
Abstract
Objective:
To evaluate if treatment of diabetic wounds by copper oxide impregnated dressings (COD) is noninferior to negative pressure wound therapy (NPWT).
Approach:
Following the CONSORT guidelines, patients with diabetes mellitus (type 1 or type 2) and noninfected wounds eligible for treatment with NPWT were randomized into two groups. One group received NPWT followed by standard wound care dressings, whereas the other was treated exclusively with COD. The primary outcome was wound size reduction, measured blindly using a 3D wound-imaging system. Secondary outcomes included patient and caregiver convenience (assessed via visual analog scores), cost, and additional wound parameters.
Results:
COD showed statistically significant noninferiority to NPWT in wound size reduction throughout the study (p < 0.01). The percentage of wounds that closed was 47.83% (11/23) and 34.78% (8/23) in the COD and NPWT arms, respectively (p > 0.05). The average time to wound closure, adjusted to potential confounders, such as gender, age, body mass index, diabetes, and smokers, was similar in both arms (p > 0.05). COD were found to be more convenient than NPWT for both patients (p < 0.001) and caregivers (p = 0.003), with a significantly shorter application time (p < 0.001). The COD cost was 14% of NPWT cost ($470 compared with $3,360).
Innovation:
COD may be considered as the first line of treatment for diabetic foot wounds when NPWT seems indicated.
Conclusions:
Using copper dressings as a first line of treatment of diabetic wounds, when NPWT is indicated, is expected to reduce health costs, improve convenience, and increase compliance without compromising the final outcome.
INTRODUCTION
Diabetic foot infections (DFI) significantly impact health care, causing numerous foot amputations, disabilities, and prolonged hospital stays, and are thus major contributors to health care costs in people with diabetic neuropathy. 1,2 DFI typically start from a diabetic foot ulcer (DFU) that gets infected. DFI that are not successfully treated may progress to severe complications such as osteomyelitis, foot abscesses, necrotizing fasciitis, and gangrene. Treatment is often surgical, involving wide debridement and/or partial foot amputation. After the infection is controlled, closing the wounds is a major task necessary to return the patient to his normal life and prevent another infectious episode. 3
Negative pressure wound therapy (NPWT) is a preferred treatment for large, irregular, or cavity-containing wounds. It promotes granulation tissue formation 4 –6 and helps reduce microbial cross-contamination by sealing the wound and removing bacteria. 4,5,7 Typically, NPWT dressings are changed once or twice a week. NPWTs are notorious for their high cost, are quite inconvenient to the patients, and cannot be applied in some of the wounds due to their location.
An alternative to NPWT for treating these kinds of wounds is copper dressings. Copper has been found to facilitate key wound healing processes such as angiogenesis, extracellular matrix protein production, and epithelialization through its interaction with wound repair factors such as Platelet-Derived Growth Factor (PDGF), Vascular Endothelial Growth Factor (VEGF), Fibroblast Growth Factor (FGF), and Transforming Growth Factor-beta (TGF-β) and enzymes such as superoxide dismutase and lysyl oxidase. 8 –15 In studies, copper has been shown to stimulate the expression and secretion of collagen, elastin, matrix metalloproteinases, and serine proteases by dermal fibroblasts, 13,16 –21 to modulate integrin expression in keratinocytes, 22 and to stabilize the extracellular matrix. 23 Copper chelation delays wound healing, 24 whereas its addition accelerates wound healing. 24 –26 Copper has potent wide-spectrum antimicrobial properties. 27
Copper oxide impregnated dressings (hereafter termed COD) are cleared by the Food and Drug Administration (FDA) and other regulatory bodies for managing acute and chronic wounds, such as DFU. Their safety and antimicrobial efficacy are well-established, and their ability to promote healing in difficult, stagnated chronic wounds across various patient etiologies was proven in multiple studies. 28 –36 Their successful use throughout the whole wound healing process has been described. 34
COD are single-use dressings with a highly absorbent layer and one or two nonadherent outer layers, all infused with copper oxide microparticles. Even in wounds with necrotic tissue, ischemia, and exposed bone, COD stimulate granulation tissue formation, 28 –30,33 similar to NPWT. This observation led us to conduct a noninferiority randomized controlled trial (RCT) comparing the efficacy and convenience of COD versus NPWT in managing diabetic foot wound (DFW).
INNOVATION
NPWT is an effective treatment of DFWs and other hard-to-heal wounds. However, NPWT is notorious for its high cost, inconvenience, and difficult application, especially in unfavorable topographic locations, which often preclude its use. Our study is the first study to suggest substituting the expensive and inconvenient NPWT with a simple wound dressing that has wound healing stimulating capabilities (angiogenesis, granulation tissue induction, and epithelialization) in addition to antimicrobial protection. COD may thus be considered the first line of treatment for DFWs when NPWT seems indicated.
CLINICAL PROBLEM ADDRESSED
DFWs have a profound impact on patients, affecting their physical, emotional, and social well-being. Poor blood circulation and microangiopathy and general medical conditions prolong healing in patients with DFWs. Diabetes is a worldwide leading cause of lower-limb amputations. Treating DFWs and associated complications is expensive, due to prolonged hospitalizations, frequent medical visits then after, and utilization of advanced wound care methods and dressings.
MATERIALS AND METHODS
Trial design
This single-center study was conducted at Rambam Health Care Campus following approval from the Rambam Health Care Ethics Committee (Approval ID: #0540-20-RMB). The study adhered to international ethical and clinical guidelines, including the Declaration of Helsinki and Good Clinical Practice standards and CONSORT guidelines. The trial protocol designed as a noninferiority RCT was detailed and registered on ClinicalTrials.gov (Identifier: NCT05215730). All patients were recovering from DFI that required extensive debridement surgery and/or partial foot amputation, resulting in wounds necessitating NPWT for closure. In accordance with the pre-study clinical protocol and inclusion criteria, only patients without overt signs of infection or if there was residual infection it was under control and in the process of resolving as evidenced by laboratory tests (within one day before study commencement for in-house patients) and clinical judgment were included in the study. Patients with wounds involving plantar aspects with pressure areas necessitating off-loading were not included in the trial.
