
Abstract
Significance:
Negative pressure wound therapy (NPWT) was introduced in clinical practice in the early 1990s and has become widely used to manage wounds in inpatient and outpatient care.
Recent Advances:
Evolutions of the initial technology include the development of new dressing interfaces and tubing configurations, the addition of instillation to improve cleansing, and various changes in design to improve portability. Research has been conducted to understand mechanisms of action and to demonstrate clinical utility. NPWT has been suggested as a valuable approach for various complex and/or nonhealing wounds, and recommendations for its use have emerged in several guidelines.
Future Directions:
The evidence, composed of a combination of randomized controlled trials, case series, cohort studies, real-world evidence, systematic reviews, meta-analyses, and expert opinion, is heterogeneous and still building. This special mini forum issue presents the current state of the science for NPWT and new studies providing insights on some innovative ways clinicians use this technology to help improve outcomes in a variety of wound types.

INTRODUCTION
Negative pressure wound therapy (NPWT) applies subatmospheric pressure to the wound, which helps reduce edema and promotes perfusion and granulation tissue formation. The first recorded application of this concept occurred in the 19th century and evolved throughout the 20th century. 1 The method became broadly accepted following publications by Morykwas et al. 2,3 who described their system including a polyurethane foam and the distribution of negative pressure by intermittence or continuous suction through a machine. Since then, various modalities have been developed and commercialized, including negative pressure therapy (NPT) for the open abdomen and for closed incisions, as well as NPWT with instillation and dwell (NPWTi-d). There are now over 100 uses identified for NPWT, 4 and the applications keep expanding. From today’s perspective, the closed incision negative pressure therapy (ciNPT) (introduced in 2006) and NPWTi-d (introduced in 2011) variations on the conventional NPWT technology are of particular importance. These advances have been recently reviewed in an update on NPWT for clinicians and outpatient care givers. 5 ciNPT can be applied immediately postoperatively over closed incisions with the aim of helping to prevent surgical site infections (SSIs) and other complications, such as seroma and hematoma. Numerous studies 6 –9 and a meta-analysis 10 have reported improved outcomes with this technology (using various commercially available systems), such as lower rates of infection and complications compared with standard of care, while also reporting a higher frequency of comorbidities associated with high risk of complications in the ciNPT group. 8 However, many studies have been underpowered, and the evidence is not considered strong. 5,8,9,11,12 At this time, consensus recommendations made for the most appropriate use of ciNPT include patients with one or more comorbidities or patients with a surgical incision at high risk for developing SSIs. 5 In the case of NPWTi-d, controlled wound cleansing through instillation of topical wound solutions is possible without causing a burden on the patient or nursing staff, and it has been used successfully for the management of acute wound infections in conjunction with systemic antibiotic therapy after surgical debridement 13,14 and in the debridement of fibrinous leg ulcers. 