
Abstract
Objective:
The pediatric cardiac intensive care unit, a department dedicated to caring for cardiac patients, conducted a program evaluation to identify registered nurse (RN) and family perceptions of barriers and facilitators to parent engagement during postoperative care after surgery.
Methods:
A quasi-experimental presurgical/postsurgical design examined RN data using the Questionnaire of Factors That Influence Family Engagement and parent perception of engagement data via a survey.
Results:
Nearly half (44.6%) of RNs responded; most were younger (30–49 years old, 44.8%), female (91.4%), and White (94.8%) and held a bachelor's degree (72.4%). Those with more experience (>15 vs. <5 years) had a higher parent engagement score (p = .021). RNs indicated that workflow (τb = .579, p = .000), unit environment (τb = .572, p = .000), nurse attitude (τb = .520, p = .000), and patient acuity (τb = .519, p = .000) correlated with overall family engagement score. The nine parents (100%) invited responded; most were mothers (n = 7, 77.8%) and married (n = 6, 66.7%), and 56% (n = 50) indicated this was not the child's first hospitalization. Parent overall safety score improved (presurgery/postsurgery, Z = −2.000, p = .046). RN barriers for family engagement included lack of written policy. For parents, a facilitator for engagement was safety. Both groups identified collaboration, communication, and shared decision making as a facilitator.
Discussion:
Results contribute to planning and implementing quality improvement initiatives. Understanding and developing a partnership between parents and RNs, nurturing mutual respect, and enhancing shared decision making improves parent engagement in care and, ultimately, a child's physical and psychological health.
BACKGROUND
Meaningful family-centered care requires that nurses and other health practitioners actively partner with families and patients. Parent engagement is a key factor in recovery for postoperative and hospitalized critically ill children (Hill et al., 2019; Rennick et al., 2014). Several studies support parent-centered engagement and empowerment in rehabilitative care of patients in the intensive care unit (ICU) to optimize outcomes (Davidson et al., 2017; Davidson & Zisook, 2017; Haines, 2018; Rennick et al., 2014; Richards et al., 2017). To promote parent engagement, the role in supporting parent engagement for the parent and nurse needs to be clearly defined and better understood.
Encouraging family engagement and participation as an integral part of promoting the health, safety, and well-being of children is now the gold standard for care (McBride et al., 2016). In support of the initiative, guidelines recommend enhancing parent engagement and promoting parents as equal partners (Davidson et al., 2017). Facilitated sensemaking, a midrange theory, promotes the development of caring relationships, encourages family presence and participation, teaches strategies for family engagement, and prepares families with communication, information gathering, and decision-making skills (Davidson & Zisook, 2017). These guidelines and theory recommend open communication and encourage nurses to accommodate the needs of pediatric patients and families within critical care units.
Many studies validate the benefits of supporting parent-centered engagement and empowerment. Promoting parent engagement reduces fear and anxiety by offering purpose, knowledge, and understanding. Families are provided tools, training, and resources needed to help care for the pediatric patient (Skoog et al., 2016). Other studies have described various interventions used by staff to promote parent-centered engagement and recommended empowerment strategies (Burns et al., 2018; Craske et al., 2019). Personalizing information has shown family participation at the bedside provides mutual benefit to patients and families (Craske et al., 2019). Identifying barriers to engagement and developing individualized care build trust and a caring relationship (Burns et al., 2018).
Multifactorial studies describe specific interventions to promote parent-centered engagement and report the results from implementing empowerment strategies. Parent anxiety and stress can be reduced through conversations and trust. Several studies show that personalized care reduces psychological distress. One study found that nurses improved family well-being and reduced family stress by facilitating health-promoting conversations, which allowed parents to express feelings, thoughts, and experiences (Agren et al., 2019). Nurses advocating for hope and building a family–nurse relationship based on trust and encouragement resulted in reduction in posttraumatic stress after ICU care (Alfheim et al., 2019). Another study found that physical and cultural environmental factors can impact parents’ perception and that information sharing, participation, respect, dignity, and collaboration are key concepts necessary for family-centered care in the ICU setting (Hill et al., 2019). Other studies show the importance of creating mutual knowledge, respect, listening, trust, and developing competencies for parents through interdisciplinary training and education (Brødsgaard et al., 2019; Goldfarb et al., 2017; Uhm & Kim, 2019).