The RCT consisted of two arms as follows (Fig. 1): The control group was treated with NPWT Arm, followed by Aquacel® Extra™ (ConvaTec, UK) or Granuflex® (ConvaTec) dressings. The test group was treated throughout the study with the COD (Fig. 2, Copper Arm). Participants meeting the inclusion criteria (detailed at ClinicalTrials.gov, NCT05215730) were thoroughly informed about the study, including its objectives, potential risks, and discomforts. Upon agreeing to participate, written informed consent was obtained using an institutional review board–approved consent form. Their medical history, demographic information, and current medications were then recorded during the initial visit (visit 1). Electronic laboratory notebook was not used. The wound was photographed and measured, and a blood sample and X-ray were taken (Supplementary Figure S1). Patients were then randomly assigned to the COD Arm or NPWT Arm. The wound was treated with either the NPWT apparatus (V.A.C.® [3M, UK], VENTURI® [Talley, UK], or extriCARETM [Alleva Medical, China]) based on the patient’s insurance or COD (MedCu Technologies Ltd.). Patients or caregivers were provided with the assigned treatment product for home application. The patients were examined one week later (visit 2) and then after every two weeks for a total of 8 visits (overall 13 weeks).
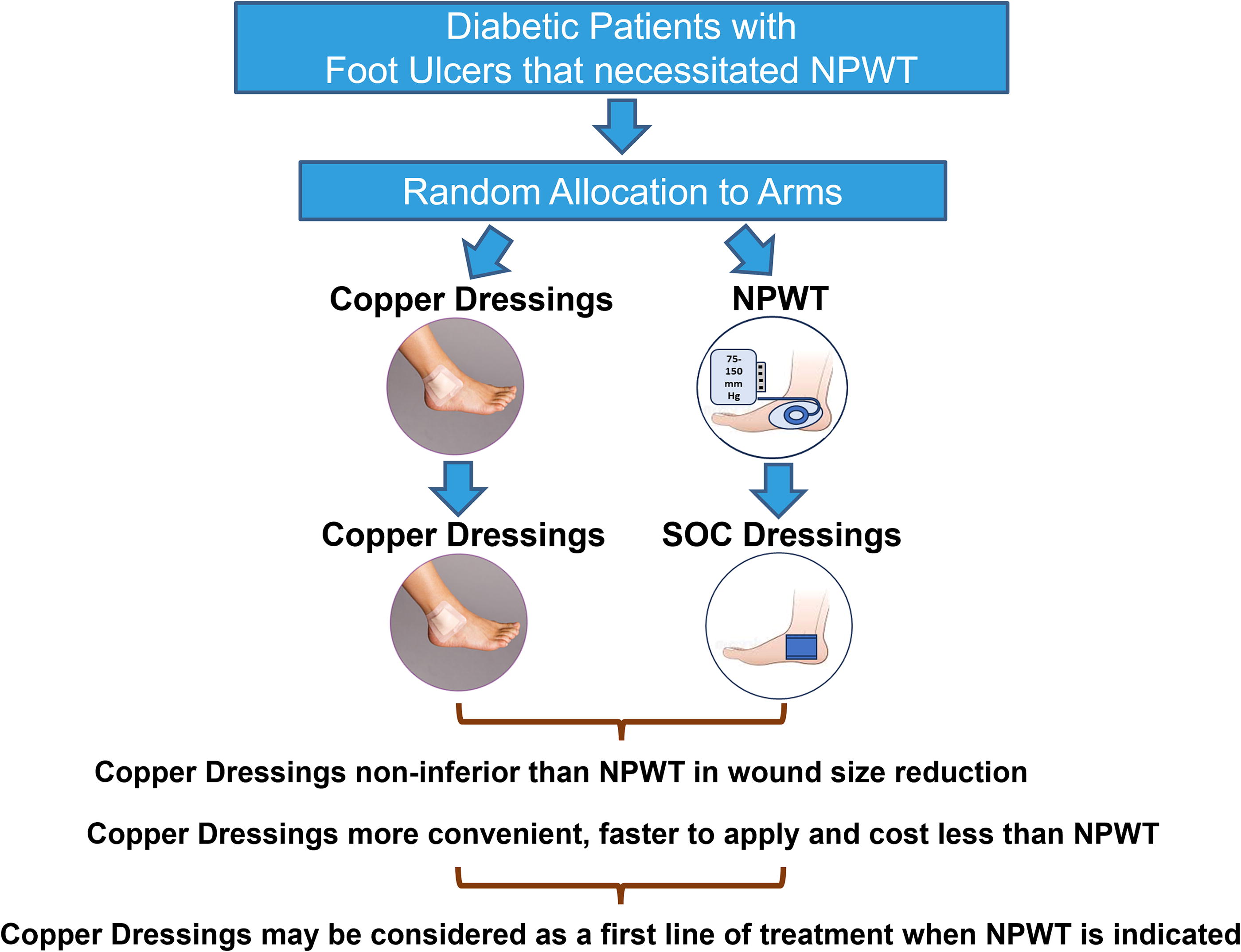
Summary graphic illustration.
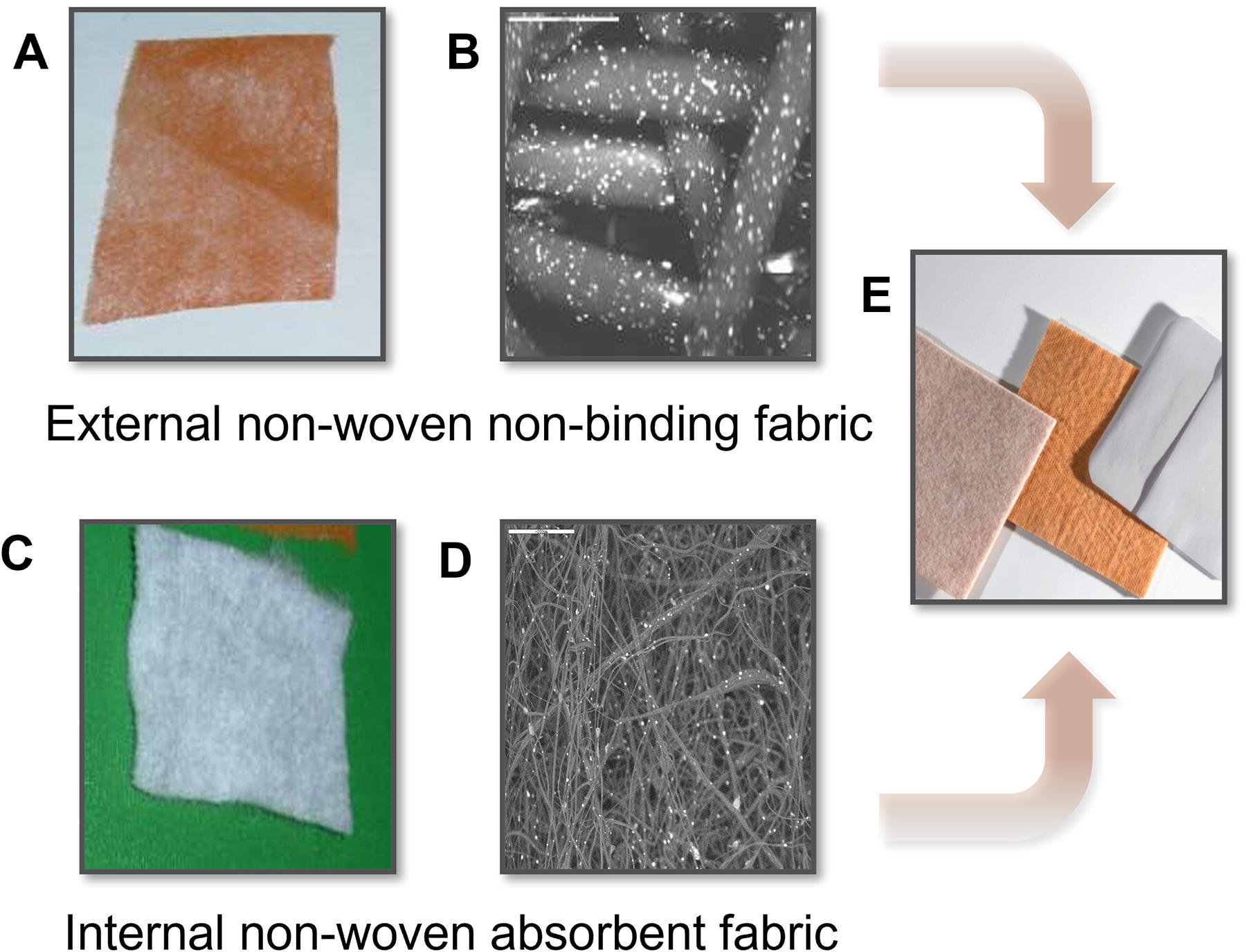
General description of the COD. The COD are composed of one or two nonbinding nonwoven orange polypropylene layers (
NPWT was administered twice weekly at home by a wound nurse, with pressures between 75 and 150 mm Hg. Caregivers were trained to change COD weekly or more often if needed due to high exudation. Caregivers reported any signs of wound deterioration or suspected infection to the research coordinator and principal investigator.
During visits 2–8, updates on the patient’s condition, pain, and medication changes were recorded. The wound was assessed and photographed with the Tissue Analytics app (TA, Net Health, USA). Temperature and vital signs were taken as needed. Aquacel Extra or Granuflex was used when NPWT was discontinued. Blood samples were taken during visits 3 and 5 and at the last visit.
Treatment was halted in case of treatment failure, adverse events (AEs), wound infection, and need for surgical treatment. AEs were assessed and graded by the investigators and recorded in the patients’ case report form (CRF) throughout the study periods, including during the screening and follow-up phases. An AE was considered as any adverse change from the subject baseline condition, whether or not considered investigational product related. AEs were reported in accordance with the Israeli Ministry of Health regulatory requirements. Each AE was reviewed and updated at each subsequent visit. Serum copper levels were assessed at the beginning of the study in all patients and at the termination of the study for the COD arm. Patients were monitored for 2–4 weeks of follow-up visits after treatment cessation.
The primary end point was wound size reduction. Secondary end points included assessment of wound closure rate, granulation tissue formation, reduction in necrotic and fibrin tissue, patient and caregiver convenience, application times, pain levels, infection rates, AEs, and treatment costs.
Sample size calculation
