
Abstract
Bath-related headache (BRH) is a rare primary headache syndrome. We present our experience over seven years and review all reported cases of BRH. Thirteen patients, including six from our group, are described. BRH occurred exclusively in middle-aged or elderly Oriental women (mean age 51 years, range 32-67. Hong Kong 6 cases, Taiwan 4 cases, Japan 3 cases). The typical presentation was a uniphasic cluster of severe headache recurrently triggered by bathing or other activities involving contact with water. Each attack lasted 30 min to 30 h. Onset was hyperacute, consistent with that of thunderclap headache. Reversible multisegmental cerebral vasoconstriction was found in two patients. No underlying secondary causes were identified. Response to acute treatment was generally unsatisfactory, but headache could be prevented by avoiding the specific trigger(s). BRH runs a self-limiting course; all patients remitted within three months after onset. Nimodipine may shorten the duration of illness.
Introduction
Headache provoked by bathing is a rare condition. It was first reported by our group as ‘shower-induced headache’ (1). We classified it under Category 4, miscellaneous headaches unassociated with a structural lesion, of the IHS Classification System. Subsequently, several cases of bath-related headache (BRH) were described (2–4). The terms used in these reports included ‘benign hot bath-related headache’, ‘hot bath-related headache’ and ‘bathing headache’. Liao et al. (3) first proposed that bathing headache is a variant of idiopathic thunderclap headache (TCH) because of similar clinical and angiographic profiles (5–7).
Queen Mary Hospital and Pamela Youde Nethersole Eastern Hospital are two district general hospitals on Hong Kong Island. We provide acute service to an urban population of about one million. Over the past seven years, we encountered six patients with BRH, including the two previously reported cases. Their characteristics and clinical course are described (in chronological order of presentation). We also review all the cases of BRH reported in the English language literature.
Case reports
Patient 1
A previously healthy 67-year-old woman developed acute bitemporal headache during a hot shower. It was very intense, throbbing, and radiated to the occipital region. The pain built up rapidly to maximum intensity at its onset. There was associated scalp tenderness. The headache gradually subsided over one hour. Afterwards, the same symptoms recurred everyday as soon as she started taking a shower. Each episode lasted 60–90 min. The pain improved partially with oral dextropropoxyphene. There was a mild diffuse headache in between the attacks. She was admitted through the emergency department (ED) on the fourth day. Neurological examination was unremarkable. Her blood pressure (BP) was not elevated. Computerized tomography (CT) did not reveal subarachnoid blood or other structural lesions. Cerebrospinal fluid (CSF) was clear and there was no xanthochromia. All laboratory tests, including CSF analysis, vasculitic screen and erythrocyte sedimentation rate, were normal. Transcranial Doppler (TCD) showed normal flow velocities in the posterior circulation. The temporal windows were insufficient for study. Over the next 10 days, her headache recurred whenever shower was attempted. Prophylactic mefenamic acid or paracetamol before a shower were ineffective. There was one episode of similar headache provoked by defecation. On day 17 after onset, she was given an oral dose of sumatriptan before challenged with a shower; no attack was provoked. She remained asymptomatic from then onwards. Magnetic resonance imaging (MRI) performed one month later showed age-related subcortical ischemic changes only.
Patient 2
A 50-year-old woman with good past health suddenly developed recurrent severe headache every time she took a hot shower. The headache was generalized and throbbing. Onset of headache was simultaneous with beginning of a shower and the pain built up rapidly to maximum intensity. Each attack lasted for up to one hour. She noticed no other provoking factors. She presented through the ED one week after onset. Neurological examination and BP were unremarkable. Brain CT with contrast and all blood tests were also normal. She could not tolerate propranolol and was treated with low dose amitriptyline. The same pattern of headache continued to recur over the next three months. Her symptoms then resolved and bathing could be tolerated. Amitriptyline was given for another three months before cessation. She remained asymptomatic with no relapse of similar headache.
