
Abstract
Our aim was to study and compare pharmacoepidemiology of headache treatment in two different settings: inside and outside a specialized Centre. We analysed the differences in headache treatment between 612 subjects admitted for the first visit (‘naive’) (F/M: 2.41; mean age = 37.31 ± 14.09 years) and 620 subjects admitted for a control visit (F/M: 3.18; mean age = 44.30 ± 15.37 years) to the Headache Centre of the University of Modena and Reggio Emilia. Most patients suffered from migraine. As acute treatment, on the first visit, 49.4% of them were taking drugs prescribed by a doctor; 41.5% were taking over-the-counter analgesics (OTCAs); 9.1% were not taking any drug. On the control visit, 81.3% of patients were taking prescription drugs; 15.8% OTCAs; 2.9% were not taking drugs (overall chi-square = 139.229, P < 0.001). Non-selective analgesics were the most-used drugs. Triptans were used by 9.1% of ‘naive’ patients and by 31.8% of patients attending for the control visit (Fisher's Z = 7.655, P < 0.001). Nimesulide was the most-used drug. A prophylactic treatment was made by 16.8% of ‘naive’ patients, and by 58.2% of patients admitted to the control visit (Fisher's Z = 12.135, P < 0.001). Antidepressants were the class of drugs most used for prophylaxis. Amitriptyline was the drug for prophylaxis most frequently used by patients attending the control visit, while flunarizine was the most frequently used by ‘naive’ patients. Before being examined in a specialized centre, few patients take prescription drugs, triptans, or prophylactic drugs; specialized care increases the proportion of patients taking prophylactic drugs, and changes the type of acute treatment used into disease-specific medication for headache.
Introduction
People suffering from headaches do not make much use of health services (1), they seldom see general practitioners or specialists (2–5), and – even if a diagnosis and a drug prescription have been made – often do not go back to the doctor (6), but limit themselves to trying to control headache by over-the-counter analgesics (OTCAs) (7–11). This might be because of organizational or economic barriers to health services admittance and the purchasing of prescription drugs (3, 12). In Italy, however, headache care should be perfectly adequate, as the National Health Service (NHS) gives everyone free assistance from a general practitioner, allows them to take advantage of a specialized consulting physician at a low additional charge (16.55 euro for the first visit; 10.35 euro for a control visit), and allows them to get many prescription drugs used for the treatment of primary headaches with no or little extra charge. Moreover, in Italy, self-medication is not practised much, and the use of OTCAs is quite insignificant compared with the United States and other European countries (13).
At present, patients and clinicians have an unprecedented range of therapeutic options available for headache treatment (10, 14–16). Moreover, the awareness of the individual, and social and economic impact of primary headaches (2, 12, 17–24) should have improved the standard of treatment for these disorders. The aim of this study was to evaluate and compare the pharmacoepidemiology of headache treatment in two different settings: both inside and outside a specialized centre (that is, either made directly by the patients or prescribed by their family doctor). So, we analysed the differences in headache treatment between subjects admitted for the first visit, and those coming to the out-patients’ wards of our Headache Centre of the University of Modena and Reggio Emilia for a control visit.
Patients and methods
All patients consecutively attending the out-patients’ wards of the Headache Centre of the University of Modena and Reggio Emilia in the course of the first 6 months of 2001, either for the first visit or for a control visit, were asked how they had been treating their headache during the last month. Informed consent was routinely obtained from all patients involved in this study; no patient refused to participate. As far as abortive treatment is concerned, we asked the patient to indicate the most important drug (just one drug) in his opinion.
The Headache Centre has been operating in Modena, a town of about 180 000 inhabitants situated in the middle of the region of Emilia Romagna, since 1980. Starting from 1990 onwards, an annual average of more than 1000 new patients visits the centre. A visit to the Headache Centre can be booked only after a written request from the general practitioner. In the course of the first 6 months of 2001, 612 patients applied to the centre for the first time (F/M: 2.41; mean age = 37.31 ± 14.09 years; range 14–78 years); the overwhelming majority (595; 97.2%) had been sent by their family doctor; only few (17; 2.8%) by specialists or by the doctor of a first-aid station. Six hundred and twenty patients (F/M: 3.18; mean age = 44.30 ± 15.37 years; range 14–79 years) applied for a control visit, as a rule, advised by a specialist of the centre. Patients who returned more than once during the period of the study were evaluated at the first control visit only. The two groups were significantly different for F/M ratio (chi-square = 4.568, P = 0.033) and mean age (Student's t =− 8.303, P < 0.001).