15 NPWTi-d can be used with saline or with various topical antiseptic solutions. Saeg et al. have reviewed the evidence and proposed irrigation guidelines for various wound types based on published studies using NPWT and other methods. 16 These recommendations include the use of silver nitrate, polyhexanide, acetic acid, or povidone-iodine, especially for complex wounds; however, the authors acknowledge that the studies included in their evidence review present small sample sizes or specific patient populations and lacked consistency in study design, potentially limiting generalizability. In contrast to those recommendations, the latest update to international consensus guidelines when NPWTi-d is used supports normal saline as the first choice of instilled topical solution and lists the following solutions as also compatible with foam dressings: hypochlorous acid, sodium hypochlorite, acetic acid, and polyhexamethylene biguanide + betaine. 17 The Saeg et al. literature review 16 suggests that NPWTi-d may be more effective at promoting granulation tissue formation than NPWT alone, 18,19 and other authors 15,20 have hypothesized that the mechanical movement of the foam caused by the succession of instillation and suction cycles is the main mechanism of action of NPWTi-d. Another advantage of NPWTi-d is that it reduces aerosolization compared with lavage. 21 These advantages, however, exist in the context of added complexity in the care process and the typical resistance to change, illustrating the challenges of introducing new technologies in health care systems. 5
INNOVATION
This special mini forum issue highlights innovative ways clinicians use NPWT to help improve outcomes and provides an update on the current state of the evidence. Figure 1 illustrates the various applications of NPWT. This issue starts with a review by Miller-Mikolajczyk et al. of the history of NPWT and its evolution over the past 3 decades. Following the first device to be commercialized, additional iterations have been developed over time to improve this treatment modality by addressing various issues observed during use, including delivering consistent negative pressure to the wound site, managing high viscosity exudate, clearing infectious material, dealing with necrotic tissue, reaching adequate drape adhesion while avoiding skin damage, facilitating patient adherence to the therapy, and limiting tissue ingrowth. All components (device, software, tubing, dressing, and sealing drape) have undergone significant advances over time to improve reliability, functionality, and usability, making commercial NPWT an integral and versatile tool for the management of a wide variety of acute and chronic wounds. The article presents a timeline of NPWT development and dives into the technical challenges of delivering NPWT. Another excellent recent review is also available that provides clinical guidance and addresses the use of NPWT in home care or out-of-hospital settings, presented from a European perspective. 5
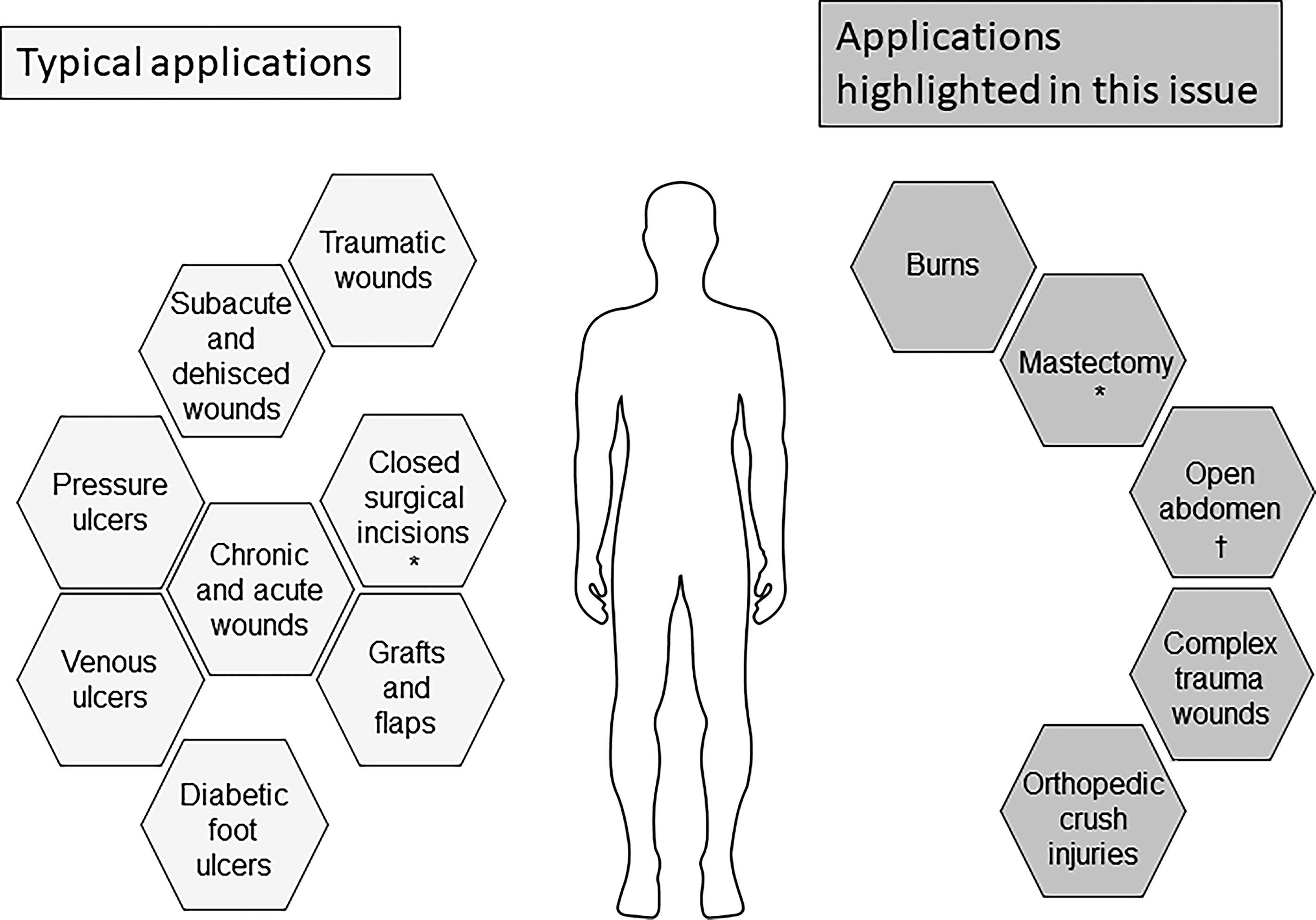
Applications of negative pressure wound therapy, closed incision negative pressure therapy (*), and negative pressure therapy (†).