Healthcare systems continue to strive to improve the quality and safety of care. Guidelines recommend family presence in the pediatric ICU care setting to improve patient and family outcomes (Davidson & Zisook, 2017; Society of Critical Care Medicine, 2020). Family engagement and empowerment are essential to delivering patient-centered care (Institute of Medicine [U.S.] Committee on Quality of Health Care in America, 2001). Guidelines published by the Society of Critical Care Medicine (Hwang et al., 2020) support family-centered care (Davidson et al., 2017) and promote facilitated sensemaking (Davidson & Zisook, 2017). Intentional focus of the parent and patient interactions to be more beneficial and more efficient with postoperative care may result in enhanced recovery and positive patient outcomes. A focus on the evaluation of barriers and facilitators to parent engagement would support a quality improvement initiative.
Current State of the Organization
An organizational assessment identified that current practices were in alignment with the department's goal to involve parents with care activities at the bedside in the pediatric cardiac ICU (PCICU). Current activities included open visitation, communicating with care team members and care plans on whiteboards, and involving parents with bedside rounds and change-of-shift reports. Team collaboration was noted to be strong. Limitations and barriers were noted to daily patient care activities including technical aspects and resource availability. Limitations were also found in sociocultural factors, including parents’ empowerment and willingness to engage.
The leadership of PCICU recognized the importance of parental engagement as they embarked on a quality improvement initiative to promote early mobility and reduce the complications of prolonged bed rest for PCICU patients after cardiac surgery. Recognizing the importance of family engagement toward the goal, the organization's nursing leadership desired to form a deeper understanding of registered nurse (RN) and parent perceptions of the family role in caring for a postoperative patient in the PCICU.
Goal, Purpose, and Objective
The overarching goal of this program evaluation is to enhance patient recovery and health outcomes using family-centered care. The purpose is to identify barriers and facilitators to parent engagement to inform an improvement initiative. The specific objective is to conduct a program evaluation, obtaining input from RNs and parents on barriers and facilitators to parent engagement before and after cardiac surgery in the PCICU.
METHODS
A program evaluation was conducted to identify RN and family perceptions of barriers and facilitators to parent engagement during cardiac surgery. The Consolidated Framework for Implementation Research (Damschroder et al., 2009) and Program Evaluation Framework (Stufflebeam, 1983) underpinned this work. The internal review board at the site determined the project was exempt.
Design
A quasi-experimental presurgical/postsurgical design was used to conduct a program evaluation. RN and parent perceptions were examined.
Sample and Setting
Convenience sampling was used to recruit RNs and parents. The setting was a six-bed PCICU that cares for children under 18 years old requiring cardiac intensive care services. The unit is located within a 234-bed, urban, freestanding children's hospital in the Midwest where cardiothoracic surgeons perform over 200 procedures annually. The spectrum of surgery ranges from complex neonatal repairs (such as staged single-ventricle palliation and arterial switch operations for transposition of great arteries) to repair of septal defects and valve repair/replacement. Postoperative care is provided by RNs who receive training in care of children in the PCICU setting.
Inclusion Criteria
Included were all RNs employed in the PCICU. Also included were parents or legal guardians of pediatric surgical patients who were less than 18 years old and admitted to and discharged from the PCICU between November 2020 and February 2021.
Measures
Demographic and characteristic data were obtained on baseline surveys. For RNs, this included age, gender, race, years of critical care experience, and highest degree earned, and for parents, it included relationship to child and marital status.
RN data were collected on the Questionnaire of Factors That Influence Family Engagement (QFIFE) (Hetland et al., 2017), which is a 15-item questionnaire with four subscales that measured nurse perception of the environment, patient acuity, workflow, and attitude. Each item contains a 6-point Likert scale ranging from strongly agree to strongly disagree. A mean score was obtained for each subscale and overall. Higher mean scores indicate perceived facilitators have a greater level of influence, whereas lower mean scores indicate perceived barriers to family engagement in patient care.