The diagnosis of headache was made according to the IHS criteria (25) by a specialist of the centre. Some chronic daily headaches, not of the chronic tension-type, could not be classified according to the IHS criteria because, in most cases, they were transformed migraines (26). Possible non-pharmacological treatments made by patients were not investigated.
Data analysis
Patients sent to the centre for the first time were compared with patients coming for a control visit according to age, sex, diagnosis and kind of therapy. Drugs taken by the patients were classified as medications for acute treatment [triptans; ergot derivatives; analgesics (non-steroidal anti-inflammatory drugs, alone or combined with metoclopramide, codeine, caffeine, acethaminophen, prochlorperazine, butalbital); others (muscle relaxants, benzodiazepines)] and drugs used for prophylactic treatment (antidepressants, beta-blockers, calcium channel blockers, benzodiazepines, anticonvulsants).
Data were inserted into a specially created database and statistically analysed by means of SPSS 8.0 software, version for Windows (SAS Institute, Cary, NC, USA). A descriptive analysis of all parameters was performed by drawing up contingency tables for all the non-parametric variables. The data obtained thus were processed and compared by the chi-square test, followed by Fisher's exact probability test. The mean ages of the patients of the two groups were compared by means of the Student's t-test for unpaired data. Differences were considered significant at P < 0.05 (27).
Results
For both patients coming for the first visit and those coming for a control visit, the headache was diagnosed as migraine in the majority of cases (Table 1) by the specialists of the centre (first visit: 495, 80.9%; control visit: 468, 75.5%). Chronic tension-type headache was more represented in patients coming for a control visit (74, 11.9%) than in patients coming for the first visit (49, 8%) (P < 0.001).
Distribution by diagnosis of patients admitted at the Headache Centre for the first visit or for a control visit

∗P < 0.001, Fisher's exact test.
†Transformed migraine.
Less than half patients coming for the first visit (302 out of 612, 49.4%) used prescription drugs for acute treatment of headache; 41.5% (254 out of 612) used OTCAs, and quite a few (56 out of 612, 9.1%) used no drug at all. In contrast, most patients coming for a control visit used prescription drugs (504 out of 620, 81.3%), a minority used OTCAs (98 out of 620, 15.8%) and only few used no drug (18 out of 620, 2.9%). As far as acute treatment is concerned, differences between the two groups of patients were statistically significant (overall chi-square = 139.229, P < 0.001). Analgesics were the most widely used drugs, on both the first and the control visit (Table 2). However, at the control visit, the use of triptans was more than tripled, whereas the use of analgesics decreased, with respect to the first visit (triptans: first visit 9.1%, control visit 31.8%, P < 0.001; analgesics: first visit 85.5%, control visit 63.4%, P = 0.002). In either group, a few patients used ergot derivatives. Nimesulide, a NSAID, was the most-used drug, either at the first visit or at the control visit (Table 3). The five drugs most used by the patients who came to the Centre for the first visit were NSAIDs, or the combination of indomethacin plus caffeine plus prochlorperazine. However, the three triptans available in 2001 were among the five drugs most used by patients coming for the control visit.