Sample size calculation was based on demonstrating noninferiority of COD to NPWT with a 20% margin. With 30 patients per group, a one-sided t-test could achieve 80% power to refute the null hypothesis of noninferiority. 37,38 Therefore, 60 patients would be randomized into the two treatment arms (1:1 ratio). An interim analysis was planned when at least 15 subjects in each group have completed the study. The interim analysis purpose was to estimate the standard deviation of the difference in mean percentage of wound closure between arms and recalculate the sample size if necessary.
Randomization
Randomization was conducted only after patient eligibility for the study was confirmed and informed consent was obtained. Security-sealed opaque envelopes were sequentially numbered from 1 to 60, corresponding to the patient’s study ID. The study IDs were randomly assigned to either the NPWT or COD group using a computer-based randomization tool (https://www.randomizer.org/), ensuring a 1:1 allocation ratio across the 60 study slots.
The group assignments were not stratified based on potential confounders, such as wound size or patient age. Each envelope contained a slip of paper indicating the group assignment. The sealed envelopes were opened by the investigator in the presence of the patients only after they had signed the informed consent form and before any study-related procedures began.
This process ensured that neither the patients nor the caregivers were aware of the group assignments until the point of envelope opening, maintaining allocation concealment and reducing the potential for bias.
Evaluations, photographs, and measurements
Wound measurements and condition were assessed using the TA 3D Wound Imaging System app, recognized by the U.S. FDA for its breakthrough status. This mobile app enables precise, automatic wound measurements without manual tracing and of course blinded to the group arm. Data included wound location, dimensions (length, width, perimeter, surface area, depth), and tissue types (necrosis, granulation, fibrin). Medical personnel also conducted backup measurements using appropriate wound measurement rulers. Both the width and the depth of the wounds were measured and recorded in the patient CRF. The data obtained and recorded by the physicians were overall similar to that obtained by the TA 3D Imaging System. However, it was not blinded. Therefore, we treated the measurements collected by physicians as backup data only and exclusively analyzed the blinded data from the 3D imaging system to ensure confidentiality and eliminate bias in data collection.
The wound size was calculated by the following formula: % wound size = (wound area at given visit/wound area at Visit 1) × 100. Complete wound closure was defined by the appearance of closed wound in combination with the absence of any staining or signs of secretion on the dressings. Physicians assessed wound exudate using a 3-score grading system as follows: 1 for minimal/no exudate, 2 for regular discharge, and 3 for high exudate and 1 for serous, 2 for serous-sanguineous, and 3 for purulent. Patient-reported pain and convenience were measured using visual analog scores (VAS) on a 10-point scale, with 0 indicating no pain/inconvenience and 10 indicating extreme pain/inconvenience. Caregiver feedback on convenience and application time was also collected at study end using a similar VAS 10-point scale.
We analyzed and compared the costs of treatment between the two Arms based on ambulatory treatment. The cost estimation for the COD Arm included dressings and home nurse visits for changes and assessments, averaging 1.5 dressings per week. For the NPWT Arm, costs involved renting the NPWT device, with the rental fee covering twice-weekly home nurse visits.