Parent surveys included nine questions and used a 6-point Likert scale to examine perceptions of parent engagement in patient care activities in the PCICU. The survey questions were created based on recommendations from the CAHPS Hospital Survey (Agency for Healthcare Research and Quality (AHRQ), 2023). The surveys measured parent perception of overall experience, engagement, safety, communication, participation, being a member of the care team, feedback, information, and education.
Data Collection
Strategies used to conduct the evaluation included cultivating a relationship with PCICU RNs and parents; assessing the organization for readiness, strengths, weaknesses, opportunities, and threats; and performing a literature review of evidence-based engagement activities (Powell et al., 2015). The survey tools were administered to the identified RNs and parents to evaluate perceptions regarding parental involvement in care activities in the unit. Several domains impacting parent engagement were examined to guide the early mobility improvement initiative.
Data were collected from RNs via an electronic survey distributed via email between October 15 and 31, 2020. The email explained the importance of parent engagement activities within the PCICU and provided a link to complete the electronic survey.
Data were collected from parents before the surgery after the surgical consult (presurgery) and at the time of the patient discharge (postsurgery), between November 1, 2020, and February 15, 2021. A paper version of the survey was handed to parents of children who met the inclusion criteria presurgery and postsurgery. When two parents were present, the parents completed the survey together and returned the form to the project manager.
Statistical Analysis
Demographic and characteristic data were analyzed using descriptive statistics. QFIFE RN mean scores were calculated for each question and subscale, and Kruskal–Wallis H test was used to determine whether there was a difference in median scores among demographics. Kendall's tau-b rank correlation coefficient test was used to examine the relationship among subscales in the QFIFE. Parent survey answers were coded, and a mean score for each