Class of drugs for acute treatment taken during the last month by patients attending the Headache Centre for the first visit or for a control visit (subjects who didn’t take any drug were excluded)
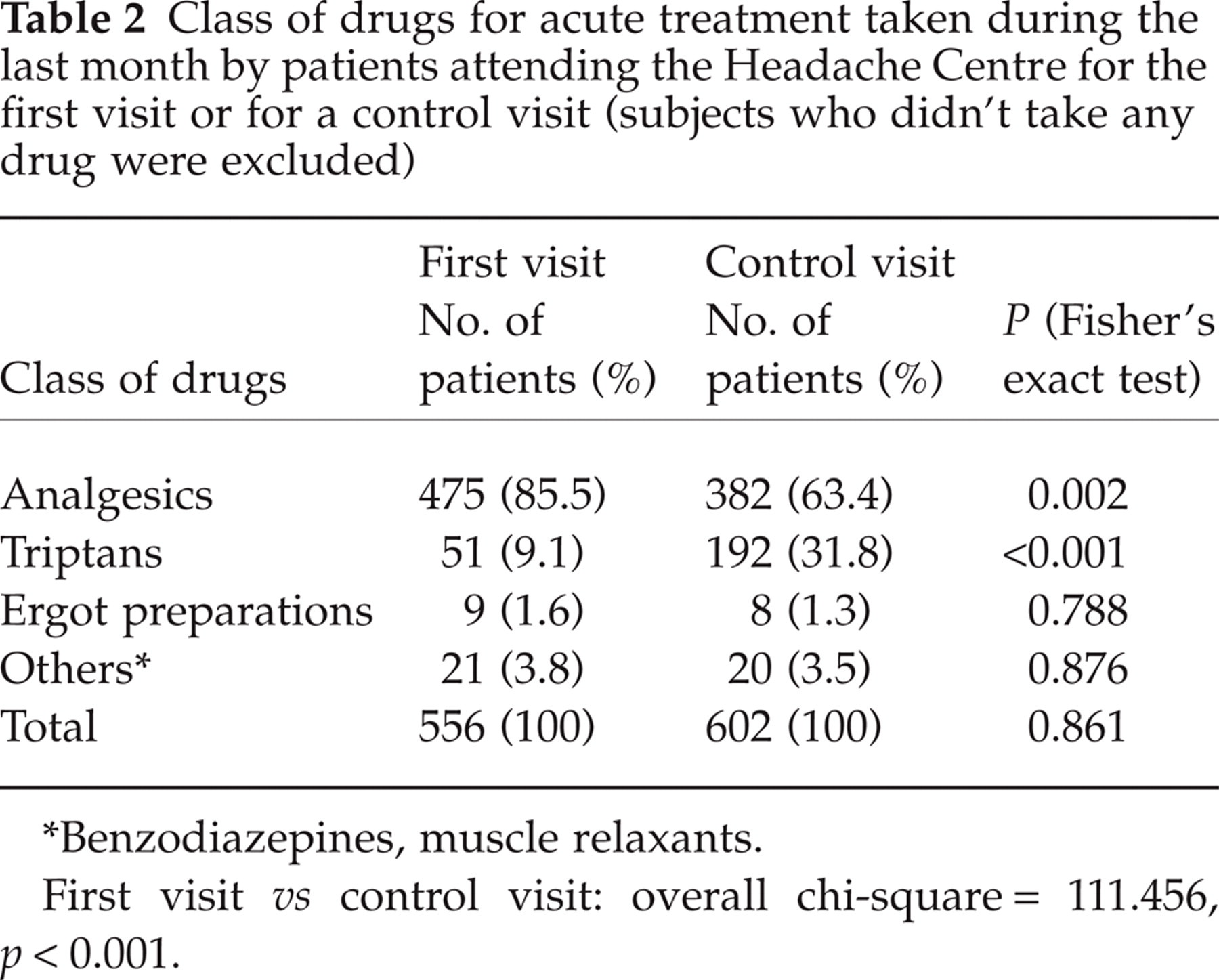
∗Benzodiazepines, muscle relaxants.
First visit vs control visit: overall chi-square = 111.456, p < 0.001.
Fifteen most-used drugs for acute treatment taken during the last month by patients addressed to the Headache Centre for the first visit or for a control visit

∗Indomethacin + prochlorperazine + caffeine
†butalbital + propyphenazone + caffeine
‡ergotamine + caffeine + aminophenazone.