Statistical analysis
t-Test, Pearson Chi-square, or Fisher’s Exact tests (as appropriate) were applied to examine differences between the study groups’ demographic data and parameters.
t-Test and Wilcoxon tests were applied for testing the statistical significance of the difference in percentage of wound closure between the study groups per each visit. Noninferiority method, using t-test, was used to analyze the relative change from baseline of wound area per the last two visits. Analysis of variance with adjustments (analysis of covariance [ANCOVA]) tested differences between wound size of the study groups at the end of the study, adjusting for the following confounders: gender, age, body mass index (BMI), diabetes, and smoking.
Secondary outcomes were analyzed using statistical tests as appropriate: the wound closure rates were analyzed by Pearson Chi-square. The Cox model compared Kaplan–Meier curves for time to wound closure, adjusting for possible covariates. The two-sample t-test or Wilcoxon Mann–Whitney rank sum test for independent samples assessed differences in granulation tissue percentage and quality, necrotic and fibrin tissue percentage, and pain and convenience scores between arms. The percentage of subjects with complete wound closure was calculated with 95% confidence interval (CI) within each treatment arm. Pearson Chi-square test or Fisher’s Exact test evaluated differences in infection episodes and complete wound closure rates between arms.
All tests were two tailed, and a p value of 5% or less was considered statistically significant. The data shown are mean ± standard error unless otherwise specified and were analyzed using SAS® version 9.4 (SAS Institute, USA).
RESULTS
Between July 2021 and July 2023, 339 patients with diabetes with wounds were considered for participation in the study (CONSORT Chart, Supplementary Figure S2). Two-hundred and ninety three patients did not meet the inclusion criteria (e.g., wound was not appropriate for NPWT, unacceptable vascular perfusion, participation in another study, and so on) or the patient did not agree to participate in the study. Forty-six patients were included in the trial. The first patient was enrolled on July 28, 2021, and the last patient exited the study on August 28, 2023. All patients had good perfusion or had undergone successful vascular intervention before the study commencement, in accordance with the study inclusion criteria. Baseline characteristics and wound measurements were performed before randomization. Twenty-three patients were randomly allocated to each arm. Forty-one patients had type 2 diabetes (89%), and 5 had type 1 diabetes (11%).
Baseline characteristics showed no statistical differences between the groups, including in vascular perfusion (Table 1). At the study onset, wound parameters were not significantly different, although mean wound size and perimeter in the COD Arm were ∼41% (p = 0.25; Table 2) and ∼26% (p = 0.19) larger, respectively, than in the NPWT Arm, based on TA measurements. Similarly, treating personnel found that wounds in the COD Arm were ∼18% deeper (p = 0.24) than in the NPWT Arm (Table 2, initial depth). There were also no statistically significant differences between the groups in the number and percentage of exposed bones, muscles, or tendons (Table 2). More patients dropped from the NPWT Arm than the COD Arm (7 vs. 1). Reasons for NPWT Arm dropouts included two wound complications requiring surgery, two patients who refused to continue with the NPWT, two for whom the NPWT caused complications in another wound, and one unrelated death. NPWT was used for 46.9 ± 6.03 days on average, excluding dropouts. The single dropout in the COD Arm was due to cellulitis requiring hospitalization.
Baseline characteristics of patients
ABI-DP/TP, ankle-brachial index dorsalis pedis/tibialis posterior arteries; BMI, body mass index; COD, copper oxide impregnated dressings; HbA1c, hemoglobin A1c; SE, standard error.
Wound parameters at the commencement of the study
Measured by the Tissue Analytics app.
Measurements with depth gauge.
Pearson Chi-squared test for three categories.
NPWT, negative pressure wound therapy.
Primary outcome
The primary end point was the reduction in wound size, aiming to show noninferiority with a 20% slower healing margin. In effect, the COD was associated with faster wound size reduction compared with NPWT. Interim analysis conducted when 40 patients concluded the study showed that the primary end point of demonstrating noninferiority was achieved (p < 0.01). Based on the study protocol and interim analysis showing that the 20% noninferiority margin was achieved (p < 0.01), the recruitment of patients was stopped and the study was concluded after the 6 ongoing patients completed the study.
Figure 3 shows the percent of the wound size per patient per visit in each arm. As detailed in Table 3, there were no differences between each arm in the relative change from baseline in the wound size per visit. Similar results were obtained when nonparametric analyses (Wilcoxon tests) were conducted (data not shown). Representative cases of wound closure in the COD arm are shown in Fig. 4, with all patient wounds depicted in Supplementary Figure S3. To account for the impact of dropouts, which were significantly higher in the NPWT arm (7 vs. 1), a Last Observed Carry Forward test was conducted. This test takes into account the patient that dropped out from the trial and the patients in whom the wounds were closed during the trial. It revealed that the COD arm achieved a statistically significant superior result compared with NPWT. The mean wound size at the end of the trial (visit 8) was 12.81 ± 4.34 (CI [4.3, 21.3]) for COD and 36.58 ± 9.53 (CI [17.9, 55.3]) for NPWT (t-test, p = 0.03). Adjusting for other confounders, which included gender, age, BMI, diabetes, and smoking, a comparison showed higher wound size reduction for COD (91.23% ± 13.7) compared with NPWT (68.32% ± 12.9) (ANCOVA, p = 0.04).