This general review article is followed by reviews of specific applications. Ottolino reviews the use of NPT on open abdomen wounds. The open abdomen is a validated approach to managing surgical and traumatic pathologies and involves leaving the fascial layer of the abdomen open after a laparotomy for blunt or penetrating trauma with the intention of going back later for definitive repair and closure. Ottolino describes the clinical situations for which the open abdomen approach is preferable or necessary and how various methods can provide temporary closure to protect the abdominal cavity during the process. This review summarizes treatment recommendations; to learn more about classification systems for the open abdomen, a narrative review was recently published by a panel of international experts. 22
In the next article, Nuhiji reviews the management of burns with NPWT and NPWTi-d, which have shown in recent years potential to improve outcomes, although the evidence is still limited (13 studies covering 308 patients). These modalities create a closed, regulated environment for wound management (helping to protect it from external contamination) and facilitate better regulation of the wound conditions while preparing the burn defect to achieve definitive closure. Burn wounds require prompt intervention and rapid closure to limit injury progression, and NPWT/NPWTi-d may provide additional options for the management of these wounds. Of note, severe bleeding has been reported (two case reports) by others in patients receiving NPWT for burn wounds, 23 highlighting that caution should always be used, and proper assessment and preparation of the wound bed as well as monitoring of the treatment are crucial to avoid severe complications.
The article by Fernandez et al. reviews the treatment of patients with complex trauma wounds. These wounds, which can be life- or limb-threatening, often require surgery in a contaminated environment and the use of resuscitation strategies. This article provides insights on how NPWT modalities can offer additional adjunctive tools and fit into the patient management plan. Traditional NPWT, open abdomen NPT, NPWTi-d, and ciNPT can each contribute to the task for these scenarios that are all unique and different and therefore require customization for each case. The literature has, however, reported complications arising from NPWT treatment, specifically in cardiac surgery, 24 and emphasized the importance of protecting exposed organs and blood vessels, 25,26 which can be a specific concern for complex trauma wounds.
Ng’s review on orthopedic crush injuries describes the evolution of surgical principles used to manage these wounds over time, from amputation to increasingly successful limb preservation. The review also includes some examples of the use of NPWT to manage these difficult wounds. This modality can be a useful intermediate step between debridement and final reconstruction by promoting granulation tissue while removing exudate and helping to protect the tissue from contamination, and it has been shown to greatly improve lower limb injury management. Other publications describing the use of NPWT in orthopedic applications have shown benefits in revision knee and hip arthroplasty. 27,28
Additional specific review articles are regularly published on the topic of NPWT. Just in the past year, Silverman et al. 29 have reviewed the mechanism of action on NPWTi-d; Mantyh et al. 30 have reviewed outcomes of ciNPT versus standard of care for surgical site complications in abdominal incisions; Li et al. 31 covered the topic of NPWT for chronic wounds; Pappalardo et al. 32 performed a systematic review on the adjunctive use of NPWT in the management of postoperative spinal wound infections; and Christodoulou et al. 33 published a meta-analysis on the use of NPWT to manage deep sternal wound complications, to list a few examples.
This special issue also contains two original research articles reporting specific studies with NPWT utilization. Hou and Griffin report on the use of NPWT with or without oxidized regenerated cellulose/collagen/silver dressings (OCSO) to treat chronic, nonhealing wounds documented in the U.S. Wound Registry. The results of this retrospective analysis showed positive healing outcomes for these wounds when this form of NPWT was combined with OCSO dressings, providing insights on how the technology can benefit from being combined with specific materials for a given application. This combination allows patients to experience the benefits of OCSO and NPWT together. This combination of products is a good example of how innovative work by wound care specialists to generate new evidence can lead to updates in the Instructions for Use and open up new therapeutic approaches. The a by Hou and Griffin provides a useful larger-scale analysis combining data from 485 patients to report on real-world evidence for this approach. Observational data obtained in a study such as this these do not replace the need for randomized controlled trials (RCTs) but is useful to complement information gained from RCTs. 34 In general, using data from a registry allows to include real-world patients without exclusions based on concomitant medications and comorbidities and provides access to a large sample size, which facilitates subpopulation analyses and better generalizability. 35 This approach of using large patient databases for retrospective analyses has great potential, as it also facilitates the identification of enough cases of emerging applications to start evaluating real-world evidence in the absence of large, randomized trials. The methodology is gaining acceptance, and the Food and Drug Administration issued a draft guidance for industry in December 2023 on the use of real-world evidence to support regulatory decision-making for medical devices. 36
Baker and Pieri retrospectively assessed the use of ciNPT as a modality for mastectomy in 25 patients with or without implant-based breast reconstruction to compare patient-reported outcomes. The modality, now available with wider-coverage foam dressings to apply the benefits of ciNPT to a larger area of surrounding tissues, was well tolerated, and patient satisfaction was high. These surgeons concluded that their results from this small cohort study support continued use at their hospital. This modality (ciNPT) is the topic of a recent systematic review and meta-analysis comparing it with standard of care in the reduction of surgical site complications. 37 The meta-analysis concluded that ciNPT use was associated with statistically significant reduction in surgical site complications, SSIs, seroma, dehiscence, skin necrosis incidence, reduced readmissions, reoperation, and length of stay. The usual limitations of meta-analysis apply to this conclusion since it included a mix of RCTs and observational studies with differences in data reporting and varying levels of quality, but with 84 studies included, the results suggest that ciNPT is a promising modality.