Patient 3
A 51-year-old woman presented through the ED with severe headache. She had a history of limb-girdle muscular dystrophy, familial polyposis coli treated with colectomy, and ventricular septal defect repaired many years ago. She suddenly developed severe frontal headache while having a hot shower. The pain started as soon as the water jet fell onto her upper body, became very intense immediately, and lasted about 30 min. She then experienced the same headache whenever she had a shower. She visited the ED on day 4 because the pain was getting more severe. Physical examination showed wasting of her proximal muscles and was otherwise unremarkable. BP was normal. She was discharged with a supply of dextropropoxyphene. The attacks continued to recur, and similar but milder headache also occurred upon rinsing her mouth with cold water. She revisited the ED again 10 days later and was referred for admission. Brain CT, CSF and all blood tests were normal. MRI showed several small deep frontal foci of T2W-hyperintense signals; Flow void of the intracranial vessels was preserved. Electroencephalography (EEG) revealed intermittent runs of theta discharge at bifrontal regions. Mefenamic acid, sumatriptan or buprenorphin before shower were not effective. She was also given sodium valproate. Her symptoms started to improve four weeks after onset and she could tolerate shower without headache one week later. Sodium valproate was discontinued six weeks later with no further relapse. The EEG abnormalities remained unchanged on subsequent assessments.
Patient 4
A 47-year-old woman with history of duodenal ulcer went on vacation and had an episode of near-drowning in the hotel swimming pool. She was rescued immediately and did not sustain any injury. On the next day, she suddenly developed a very intense band-like headache with nausea and vomiting about 10 s after beginning a hot shower. It subsided after 10 min. Afterwards, the same symptoms recurred everyday once she took a shower. There were no other provoking factors. The headache became more persistent and lasted 30 min to four hours. There was a mild right occipital throbbing headache in between the attacks. She presented to the ED on day 5 and was referred for admission. Neurological examination, BP, all blood tests, CSF and EEG were normal. Brain CT showed bilateral basal ganglial calcification only. Paracetamol before a shower could not prevent an attack. Etodolac partially relieved the pain. The severity of headache gradually improved over the next week. She did not experience further shower-induced headache since day 10 after onset.
Patient 5
This patient referred to our clinic was seen four months after onset of her symptoms. She was a 58-year-old housewife with mild asthma on low-dose inhaled bronchodilator. She had occasional tension headache which never required medical attention. Her BRH started three months after menopause. She had recurrent headache triggered by warm or cold shower and micturition but not by soaking in a bath. She limited her fluid intake and tried to hold her urine for as long as possible to avoid provoking an attack. The headache was a severe gripping pain at the vertex. Intensity was already maximum at the beginning. Associated features included vomiting, sweating, scalp tenderness, slurred speech and mild gait unsteadiness. The headache lasted from two to nine hours. She was well in between apart from occasional tapping sensation at the vertex. She visited the ED once because of severe headache. The pain was partially relieved with ketorolac injection. BP was 170/90 but the subsequent readings were normal. Physical examination was otherwise unremarkable. Brain CT did not reveal subarachnoid blood or other abnormalities. She was then managed by her general practitioner and was prescribed paracetamol, nimesulide, diazepam and gabapentin, but without much effect. Her symptoms remained static until four weeks later when she started to improve with shorter attacks and less severe pain. After two weeks, she was able to resume shower without headache. When we first saw her, she was already asymptomatic. Neurological examination, BP and blood tests were normal. MRI only showed a small arachnoid cyst at the right cerebellopontine angle.
Patient 6
This 50-year-old woman had noninsulin dependent diabetes mellitus. Glycemic control was satisfactory. She also had history of thyrotoxicosis treated with partial thyroidectomy. One day while having a hot shower, she suddenly developed an excruciating left-sided bursting headache. It was of split-second onset as soon as water came into contact with her upper body and rapidly became very severe. The pain was aggravated by movements and was associated with nausea and vomiting. She did not have photophobia or phonophobia. The pain subsided after one hour. This was followed by daily attacks of shower-induced headache. On the fifth day, the pain was very intense and persistent. She took multiple doses of paracetamol and dextropropoxyphene but her headache did not subside until six hours later. She was then admitted. Neurological examination, BP, brain CT and all laboratory tests were normal. TCD showed increased flow velocity at left posterior cerebral artery (PCA). Oral nimodipine was commenced at 30 mg every four hours but she remained symptomatic. She also noticed headache when her face was exposed to steam, with micturition, and during an episode of watery diarrhoea. However, bathing with cold or lukewarm water did not provoke an attack. MRI performed on day 11 after onset showed focal narrowing at both PCA (Fig. 1). No acute white matter changes or infarction was detected. Nimodipine was stepped up to 60 mg every four hours on day 12. Her last attack occurred that evening. There was no further recurrence afterwards and she could resume bathing with hot water. TCD five days later showed normalization of flow velocity in left PCA. MRI four weeks after remission also showed resolution of the initial vasoconstriction (Fig. 1). No delayed ischemic stroke was found.