Only 103 out of 612 (16.8%) patients who came to the centre for the first visit had taken a prophylactic treatment in the last month, compared with 361 out of 620 patients (58.2%) returning for the control visit (Fisher's Z = 12.135; P < 0.001). Antidepressants were the most widely used drugs for prophylaxis (Table 4), followed by calcium channel antagonists, either by patients coming for the first time or by those coming for a control; amitryptiline and flunarizine being the most used in their respective class (Table 5). Patients coming for the first time consumed more benzodiazepines (21.4%) than patients returning for a control (6.8%, P < 0.005). Other drugs for prophylaxis, such as valproic acid, verapamil and lamotrigine were only used by patients coming for the control visit.
Class of drugs for prophylactic treatment taken during the last month by patients addressed to the Headache Centre for the first visit or for a control visit (subjects who didn’t take any drug were excluded)

∗First visit vs control visit: P = 0.004, Fisher's exact test
∗∗First visit vs control visit: P < 0.001, Fisher's exact test.
Fifteen most-used drugs taken for prophylactic treatment during the last month by patients addressed to the Headache Centre for the first visit or for a control visit

Discussion
Recent advances in headache care have little influenced the treatment of headache, both by patients and by general practitioners. The less than half (49.4%) of the headache patients examined for the first time in the Headache Centre of the University of Modena and Reggio Emilia had taken prescription drugs for acute treatment in the last month; the other patients either used OTCAs (41.5%) or didn’t use any drug (9.1%). However, contrary to what has been reported in other studies (3, 6, 12), after having received a diagnosis and a therapy by the specialist of the Headache Centre, 81.3% of patients returning for the control visit were using prescription drugs; only 15.8% continued to use OTCAs, and very few (2.9%) didn’t take any drug at all for acute treatment.
Among headache patients, those suffering from migraine most frequently seek specialist treatments (7, 20, 28, 29), either because they are worried or because they are unsatisfied with the remedies advised by their family doctor (30). During the first six months of 2001, the large majority of patients attending the Centre suffered from migraine
In the region of Emilia Romagna, triptans are fully at the expense of the NHS; therefore, if they are prescribed by the doctor, there should be no reason not to use them, because the cost for the patient is lower than that of an OTCA. Nevertheless, among the five drugs most used for acute treatment of headache by the patients coming to our centre for the first visit (Table 3), there were no triptans, but only analgesics, all of them paid entirely by the patients. It is possible that general practitioners are reluctant to prescribe triptans because of their cost for the NHS. In fact, in not having to exceed a fixed-expenditure budget for drugs, it may be that they choose to save in headache care, which is usually considered as a minor illness (24), and could be treated by prescribing mainly analgesics and therefore not at the expense of the NHS. However, in a wider perspective
Another reason for the poor prescription of triptans might be the difficulty for general practitioners in making a correct diagnosis. Migraine is, in fact, largely undiagnosed (21, 35, 36), so the treatment is seldom specific (37). In the absence of a correct diagnosis, patients mostly use OTCAs, while, for the majority of them, other treatments would be required (38). In accordance with this interpretation, while the number of patients taking drugs for abortive treatment was not significantly different between the two groups, the types of drugs they took were different. In patients coming for the control visit, the use of analgesics lowered to 63.4% (Table 2), while that of triptans increased to 31.8%; the three triptans available in Italy being among the five most-used drugs (Table 3).