question was obtained. Evaluation questions were grouped together into main topics centered around overall experience, engagement, and safety during the hospital stay. Wilcoxon signed-rank test determined if there were differences among presurgery and postsurgery survey questions. Data were analyzed using SPSS Version 26, and significance was determined if p value was <.05.
RESULTS
Demographics and Characteristics
Table 1 displays demographic and characteristic data. RNs responded at a rate of 44.6% (58 of 130). The highest number of respondents were between the ages of 30 and 49 years (44.8%, n = 58). Most were female (91.4%, n = 53) and White (94.8%, n = 55). Most had a bachelor's degree (72.4%, n = 42), and 48.3% (n = 28) reported having less than 5 years of critical care experience. All parents (100%) invited to complete the survey responded. Mothers responded 77.8% (n = 7), and both mothers and fathers responded the remaining 22.2% (n = 2). Of the nine parent participants, 66.7% (n = 6) were married. Over half of the parents (56%, n = 50) indicated this was not the child's first hospitalization.
Demographics and Characteristics of RNs and Parents and Impact of Nurse Demographic Variables on the Questionnaire of Factors That Influence Family Engagement (QFIFE) Mean Scores
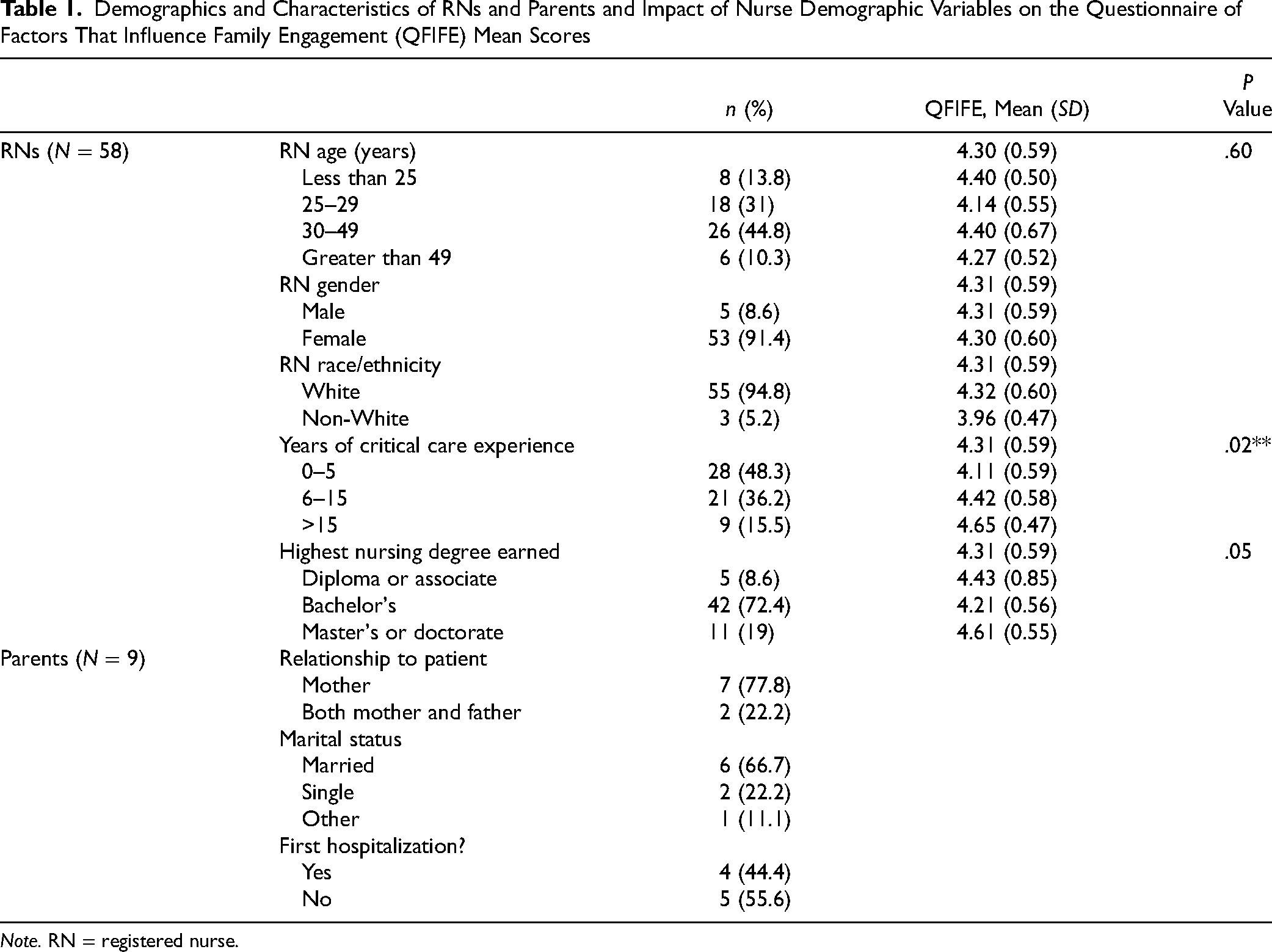
Note. RN = registered nurse.
RN Surveys
QFIFE scores are shown in Table 2. RNs with greater than 15 years of experience in an ICU had higher median QFIFE scores compared with those with 5 years of experience or less (p = .011; Kruskal–Wallis H test). QFIFE subscale scores ranged from 3.91 (ICU environment) to 4.68 (RN workflow). The lowest score was regarding established written policies involving family caregivers in care (M = 3.03, SD = 1.39). The highest score tied between involving family caregivers to make decisions (M = 4.98, SD = 0.76) and involving family caregivers increases overall quality of care (M = 4.98, SD = 0.81). RN workflow (τb = .579, p = .000), PCICU environment (τb= .572, p = .000), nurse attitude (τb = .520, p = .000), and patient acuity (τb = .519, p = .000) had a strong, positive correlation to the QFIFE (Kendall's tau-b rank correlation coefficient).