(a, b) Three-dimensional time-of-flight MRA on day 11 after onset of symptoms demonstrating multifocal short segment narrowing at bilateral posterior cerebral arteries (arrow) on lateral and axial views. The arteries of the anterior circulation were relatively spared. (c, d) Follow-up MRA (similar views) four weeks later depicted the complete resolution of vasoconstriction in the posterior cerebral arteries. All the arteries had smooth outline.
A summary of these six patients and other reported cases of BRH (2–4) are shown in Table 1.
Summary of clinical features, investigation findings and outcome in our patients and other reported cases of bath-provoked headache.

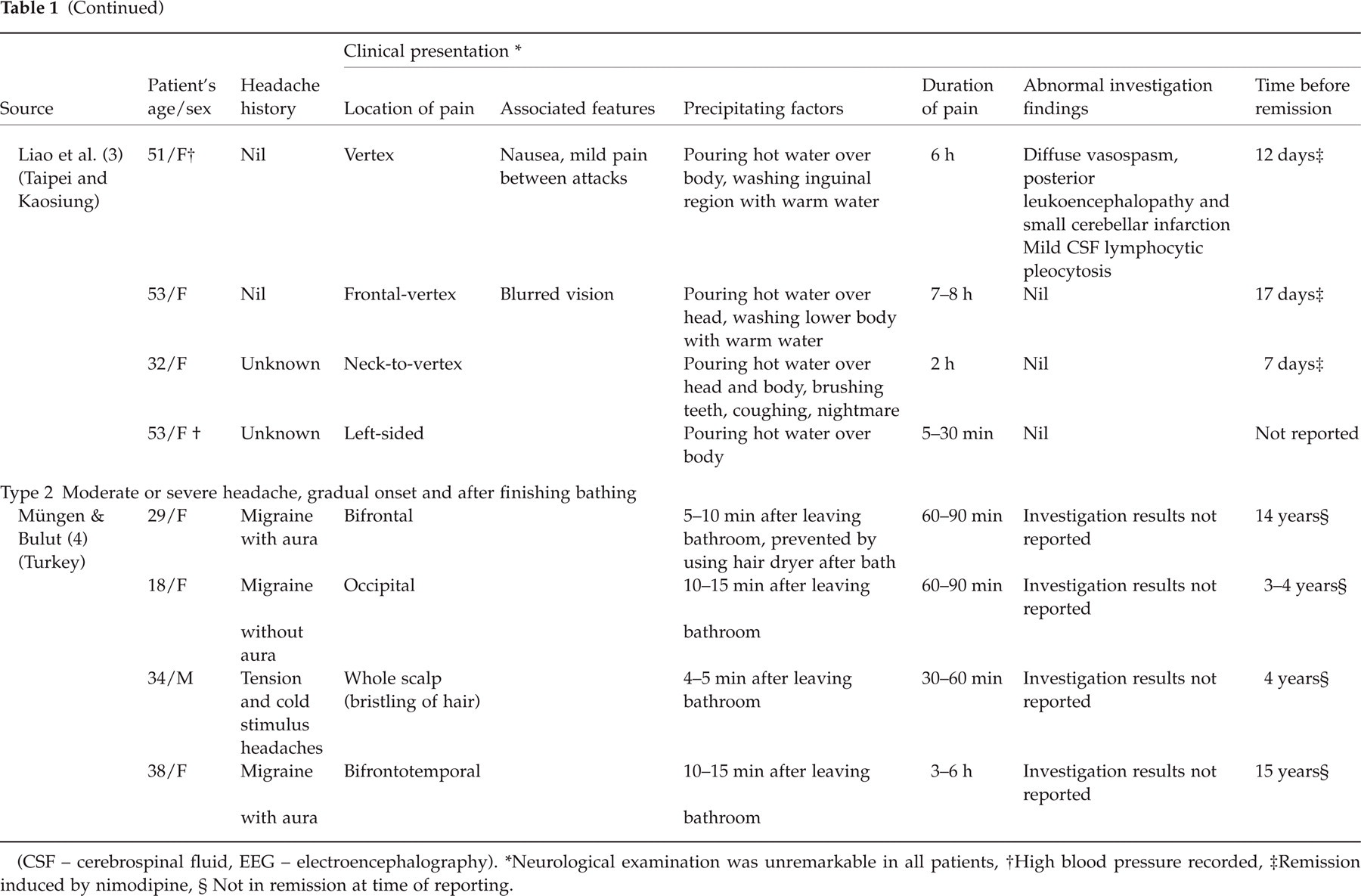
(CSF – cerebrospinal fluid, EEG – electroencephalography).
Neurological examination was unremarkable in all patients,
High blood pressure recorded,
Remission induced by nimodipine,
Not in remission at time of reporting.
Discussion
Headache precipitated by bathing was first recognized by Negoro et al. (2). They diagnosed three Japanese cases in 1991 and 1992, characterized by recurrent headache every time the patients took a bath or poured hot water over themselves. The clinical picture is similar in our six Chinese patients and the four Taiwanese patients reported by Liao et al. (3). These 13 patients had a unique pattern of presentation. They all had paroxysmal, intense headache stereotypically triggered by specific activities that involved contact with water. These included taking a shower, soaking in hot bath, exposure to steam, tooth brushing, mouth rinsing, and even micturition. Onset was simultaneous upon exposure to these triggers. The headache was not always ‘hot bath-related’; besides, it could be brought about by cold water. The patients usually stopped regular bathing since the pain was very severe and could be prevented by avoiding the trigger. Not the whole body surface was equally susceptible to stimulation; some patients could wash their hair or lower body without symptoms but had excruciating pain provoked when other areas came into contact with water. Less common precipitating factors included defecation, diarrhoea, exposure to cold, coughing and nightmare. The provoked pain built up hyperacutely within