurological ward on 10 January 2001. She was not involved in a traffic accident, nor did she receive massage or chiropractic treatment prior to her attack. Her history revealed 17 years of controlled hypertension, but she denied having a history of headaches.
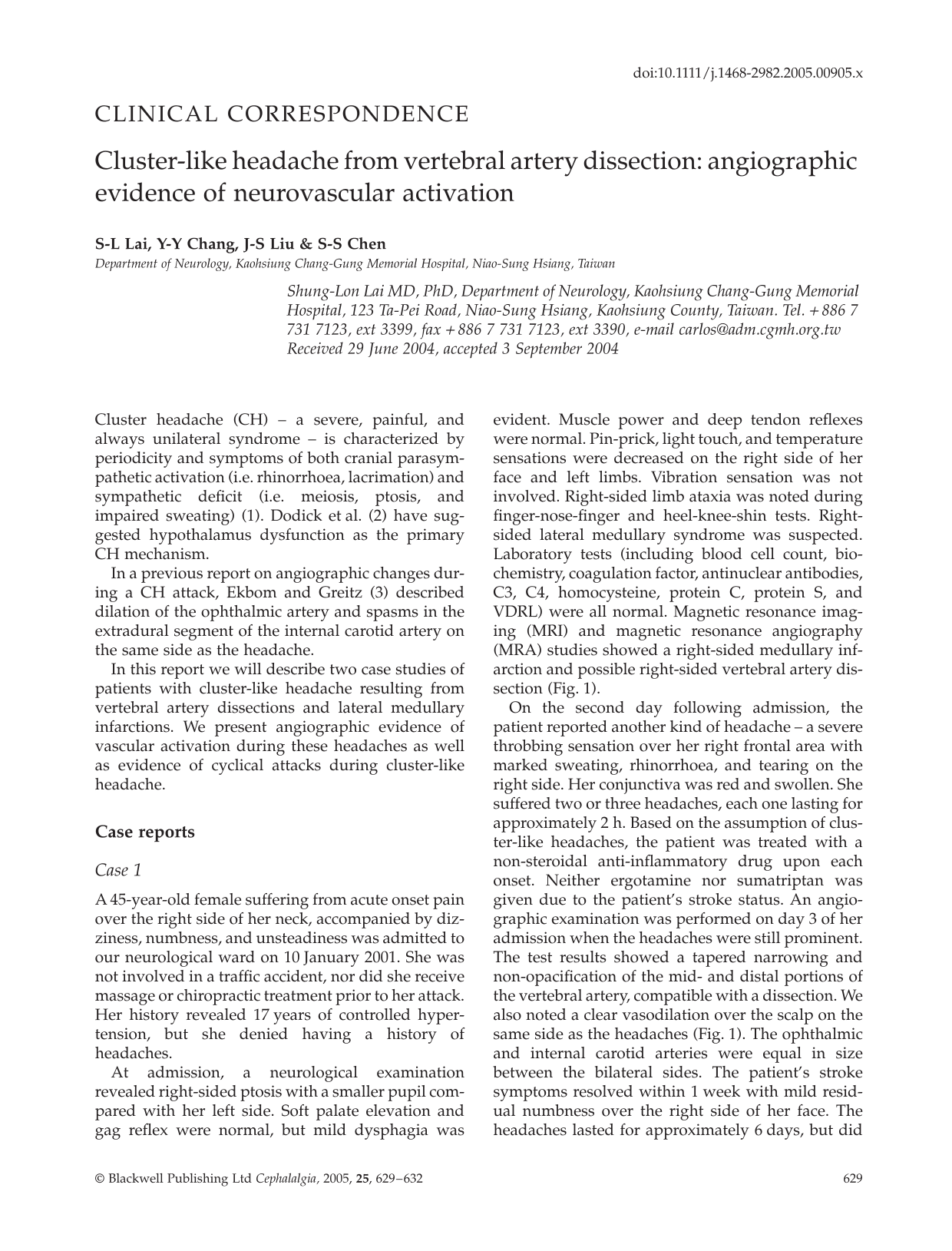
At admission, a neurological examination revealed right-sided ptosis with a smaller pupil compared with her left side. Soft palate elevation and gag reflex were normal, but mild dysphagia was evident. Muscle power and deep tendon reflexes were normal. Pin-prick, light touch, and temperature sensations were decreased on the right side of her face and left limbs. Vibration sensation was not involved. Right-sided limb ataxia was noted during finger-nose-finger and heel-knee-shin tests. Right-sided lateral medullary syndrome was suspected. Laboratory tests (including blood cell count, biochemistry, coagulation factor, antinuclear antibodies, C3, C4, homocysteine, protein C, protein S, and VDRL) were all normal. Magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) studies showed a right-sided medullary infarction and possible right-sided vertebral artery dissection (Fig. 1).