Summary of RN Score on the Questionnaire on Factors That Influence Family Engagement (N = 58)
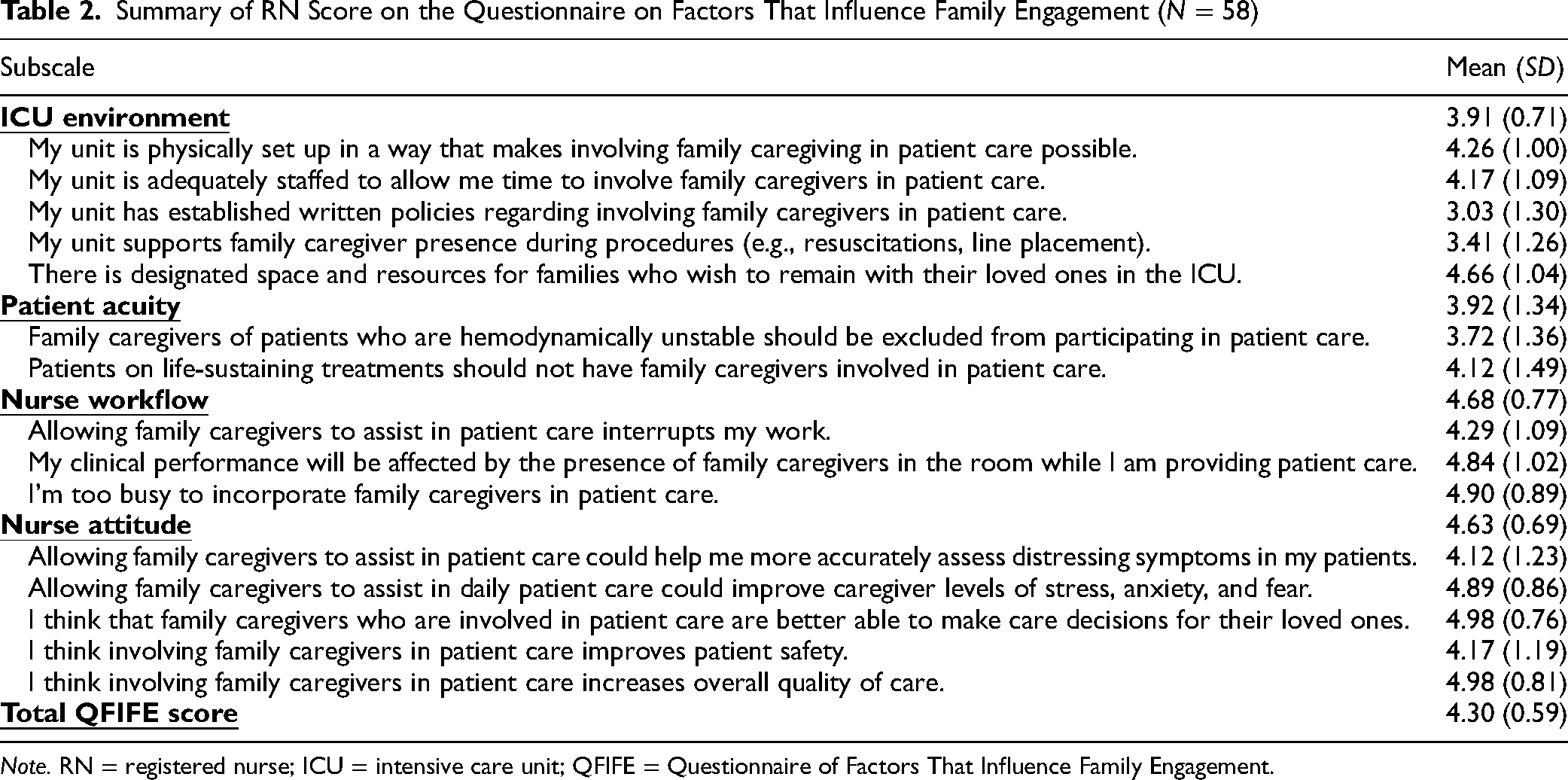
Note. RN = registered nurse; ICU = intensive care unit; QFIFE = Questionnaire of Factors That Influence Family Engagement.
Parent Surveys
The responses of the 81 parents are shown in Figure 1. When presurgery/postsurgery responses were compared, higher values were found on 13.6% (11) responses (negative rank) and 28.4% (23) responses (positive rank), and 58% (47) did not change (tie). Parent perception of overall safety improved presurgery/postsurgery (Z = −2.000, p = .046, Wilcoxon signed-rank test), with median scores increasing from 4.300 to 4.778. No other significant findings were found.