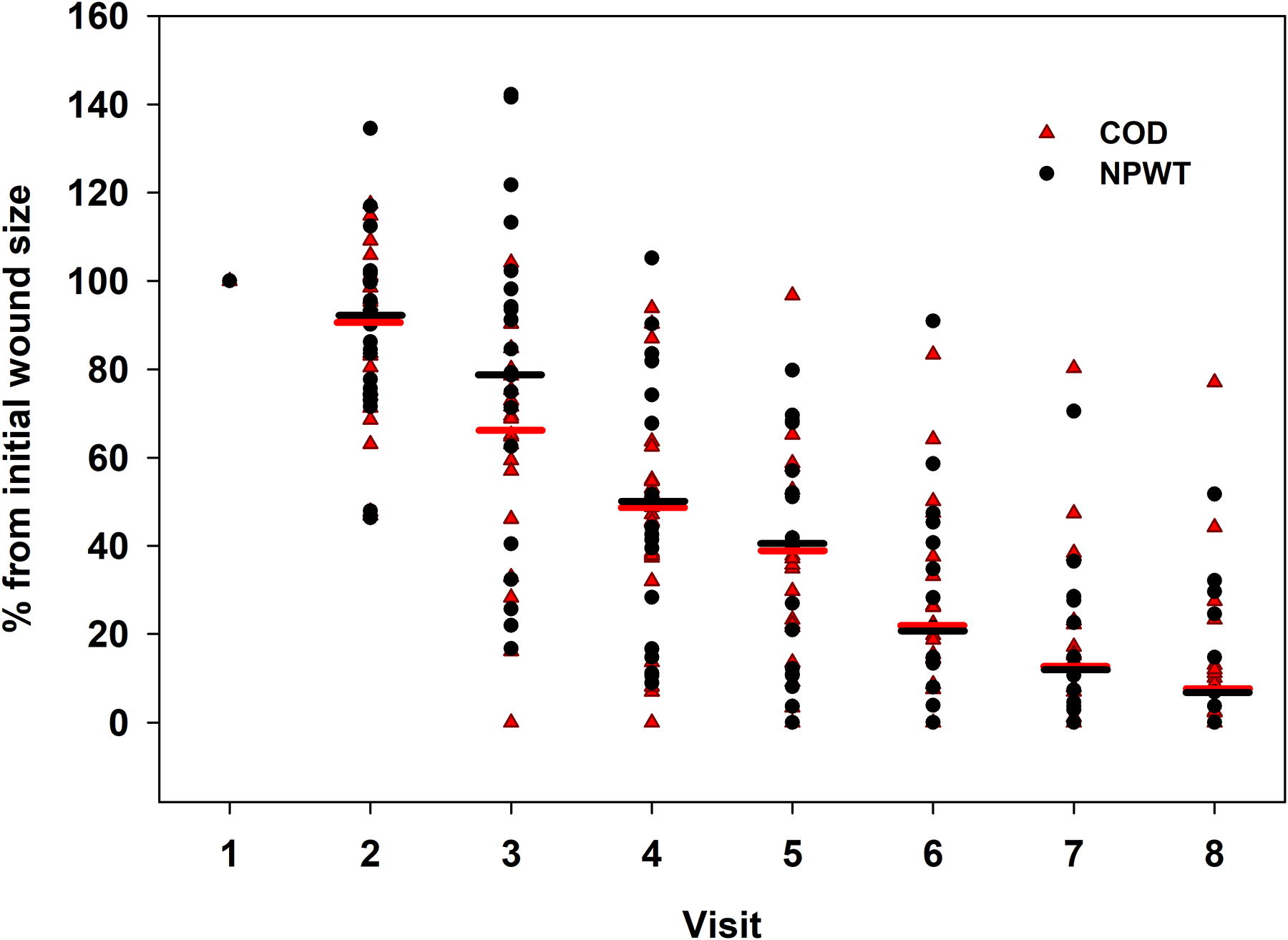
Wound size reduction through the trial. The size of the wound was determined blindly by the Tissue Analytics software. The wound size at each visit is presented as the percent of the initial wound size. Similar reduction trends were observed in both arms, with no statistically significant differences between arms in each visit (p > 0.05 for the difference in the percentage of wound closure between study groups at each visit, assessed using t-tests and Wilcoxon tests, as well as for the noninferiority analysis of the relative change from baseline in wound area over the last two visits using a t-test). The horizontal lines represent the mean of the data at each visit.
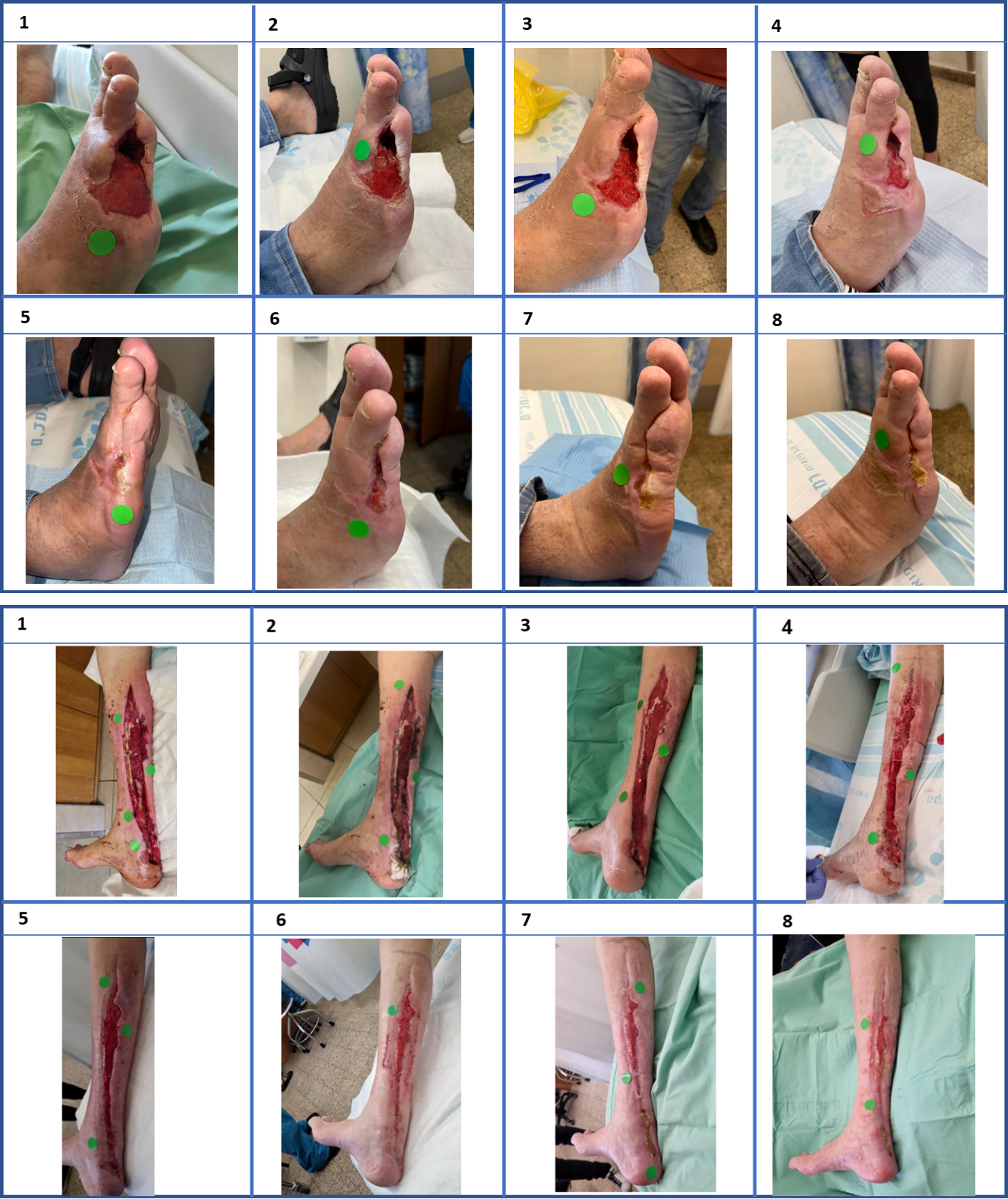
Two representative wounds that were treated with COD. Pictures were taken at each 2 weeks apart visit. The number of the visit is indicated. The green round circles served for size and color reference to the Tissue Analytics wound measurement software used.