seconds to maximum intensity before its gradual resolution. Some patients had a mild background headache in between the attacks. Neurological examination was normal in all patients. This type of BRH is a self-limiting condition; spontaneous remission is the rule after a few weeks to several months. There is no report of relapse after the initial cluster. To date, all the reported cases with this type of BRH were middle-aged or elderly Oriental women. The reason for this exclusive pattern of racial, gender and age distribution is unknown but is probably unrelated to cultural background because the patients were from different countries.
BRH is a unique headache syndrome. The clinical profile of BRH satisfies the diagnostic criteria of TCH without neurological signs or symptoms (1.1 under the Dodick criteria) (3, 7). The pathogenic mechanism of BRH is unknown. There is so far no plausible explanation for this odd phenomenon of headache provoked repeatedly by bathing or contact with water. It seems that direct skin stimulation and temperature change are both essential components of the trigger. Heat alone, however, is insufficient to provoke an attack. The flow of water may also be important; some patients could tolerate stationary but not running water. Idiopathic TCH can be precipitated by various stimuli including exertion, sexual intercourse or orgasm, and Valsalva maneuvers by coughing, sneezing, weight-lifting and straining (7). Bathing or activities involving contact with water should also be recognized as a specific provoking factor of TCH. The pattern of recurrence in BRH is also unusual and different from other types of TCH; the precipitation of symptoms is consistent and almost inevitable with every exposure to the stimuli. The result is a high frequency of attacks within a short period of time. This stereotypic nature and phasic occurrence of symptoms are similar to those of cluster headache (CH). Hot bath can also precipitate attacks in CH but this is related to increased body heat rather than specific to bathing (8). The clinical manifestations of BRH are not compatible with CH. It is also uncommon for CH to affect middle-aged and elderly women. No other type of headache is known to be provoked by heat or warm water.