CLOSING REMARKS
From this collection of articles, we learn that NPWT continues to evolve based on the needs reported by the users, and clinicians remain interested in identifying new applications for the most complex wounds they encounter. Figure 2 provides a decision tree to help choose the right type of NPWT. Various iterations of this modality can be used on venous ulcers, diabetic ulcers, pressure injury/ulcers, debrided partial-thickness burns, traumatic wounds, and surgical wounds, providing a versatile tool to manage wounds and closed incisions.
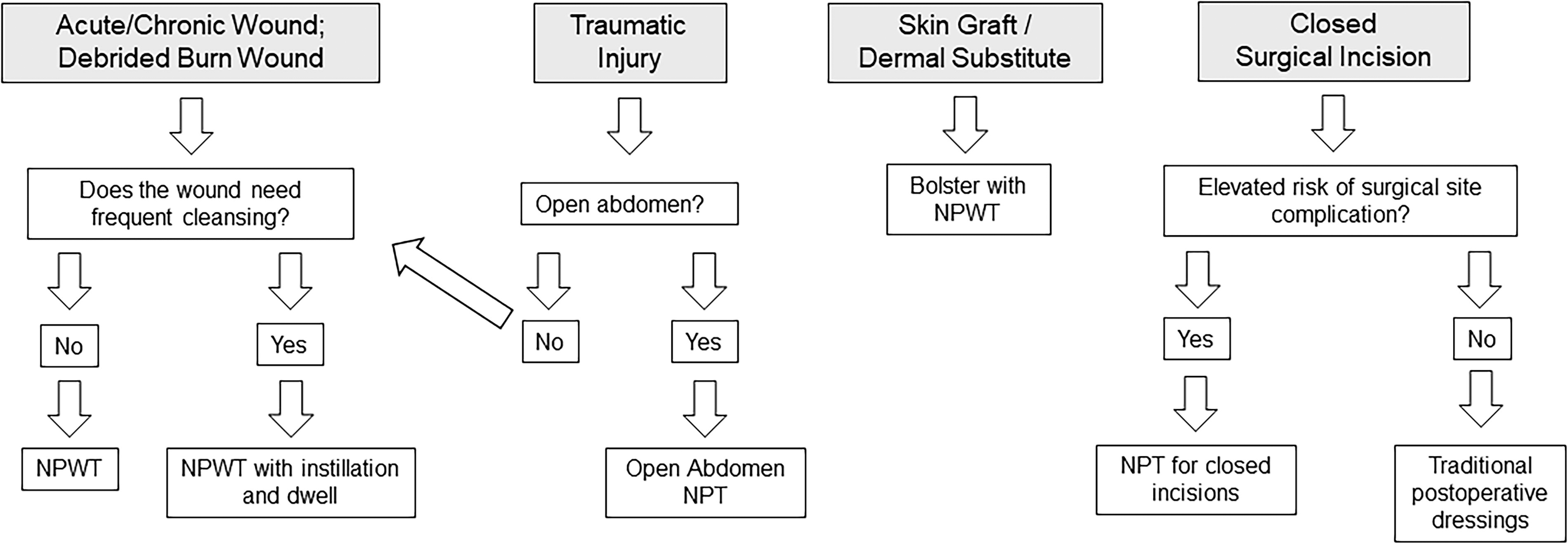
Choosing the right type of negative pressure wound therapy (npwt) and negative pressure therapy (npt).
At this point, various reviews on this technology make mixed recommendations for the use of NPWT: differences in methodology for the inclusion criteria account for the differences in the findings driving the recommendations. In addition, the exact application method, the magnitude of the pressure applied, the frequency of dressing changes, and the overall management of the therapy are all variables that can impact outcomes, and the existing literature does not always include a detailed methodological description, which compromises comparative analysis across studies to reach the best evidence. NPWT is currently the topic of a large number of ongoing clinical studies, according to information available from clinical trial registries, and review updates will be required to include the results from these studies as they become available. As more data become available, it should become possible to better analyze results specifically for the different types of NPWT, the different protocols used with these modalities, and the different outcomes of interest. This will hopefully further inform our understanding of circumstances in which NPWT is most beneficial. We hope this issue triggers your interest and stimulates more ideas and research to study new approaches and innovative ways to treat complex wound cases.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
No funding was received for this article.
AUTHOR DISCLOSURE AND GHOSTWRITING
S.F.B. is an employee of Solventum. No ghost writer was involved in the writing of this article.
ABOUT THE AUTHOR