Relative change from baseline in wound size
The data presented in this table do not include the data collected from the patients that dropped from the trial.
t-Tests.
Secondary outcomes
Wound closure rates were 48% (11/23) in the COD arm and 35% (8/23) in the NPWT arm. Although more wounds closed in the COD arm, the difference was not statistically significant (p = 0.37). Figure 5 shows that the percentage of wounds closed was higher and earlier in the COD arm, but it did not reach statistical significance (p = 0.73), also when adjusted for confounders (p = 0.78).
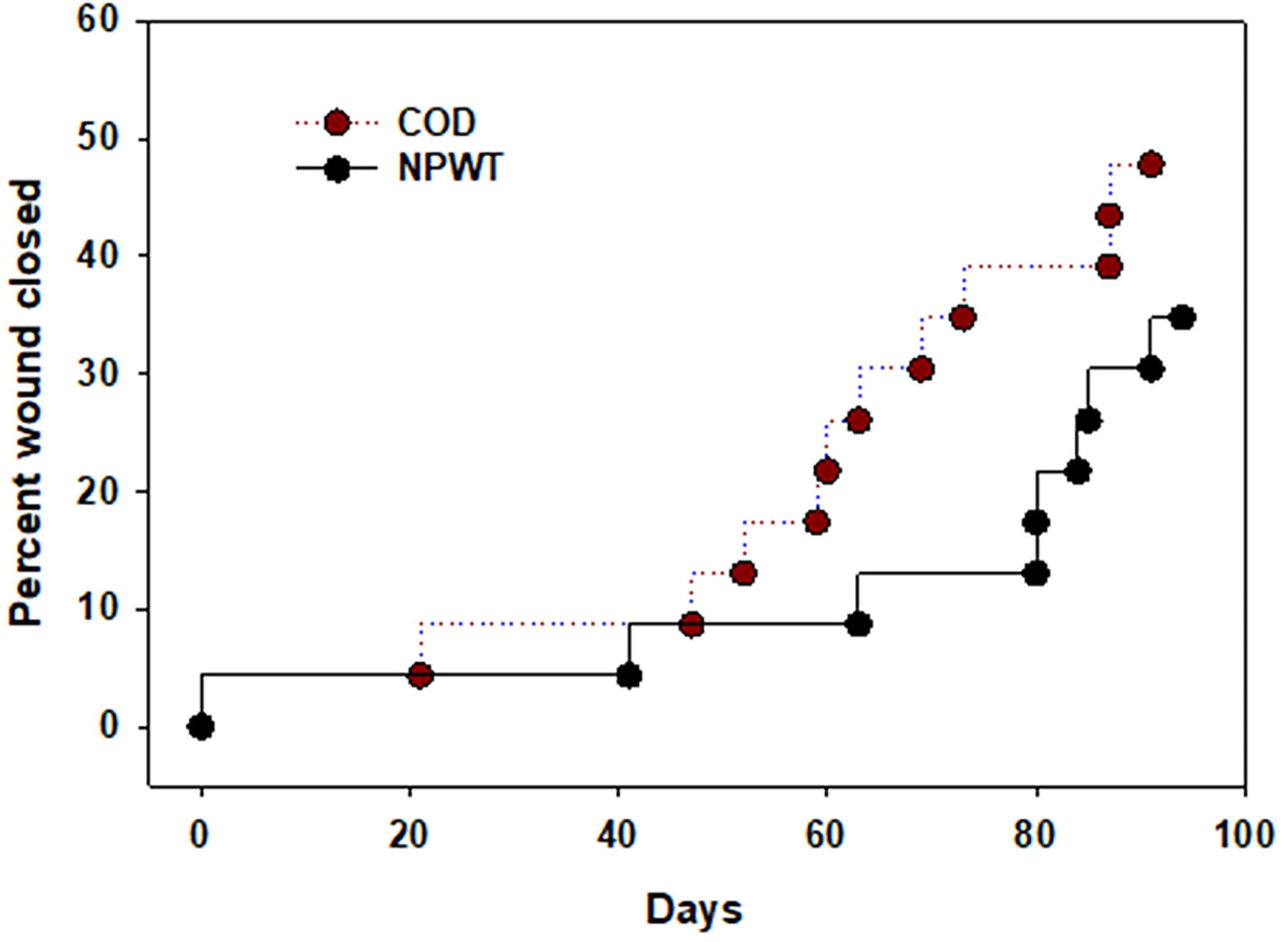
Kaplan–Meier wound closure estimates showing the percent of wound closure through the trial (p > 0.05 per Pearson Chi-square test).
There were no significant differences between the two arms in terms of the percentage and quality of granulation tissue, necrotic tissue, and fibrin tissue throughout the study (p > 0.05). The wound exudate amount and quality were also similar between the arms (p > 0.05). Although patients in the COD arm reported less pain (VAS 1.3 vs. 2.24), this was not statistically significant (p = 0.16). However, COD treatment was more convenient for both patients (VAS 8.37 vs. 6.14, p < 0.001; Fig. 6A) and caregivers (VAS 8.45 vs. 6.1, p = 0.003; Fig. 6B), and application was faster (p < 0.001; Fig. 6C). There were no significant differences in AEs (Table 4). In COD Arm, there were 7 serious adverse event (SAE), one of them possibly related to the study treatment. The patient was hospitalized due to wound infection and cellulitis. In the NPWT Arm, there were 8 SAE, two of them probably related to the study treatment as follows: One patient was hospitalized due to an ischemic wound that became infected and necrotic and necessitated amputation. Another patient was hospitalized following amputation of the non-study wound, very close to the NPWT-treated wound. One SAE possibly related to the study treatment was worsening of the wound condition, appearance of necrotic tissue, and eventually amputation.