Some intracranial disorders can also produce TCH, including aneurysmal subarachnoid haemorrhage, cerebral venous thrombosis, pituitary apoplexy, arterial dissection, and hypertensive encephalopathy (6, 7, 9). No serious underlying cause for headache was identified after appropriate workup in all the cases. Imaging studies did not show any relevant structural lesions in our patients. The EEG abnormality in Patient 3 was probably longstanding and unrelated to the headache.
TCH is associated with multisegmental cerebral vasoconstriction (5–7, 10–13) and posterior leukoencephalopathy (9). The vasoconstriction is transient and completely reverses after resolution of TCH. Liao et al. reported similar radiological findings in one of their patients with bathing headache (3). Our last patient also had transient vasospasm but no leukoencephalopathy. (Nevertheless, we might not detect the acute radiological changes in some of our patients because immediate access to MRI was not always available in our hospitals.) The exact pathogenic mechanisms of TCH and its associated radiological changes remain poorly understood. Vasospasm may be mediated by an exaggerated neurogenic vasomotor reflex (6, 7), which probably applies to BRH as well. Pain in these headache syndromes may be the direct result of vasomotor changes. Alternatively, pain and vasospasm may be mediated independently by some underlying unknown physiological disturbances through different pathways.
All patients with this type of BRH had a favourable clinical outcome. Hence, the term ‘benign hot bath-related headache’ was originally used (2). Neurological deficits of delayed onset were not observed. Only one of the reported cases was complicated by subclinical cerebellar infarction detected on MRI at two weeks after onset of headache (3). Nevertheless, TCH-associated vasospasm may cause stroke with persistent neurological deficits, seizure, coma and death (10–12).
Patients with BRH generally responded poorly to acute treatment including simple analgesics, narcotics and nonsteroidal anti-inflammatory drugs. Although antimigraine drugs were tried in some early cases – sumatriptan in Patients 1 and 3 and ergotamine in one of Negoro's cases, the use of these agents is inappropriate given their potential risk of exacerbating vasoconstriction. Our patients were also treated with amitriptyline, sodium valproate or gabapentin. They all improved but probably in the natural course of BRH rather than as a result of treatment. Similarly, Patient 1 might have already remitted before given sumatriptan.
Liao et al. (3) first reported the efficacy of nimodipine in hastening recovery in BRH. Remission was induced in all their patients within three days of commencing oral or intravenous treatment. Our last patient also remitted one day after stepping up the dosage of oral nimodipine. The therapeutic efficacy of calcium channel antagonsits in TCH (11, 12) as well as BRH may further suggest a similar pathogenic mechanism for both conditions. Symptoms of BRH can be disabling, particularly in patients whose precipitating factors are unavoidable like micturition. Therefore, a trial of nimodpine to shorten the duration of BRH is worthwhile despite its self-limiting and relatively benign course. The potential risk of ischemic complications from vasospasm is another indication to justify the use of nimodipine (3, 12).
Müngen and Bulut (4) reported four patients with BRH from Turkey but their clinical manifestations were rather different (Table). Instead of intense headache of split-second onset precipitated instantaneously by bathing, these patients’ symptoms were delayed by up to 15 min after leaving the bathroom. The headache also built up slowly and could be of moderate severity only. The problem lingered on for many years without remission. All the patients had other primary headache syndromes as well. Therefore, we classify these four cases as Type 2 BRH to distinguish them from the usual pattern seen in Oriental women.
To summarize, BRH is a rare primary headache syndrome. Two types of BRH are recognized. The first type is a variant of idiopathic TCH that occurs exclusively in middle-aged or elderly Oriental women. The clinical course is usually benign and self-limiting. Nimodipine may hasten its remission. The clinical presentation is different for Type 2 BRH, which is probably a separate disease entity.
Note added in proof
Since acceptance of this article, another case of thunderclap headache provoked by bathing has been published (14). The patient was a 46-year-old women from Taiwan.