What characterizes the specialist's management of headache is the use of a prophylactic treatment (30), which is often ignored by general practitioners (37). In our study, only 16.8% of patients coming to our centre for the first time had taken a prophylactic treatment during the last month, compared with 58.2% in the case of patients coming for the control visit. The most widely used drugs for prophylaxis (Table 4), both at the first visit and at the control visit, were antidepressants, but benzodiazepines were also largely used, mostly by patients coming for the first visit. However, depression (often associated with anxiety) is one of the most common problems in the setting of general practice (39, 40). Moreover, depression is frequent among both general headache patients and those who apply to specialist centres (41). Amitriptyline was definitely the most widely used antidepressant drug (Table 5) and the most prescribed (24.8%) by the specialists of our centre for prophylactic treatment. It is also the first choice for the treatment of chronic tension-type headache, from which about 12% of patients returning for the control visit suffered. General practitioners seem to prefer flunarizine, which is the prophylactic drug most frequently used (21.4%) by patients coming to the centre for the first visit. Among the drugs used by these patients are neither valproate nor verapamil, which, in Italy, are not registered for the prophylactic treatment of either migraine or cluster headache, although they are included in the guidelines of the Italian Society for the Study of Headaches (42) for this use. Also, the low use of anti-epileptic drugs in the speciality patients at the control visit might depend on the centre's specialists being internists (instead of neurologists) and therefore not used to prescribing these drugs
Our investigation has some limits. We have not analysed the treatment of headache in the same patients before and after their visit to our Headache Centre. However, although we have studied different subjects, the distribution by diagnosis was quite similar in the two groups (Table 1), with the only exception being a larger number of chronic tension-type headaches among patients at the control visit (first visit: 8%; control visit: 11.9%; P < 0.001). These patients were older (mean age of patients of the control visit: 44.30 ± 15.37 years; first visit: 37.31 ± 14.08 years, P < 0.001) and included a greater number women (control visit: 76.1%; first visit: 70.8%; P = 0.03), in agreement with the notion that women seek a doctor's care more frequently than men (43–45). Moreover, our intention was to study and compare the pattern of pharmacological treatment in two different settings. It was not to evaluate whether, and why, the treatment of the same patient changed after consultation at the centre.
Another limit of our study is represented by the peculiarity of the Italian pharmaceutical market, that is particularly reflected in the list of the 15 drugs for acute therapy most used by patients coming to the centre for the first visit (Table 3): the highest on the list was nimesulide, used by 28.6% of the patients. Nimesulide is a sulphonanilide NSAID with low gastrointestinal ulcerogenicity, widely used in Europe for its analgesic and anti-inflammatory activities. This drug, marketed in Italy since 1985, is an outstanding success as an analgesic among headache patients (about 24 million prescriptions per year in 2000 and 2001) (46). The combination of indomethacin, prochlorperazine and caffeine, that is listed in the SISC guidelines (42) as a third-level drug which might be recommended for migraine management, was among the five most-used products (7.5%). In English-speaking countries, however, the drugs that are most-often used for acute headache management are acetaminophen, ibuprofen and aspirin (11, 47). Ibuprofen was also largely used by our patients (13.5%), whereas acetaminophen was only in sixth position (5.7%).
In conclusion, in Italy, where self-medication is not widespread, and the NHS offers medical assistance to everybody, many patients (41.5%) continue to use OTCAs, while a few use triptans (9.1%) or take prophylactic treatment (16.8%) before visiting a specialized centre. This is in spite of scientific progress in the field of headache and the efforts made by scientific societies to improve the standard of treatment.
Contrary to what has been reported in studies performed in other countries (6–11), after the diagnostic and therapeutic framing, patients coming to the centre for a control visit take more prescription drugs (81.3%), triptans (31.8%) and prophylactic therapies (58.2%), and at the same time reduce self-medication (15.8%). It seems that general practitioners are reluctant to be involved strongly or directly in the management of primary headache, and that they prefer to delegate specialists to prescribe those treatments that require a precise diagnosis. Possibly, general practitioners may feel that they are inadequately prepared, and/or try to check the pharmaceutical costs, without taking into account, or even ignoring, the fact that pharmaceutical costs are negligible in comparison with the indirect costs of primary headaches (48). Such an approach does not help the patient, overburdens the specialist structures, and is ultimately expensive. In fact, the waiting list for a first visit to our centre is very long, and we observe from our study that the patients on the list are, in the main, migraineurs (80.9%). These patients could receive the most appropriate treatment from their own doctor, as only an accurate clinical history and a complete medical examination are required to diagnose migraine, rather than special tests.
To summarize, the results of our present study strongly indicate that it is necessary to increase the role and the involvement of general practitioners in the management of primary headaches. Considering the large prevalence of migraine in the population, it is not feasible that migraineurs have to apply to specialist centres to obtain proper treatment. Specialists should be consulted only in a second phase, for the most complex cases, or for those resistant to the therapy prescribed by the general practitioner.
From our study, it emerges that the effect of specialist care is to increase the proportion of patients taking prophylaxis and to change the type of acute treatment used into disease-specific medication for headache.