(a) Right internal carotid angiography showed increased vascularity over right scalp while the left side (b) was normal. The increased vascularity disappeared during follow-up (not shown). (c) Tapering sign of right vertebral artery was noted in the angiogram of aorta. (d) High signal change in right lateral medullar area was noted in the magnetic resonance imaging flair image.
On the second day following admission, the patient reported another kind of headache – a severe throbbing sensation over her right frontal area with marked sweating, rhinorrhoea, and tearing on the right side. Her conjunctiva was red and swollen. She suffered two or three headaches, each one lasting for approximately 2 h. Based on the assumption of cluster-like headaches, the patient was treated with a non-steroidal anti-inflammatory drug upon each onset. Neither ergotamine nor sumatriptan was given due to the patient's stroke status. An angiographic examination was performed on day 3 of her admission when the headaches were still prominent. The test results showed a tapered narrowing and non-opacification of the mid- and distal portions of the vertebral artery, compatible with a dissection. We also noted a clear vasodilation over the scalp on the same side as the headaches (Fig. 1). The ophthalmic and internal carotid arteries were equal in size between the bilateral sides. The patient's stroke symptoms resolved within 1 week with mild residual numbness over the right side of her face. The headaches lasted for approximately 6 days, but did not re-occur during 3 years of subsequent treatment. Vasodilation on the right side did not appear in her second angiography 6 months later.
Case 2
A 37-year-old male patient had a fall in the shower, after which he experienced dizziness, perioral numbness, right-sided clumsiness, and an unsteady gait. He was sent to our ER on 25 December 2000. Upon admission, a neurological examination showed mild right-sided ptosis with a smaller pupil compared with the left side. He claimed to have no prior history of headaches. Results from muscle power tests over four extremities were all grade 5; deep tendon reflexes were normal, as were the results of a sensory test. Right-sided limb ataxia was noted during finger-nose-finger and heel-knee-shin tests. The patient complained of dull neck pain. Right-sided lateral medullary syndrome was suspected.
Laboratory blood tests revealed elevated triglyceride levels (269 mg%), but all other biochemistry data (blood cell count, erythrocyte sedimentation rate, coagulating factor, protein C, and protein S) were normal. Results from a heart survey, including Holter's monitor and echocardiography, were normal. Increased flow speed over the vertebral artery was noted during a duplex study. Brain MRI and MRA tests identified an infarction over the right medullary area (Fig. 2).

(a) High signal change in right lateral medullar area was noted in magnetic resonance imaging diffusion-weighted image. (b) Right internal carotid angiography showed increased vascularity over right scalp. (c) Pseudoaneurysm over right vertebral artery was noted in right vertebral angiography. (d) The psedoaneurysm was embolized after the second lateral medullary syndrome.
Around 23.00 h on the third night following admission, the patient complained of a severe headache over the right temporal area and a stabbing sensation behind the right eye, which was accompanied by excessive lacrimation, rhinorrhoea, and sweating over the right side of his face. For the next five nights he suffered from the same headache pattern for approximately 2 h. The patient responded positively to 100% oxygen. An angiogram performed the morning following the last headache revealed signs of tapering in the bilateral vertebral artery and a pseudoaneurysm over the right vertebral artery (Fig. 2). Similar to the first patient, mild vasodilation was noted on the right scalp during the capillary phase. Renal angiogram results were normal. We treated the patient with heparinization, followed by warfarin. His stroke symptoms improved within 14 days, and the CH-like headaches resolved 6 days after onset.
A follow-up angiogram performed in May 2001 showed improvement over the left vertebral artery but persistent right vertebral dissection and aneurysm enlargement. An embolization procedure was suggested but refused because of cost. In December of the same year he experienced another attack of right-sided ataxia accompanied by sensory change in the right face and left side of the body. During admission, he reported the onset of a CH-like headache similar to the ones he had suffered a year earlier. An MRI exam revealed a new infarction over the right-sided medullary area. He received an angiogram with embolization of the right distal vertebral artery after the attending physician noted an enlargement of the pseudoaneurysm (Fig. 2). The aneurysm disappeared following placement of a coil, and the patient's neurological status improved within 1 week. He received wafarin as part of his out-patient treatment.
He experienced a third episode of numbness in the right side of his face and left side of the body in October 2002. As with the preceding two episodes, Horner's sign, sensory dissociation, and ipisilateral ataxia were associated with the right-sided medullary area, and a brain MRI confirmed a new infarction. A new angiogram showed a patent left vertebral artery and a proximal portion of the vertebral artery. However, no cluster-like symptoms appeared. This time the stroke symptoms resolved within 10 days. No new strokes or cluster-like headaches have been noted during 1.5 years of follow-up treatment and examinations.