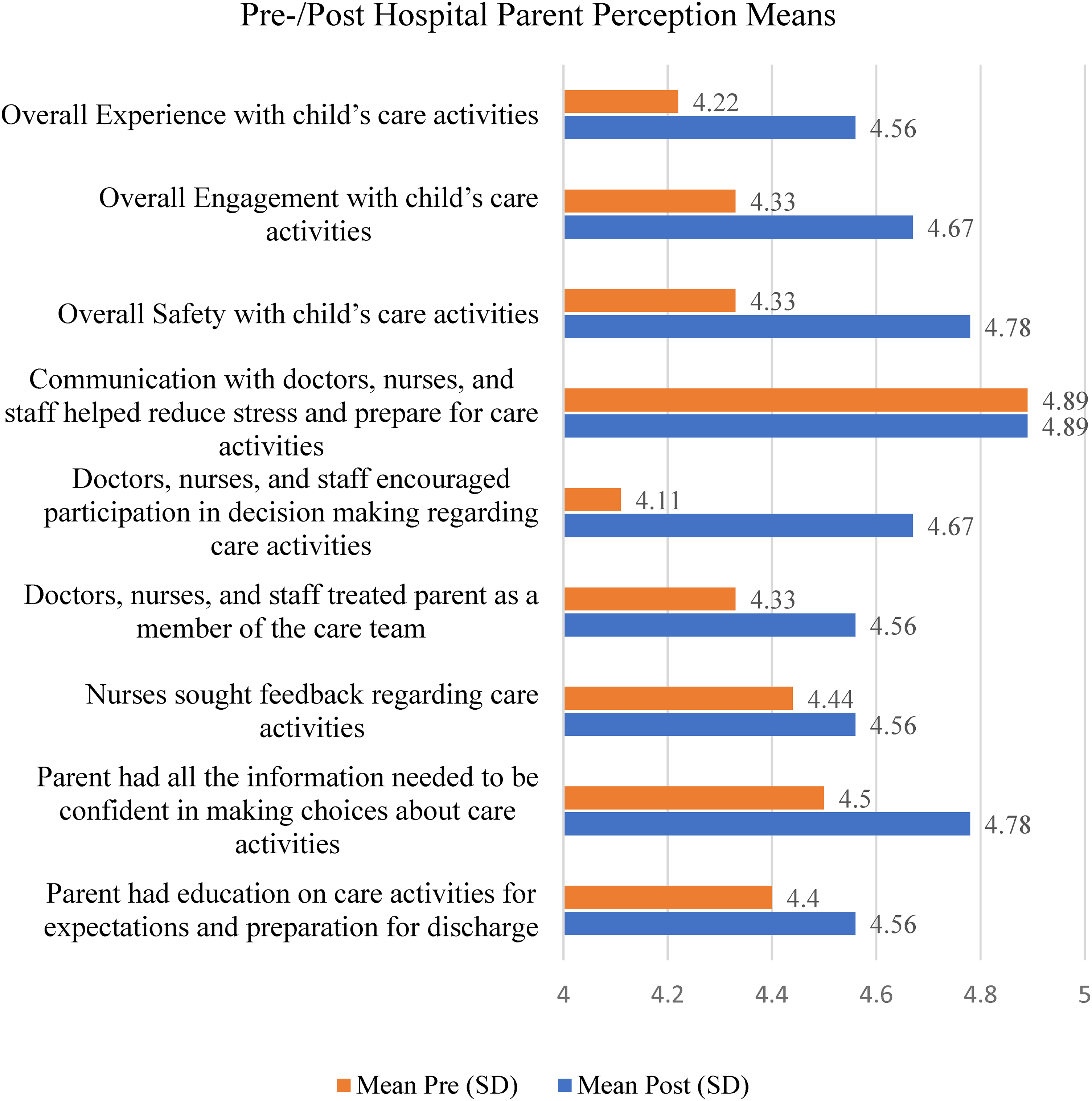
Parent (N = 9) perception mean on the survey before and after surgery.