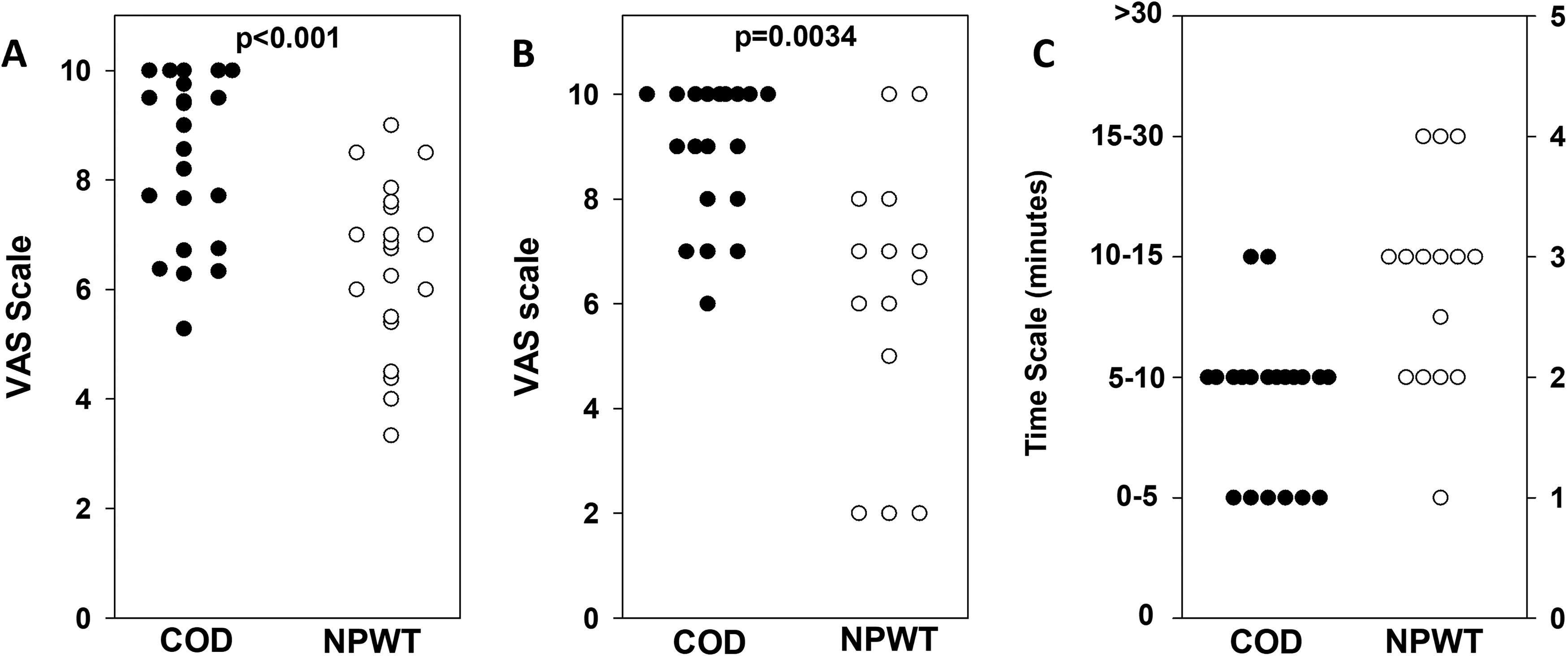
Convenience of use as scored by the patients (
Number and classification of adverse events
AE, adverse event.
There were 84 and 49 AEs in the COD and NPWT arms, respectively (Table 4). Eight and nine were classified as severe (COD and NPWT arms, respectively) but were not attributed definitely to the device test itself. All other AEs were mostly mild or moderate and unrelated to the study or test items. There were also no significant differences in the number of wound infections (6 vs. 3 in the NPWT and COD, respectively [p = 0.26]). All six infections in the NPWT arm were rated as superficial (grade 1 in a scale of 1 [superficial] to 5 [severe]). In the COD arm, the infections were rated as 1, 2, and 4, respectively. All infections were resolved within a week by administration of systemic antibiotics.
There were no significant differences in serum copper concentrations between the beginning and end of the trial in either arm (COD: 134.8 ± 7.2 vs. 121.7 ± 7.2 µg/mL, p = 0.2; NPWT: 142.1 ± 10.9 vs. 123.3 ± 8.5 µg/mL, p = 0.19) or between the arms at any point (beginning: 142.1 ± 10.9 vs. 134.8 ± 7.2 µg/mL, p = 0.58; end: 123.3 ± 8.5 vs. 121.7 ± 7.2 µg/mL, p = 0.89).
The average and the median duration of using the NPWT apparatus was 46.9 ± 6.03 days and 43 days, respectively, before switching to using standard of care wound dressings. We compared the costs (including labor) associated with NPWT and COD over this period, based on local Israeli quotes. The weekly cost of COD was approximately $70, whereas NPWT was around $500, making NPWT roughly 7 times more expensive. Over 47 days, the estimated treatment cost per patient was approximately $3,360 for NPWT and $470 for COD (Table 5).
Cost estimation analysis for negative pressure wound therapy versus copper oxide impregnated dressings (in U.S. dollars)
Values in bold are the final cost and percent of expenditure based on the calculations detailed in the other columns.
The average duration use of the NPWT before switching to Standard of Care (SOC) dressings was 46.9 days. The comparison is thus for 47 days of use.
Average of 1.5 dressing changes per week.
In Israel, the NPWT apparatus is rented, and its cost includes the nurse home visits to apply the NPWT.
DISCUSSION
Our RCT showed that DFW management with COD was noninferior to NPWT in reducing wound size with statistical significance (p < 0.01) according to the predeclared statistical method of analysis. Nevertheless, a Last Observed Carry Forward analysis, considering dropouts and wound closures, showed that COD outperformed NPWT significantly (p = 0.03) in wound size reduction. COD treatment was linked with greater convenience for both patients (p < 0.001) and caregivers (p = 0.003) and required less application time (p < 0.001). In addition, COD’s cost was one-seventh that of NPWT.
The objective of the study was to demonstrate the noninferiority of the study treatment (COD) compared with the standard of care (NPWT), with a 20% margin. The sample size calculation, as outlined in the study protocol (ClinicalTrials.gov; ID NCT05215730: Comparison of Wound Healing Between MedCu Dressings With Copper Oxide and Negative Pressure Wound Therapy Treatment), was based on an assumed zero difference in the percentage of wound closure between the two groups. Initially, the sample size justification was as follows: with 30 participants per group, a two-group, one-sided 0.05 t-test would have 80% power to reject the null hypothesis of noninferiority (i.e., a difference in means of 20% or more) in favor of the alternative hypothesis that the treatment is inferior, assuming a mean difference of 0 and a common standard deviation of 30. An interim analysis was planned after 15 subjects per group had completed the study to estimate the standard deviation of the difference in mean wound closure percentage and adjust the sample size if needed. The interim analysis confirmed noninferiority between the treatments, leading to the conclusion that the number of completed participants was sufficient. As a result, the study was concluded after the 6 ongoing patients completed the study.