Discussion
Both cases presented with a combination of right lateral medullary infarction and right vertebral artery dissection. The second patient had a pseudoaneurysm resulting from the vertebral artery dissection. Both had initial neck pains which may have resulted from either the infarctions or dissections, and both experienced another severe, stabbing pain over the retro-orbital and temporal areas. Both patients had injections over their eyes, with lacrimation and sweating, ipsilateral ataxia at the headache site. Another similarity was ptosis and small pupils that were present following their strokes. In the first patient, the headache frequency was several per day; in the second, the headaches occurred near midnight and ceased following treatment with 100% oxygen.
Both patients’ headaches were very similar to CH: severe unilateral orbital, supra-orbital, or temporal pain lasting 15–180 min untreated; autonomic effects that included conjuntival injection, lacrimation, rhinorrhoea, or Horner's syndrome on the side experiencing pain; and an attack frequency of one per 48 h to several times per day on eight consecutive days (1). The headache could be classified as trigeminal-autonomic cephalalgia.
Cluster-like headaches resulting from posterior circulation dysfunction have been described in one vertebral artery aneurysm case (4), two basilar artery cases (one with an ectasia [5] and the other with an aneurysm [6]), one case with a cervical cord infarction (7), one case with a lateral medullary infarction (8), and two cases of vertebral dissections with cervical cord and medullary infarctions (9, 10). Combined, the data from these cases suggest (i) a trigeminal-autonomic reaction was activated from the upper cervical or medullary segments, which overlap and connect with the trigeminal nucleus; (ii) the ecstatic basilar artery caused the compression of the trigeminal root; or (iii) the aneurysmal dilation of the vertebral or basilar artery may have irritated other nociceptive receptors that are synaptically associated with the upper cervical segments and therefore capable of affecting the trigeminal nucleus; (iv) an imbalance between both autonomic systems and created by the lesion of the sympathetic system in lateral medulla could have contributed to the cluster-like headache.
The second patient had three lateral medullary infarctions, but the cluster-like symptoms appeared only following the first two strokes; the vertebral dissection and pseudoaneurysm resolved after the second. This suggests that a cluster-like headache moves through dissections and aneurysms, which irritate the cervical innervations over these structures and therefore affect the trigeminal nucleus. The dissection and lateral medullary infarction were also confounding factors of the headaches experienced by the first patient.
In non-human primates, the stimulation of vascular afferents leads to neuronal activation in the trigeminocervical complex – that is, the superficial layers of (i) the trigeminal nucleus caudalis near the cervicomedullary junction and (ii) the dorsal horns of the C1 and C2 levels of the spinal cord (11). Giffin and Goadsby have suggested that the anatomical connection between C1/C2 and the trigeminocervical complex, including connections to the superior salivatory nucleus that mediate parasympathetic activity, may be the point of origin for autonomic features similar to those we observed in our patients (6).
The onset of a headache at the same time late at night is a classic CH pattern. In such cases, the hypothalamus is usually considered the point of origin, since it contains posterior cells that regulate autonomic functions and anterior nuclei that serve as the primary circadian pacemaker in mammals – both of which are strongly associated with the clinical symptoms and periodicity of cluster attacks. However, the second patient's lesion is insufficient for explaining the entire situation in terms of periodicity, since a connection exists between trigeminal nuclei and dorsal raphi nuclei before connecting to the hypothalamus. As with other locations of symptomatic CH (12), a possible explanation is the salutary effect of afferent stimulation within the area where the headache pain is felt.
In the first patient, marked vasodilation over the scalp ipisilateral to the headache was noted in the angiograph taken during her headache stage. No change was noted in the ophthalmic artery or internal carotid artery. Ekbom and Greitz describe one case of CH developing during an angiogram; they observed a dilation of the ophthalmic artery and spasms in the extradural segment of the internal carotid artery (3). May et al. (13) looked at MRA data for patients suffering from CH and reported vasodilation in the region of the major basal arteries. They concluded that cranial vessel dilation is not specific to any particular headache syndrome but generic to cranial neurovascular activation, probably mediated by the trigeminoparasympathetic reflex. In our patients, the vasodilation appeared during the headache phase and resolved during the follow-up examinations. We believe this demonstrates an association between trigeminal-autonomic cephalagia and vascular activation.
Vasodilation in the scalp may be a manifestation of a CH-like state. The CH-like pictures we observed were probably related to dissections or aneurismal dilations that triggered cervical nerves or lesions of the sympathetic system in lateral medulla which caused an imbalance of the autonomic system and activated the two patients’ trigeminal-autonomic systems.