DISCUSSION
Engaging parents with postoperative care activities in the PCICU presents opportunities and challenges (Burns et al., 2020). Results from the questionnaires provide insight for leaders, identifying barriers and facilitators to parent engagement and, thus, opportunities to strengthen family engagement activities with patient's care. RN demographics and characteristics did not influence nurse perception of family engagement or QFIFE score; however, RNs with more critical care experience were more supportive of family engagement. The results from our overall QFIFE scores further support findings in the literature (Hetland et al., 2017; Hetland et al., 2018) that nurse workflow, ICU environment, nurse attitude, and patient acuity are factors influencing parent engagement. RN findings indicated how nurses view family engagement. Results of this project reinforce the need for RNs to endorse parent engagement and participation with care activities and that communication is imperative, as recommended by prior studies (Craske et al., 2019; Davidson et al., 2017). The organization's nursing leaders gained knowledge of perceived barriers from RNs and can work to improve perceptions and workflow. Guidelines exist to improve parent engagement and participation policies and procedures to promote care activities (Davidson et al., 2017). Enhancing policies can lay a foundation for RNs to implement quality improvement initiatives and optimize family-centered care in the PCICU.
The parent survey found that the child's overall safety facilitated their involvement and engagement in the care of their child. Safety scores after cardiac surgery indicated parents felt the child was safer than the parents perceived the child would be before surgery. These results correspond with the findings reported in the literature (AHRQ, 2023; Hill et al., 2019), emphasizing the need to prioritize parent involvement with daily physician/nursing rounds, communication, and sharing of information, all key to facilitating parent engagement in care to promote patient safety. Parent perception answers on the remaining survey questions did not change. Parents providing the same answers presurgery and postsurgery survey likely show that expectations before surgery were met or exceeded. Results of the parent survey implied they felt they were treated as part of the care team, indicating parent engagement is promoted within the PCICU.
Limitations
The project had several limitations. Perspectives not represented may have been missed. Although additional data would have strengthened the project, the results suggest that parent engagement will improve care at the bedside. COVID-19 was also a limiting factor, as the number of nonemergent surgical cases was decreased because of scheduling restrictions; the PCICU was closed for several weeks during the project, and visitor restrictions may have affected parent perceptions. These factors combined resulted in a lower number of surveys from parents than expected. Finally, because of other confounding variables, such as patient acuity that could not be measured for in this project, parent engagement activities and perceptions may have been impacted.
CONCLUSION
There are several implications from this program evaluation. The use of RNs and parent surveys was effective in identifying RN and parent perceptions of their role in caring for postoperative patients in the PCICU. In addition, barriers and facilitators for engaging parents and RNs with care activities were identified. These findings were consistent with findings in the literature emphasizing the need to create mutual respect, listening, trust, and sharing knowledge (Davidson & Zisook, 2017; Goldfarb et al., 2017; Hill et al., 2019; Rennick et al., 2014; Richards et al., 2017). Enhancing communication, improving information gathering, and increasing participation in decision making are key to successful parent engagement. Hospital nursing leaders need to support initiatives to promote parent partnership through training, education, and RN support (Goldfarb et al., 2017). RNs and parents bring diverse backgrounds, beliefs, and experiences, which can influence communication, participation, and engagement.
The results of this project can promote and strengthen the interaction between nurses, patients, and parent caregivers to enhance patient recovery. Consistent with the literature (Brødsgaard et al., 2019), promoting these concepts will enhance desired patient and family outcomes. The Society of Critical Care Medicine (2020) recommends that hospitals implement flexible hours for visitation, daily meetings with the family, and physical redesign efforts to positively impact family presence (Institute of Medicine [U.S.] Committee on Quality of Health Care in America, 2001) to facilitate keeping families informed, active in decision making, and providing physical and emotional support to the patient.
Focusing on providing patient- and family-centered care, leaders and RNs should promote patient engagement through collaboration, mutual respect, dignity, participation, information sharing, and decision making.
Footnotes
Acknowledgments
We would like to thank those parents who, during a time of family distress, assisted by providing information that will inform and improve care.
Declaration of Conflicting Interests
The authors declare no conflict of interest.