The main beneficial effect of NPWT, compared with other treatments, is enhanced formation of granulation tissue and reduced healing time, leading to high adaptation with $2.80 billion in sales (https://www.globaldata.com/store/report/npwt-devices-and-accessories-devices-market-analysis/). Nonetheless, the evidence in favor of NPWT is at times equivocal. Meta-analysis of the percent of wound closure achieved with NPWT showed that 44.2% and 54.7% of postoperative and diabetic wounds, respectively, do not heal, 7 and ∼3.5% of these NPWT-treated wounds result eventually in amputations. 7 Some of the shortcomings of NPWT are their high cost and complicated and prolonged application requiring specialized personnel training. 6 These factors contribute to an enormous cost burden for health care system providers and consume valuable resources. In addition, patients often find NPWT uncomfortable, since it necessitates being constantly connected to a vacuum machine and can be painful, contributing to patient noncompliance. Furthermore, in many instances, application of NPWT requires hospitalization, at least during the initial treatment sessions. Although it is claimed that NPWT sucks bacteria out of the wound, NPWT is not considered to have an antimicrobial effect and wound infection is a contraindication for its use. 7 Furthermore, due to its cost and complexity, NPWT is not affordable in developing countries. In our cost evaluation, we did not include the expense of the 3-day hospitalization required for initiating NPWT, as this is standard practice in our hospital for the first NPWT session and may not be applicable in other health care settings. The inclusion of this hospitalization nearly doubles the total cost of NPWT, reducing the cost of COD treatment to approximately 8% of the NPWT cost.
Similar hospitalization requirements for NPWT initiation may also be standard in other health care systems. In addition, in some settings patients are required to purchase or rent the NPWT apparatus. For example, a retrospective cost analysis performed at the University of Chicago Medical Center between 1999 and 2014 found that the rental cost of a portable vacuum machine and related equipment was $119 per day of treatment. 39 These factors support our conclusion that the substantial cost savings of COD compared with NPWT extend beyond outpatient care in Israel and may be relevant in a variety of health care contexts.
Although NPWT is commonly used to treat complex large wounds, we observed at least similar results with COD in terms of wound size reduction and better convenience and preference by the nursing team of COD over NPWT. We therefore decided to compare NPWT to COD in a noninferiority RCT study, with the primary end point being reduction of wound size. We set the limit of comparison for statistical analysis on 20% lower healing rate. The rational of this number is that since NPWT is expensive and inconvenient, the patient and caregiver would prefer to use COD for 5 weeks than NPWT for 4 weeks to get the same effect in wound reduction size.
The study was conducted on patients’ diabetic foot recovering from infection after debridement and/or minor amputation surgery to get a relatively homogenous group of wounds in a very challenging population. This population is characterized by wounds that are difficult to heal and prone to complications. The patients involved in the study also suffered from many underlining clinical conditions and experienced many AEs during the trial that were unrelated to the devices being studied. For example, patients 16 and 23 in the COD Arm suffered each from 13 AEs unrelated to the COD. We did not find any correlation between the number of AEs and the wound closure. For example, patient 16 closed the wound after 59 days (visit 6) despite the multiple AEs he experienced.
Although pain was low in both arms, this can be attributed to the neuropathy of the patients. Nevertheless, convenience was statistically significantly better in the COD Arm. Newer NPWT machines emphasize convenience but are much more expensive. The machines used in the current trial were portable NPWT devices of previous generations, and although they are less expensive than the newer machines, treatment costs were approximately seven times that of COD treatment (the calculated prices are based on outpatient treatment costs in Israel, including labor).
The limitation of our study is the relatively small number of participants and the relatively high number of patients that dropout, especially from the NPWT Arm (7 vs. 1), which may have influenced the study results. Two patients discontinued NPWT due to inconvenience, and five experienced wound deterioration. In contrast, only one patient in the COD arm discontinued treatment due to wound deterioration. The difference in the dropout numbers between both arms point to the advantage of the COD treatment. The drawbacks due to the small number of patients are counterbalanced by the homogenous group of patients with DFWs, all recovering from infectious episodes and surgery. In addition, not only the results demonstrated a statistically significant noninferiority between both arms based on the predetermined noninferiority calculation method but also further analysis using a Last Observed Carry Forward test further supports our conclusion that COD may be used as the first line of treatment in patients with DFW when NPWT is considered.
Another limitation of the study was that the sample size was calculated only for the primary end point. From a statistical point of view, the secondary end points were not formally powered calculated. We therefore had not conducted multiple comparison analyses. The nonformal analyses for secondary end points are part of the limitations of the study because of the relatively small sample size of the study. Our study was also a single-center and region-specific (Israel) study. Further multisite studies should be carried out to support the applicability and relevance of our finding to other health care systems and populations.
The conflict of interest of the primary investigator (E.M.) and the last two authors (T.R. and G.B.) due to their affiliation with MedCu, the COD manufacturer, may be regarded as an inherent weakness of the study. This potential conflict of interests was mitigated by blinded and objective automated software program (TA) measurement of the wound size and granulation, necrotic and fibrin tissue percentage and quality, and by statistical analyses of the data performed by an independent biostatistician company (Medistat).
Key Findings
COD, while being noninferior to NPWT in wound size of DFW, were faster to apply, were associated with higher convenience to both patients and caregivers, and were significantly less costly than NPWT.
COD may be the first line of treatment in patients with DFW when NPWT is considered, as well as in cases where NPWT cannot be applied.
Using COD first is expected to reduce health costs, improve convenience, and increase compliance without compromising the final outcome, also when extrapolating the study outcome to other circumstances when NPWT is indicated.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors would like to thank the nursing staff at the departments and outpatient clinic of the Division of Orthopedics at Rambam Health Care Campus, Haifa, Israel, for their devoted treatment and for taking care of the patients participating in the study. The study was funded by MedCu Technologies Ltd., the company that developed the COD.
AUTHORS’ CONTRIBUTIONS
E.M., M.S.P., and G.B. designed the clinical trial protocol. E.M., J.D., T.I., and I.K. gathered the data. E.M., T.R., M.S.P., and G.B. analyzed the data, contributed to the discussion, wrote the first draft of the article, and reviewed and edited the article. All authors had access to the data, and all authors approved the final version of the article.
AUTHOR DISCLOSURE AND GHOSTWRITING
G.B. is the Chief Scientist of MedCu Technologies. T.R. is an employee of MedCu Technologies. E.M. and M.S.P. are medical consultants of MedCu Technologies. J.D., T.I., and I.K. do not have any conflict of interests. There was no ghostwriting involved. Independent compensated statistical analyses were performed by Dr. Gil Harari, from Medistat (![]() ).
).
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.