
Abstract
Objective:
Determine the validity and reliability of the LIMB-Q scales, Function, and Symptoms in patients with chronic lower extremity wounds.
Approach:
Cognitive debriefing interviews with people with current or previous wounds were conducted to examine content validity. Scales were field-tested in an international sample of people with chronic lower extremity wounds sourced from an online platform (i.e., Prolific). Psychometric properties were examined using the Rasch Measurement Theory analysis. A test–retest reproducibility study was performed, and construct validity was examined.
Results:
Content validity was established after 10 cognitive interviews. A total of 233 people with lower extremity wounds (age 19–80 years, mean 39.3) participated in the field test. All 25 items tested demonstrated good fit to the Rasch model with ordered thresholds. One item had a fit residual outside ±2.5, but no items had significant χ 2 values after Bonferroni adjustment. Reliability was high with the person separation index, Cronbach alpha, and intraclass correlation coefficient values >0.8. Strong correlations were found between the Function and Symptoms scales and EQ-5D dimensions measuring similar constructs as well as the EQ-5D global score. All hypotheses for construct validity were confirmed.
Innovation:
Patient-reported outcome measures are an important component of patient-centered care, as they capture the patient’s perspective in a rigorous and reproducible way. Adding these two scales to the WOUND-Q provides a means to measure function and symptoms associated with lower extremity wounds.
Conclusion:
These new WOUND-Q scales can be used to measure outcomes important to patients with lower extremity wounds in clinical settings and research studies.
INTRODUCTION
Chronic wounds are a growing public health challenge. 1,2 With a prevalence of 2.21 per 1,000 people, 3 chronic wounds impact millions of people worldwide. The most common type of chronic wounds are lower extremity wounds, 3 which tend to be caused by arterial insufficiency, venous insufficiency, mixed arterial and venous insufficiency, pressure injuries, and/or diabetes. 4 The risk of developing a lower extremity wound increases in older people, those with obesity, and those with diabetes. 1,5 –7 The increasing incidence of chronic lower extremity wounds, linked to an aging population and rising obesity rates, places a considerable burden on the health care systems. 1,2,8,9
In addition to the high burden that lower extremity wounds have on health systems, they also have a multifaceted and often negative impact on patients. 8,10 –14 Wound-related concerns such as pain, 8,10,15,16 foul odor, 10,14 impaired mobility, sleep disturbances, social isolation, and financial and psychological distress 8,10,11,14 –17 contribute to worse health-related quality of life (HRQL). Given the significant impact lower extremity wounds can have on HRQL, it is imperative to understand how HRQL is affected to improve it. 18 Patient-reported outcome measures (PROMs) are designed to measure patients’ self-reported experiences, symptoms, functioning, and quality of life in a quantitative manner. These outcomes, also known as patient-reported outcomes (PRO), are defined by the Food and Drug Administration as “any report coming directly from patients about health condition and its treatment.” 19 The implementation of PROMs in clinical practice has been found to enhance the quality of health care through improvements in diagnosis, patients’ perceptions of communication, disease control, and patient’s quality of life. 20 PROMs can be divided into two main categories, that is, generic and condition-specific. Generic PROMs can be used across a wide range of health conditions; in contrast, condition-specific PROMs are developed to assess outcomes for a specific condition. When PROMs are designed by eliciting concepts important to patients, it ensures that only patient-centered outcomes relevant to patients are measured. A condition-specific PROM further ensures that important and relevant outcomes to the specific patient population are measured. The choice between these two types of PROMs depends on the objective of the assessments. 19,21
INNOVATION
Lower extremity wounds are common and associated with a significant symptom burden and impact on function and mobility. We have added two new scales to the condition-specific PROM WOUND-Q (i.e., Function, Symptoms) for patients with lower extremity wounds (Fig. 1). Adding these scales to the WOUND-Q fills an important gap in the measurement of outcomes for lower extremity wounds. Using the WOUND-Q with these two new scales in research and clinical settings has the potential to improve patient care.
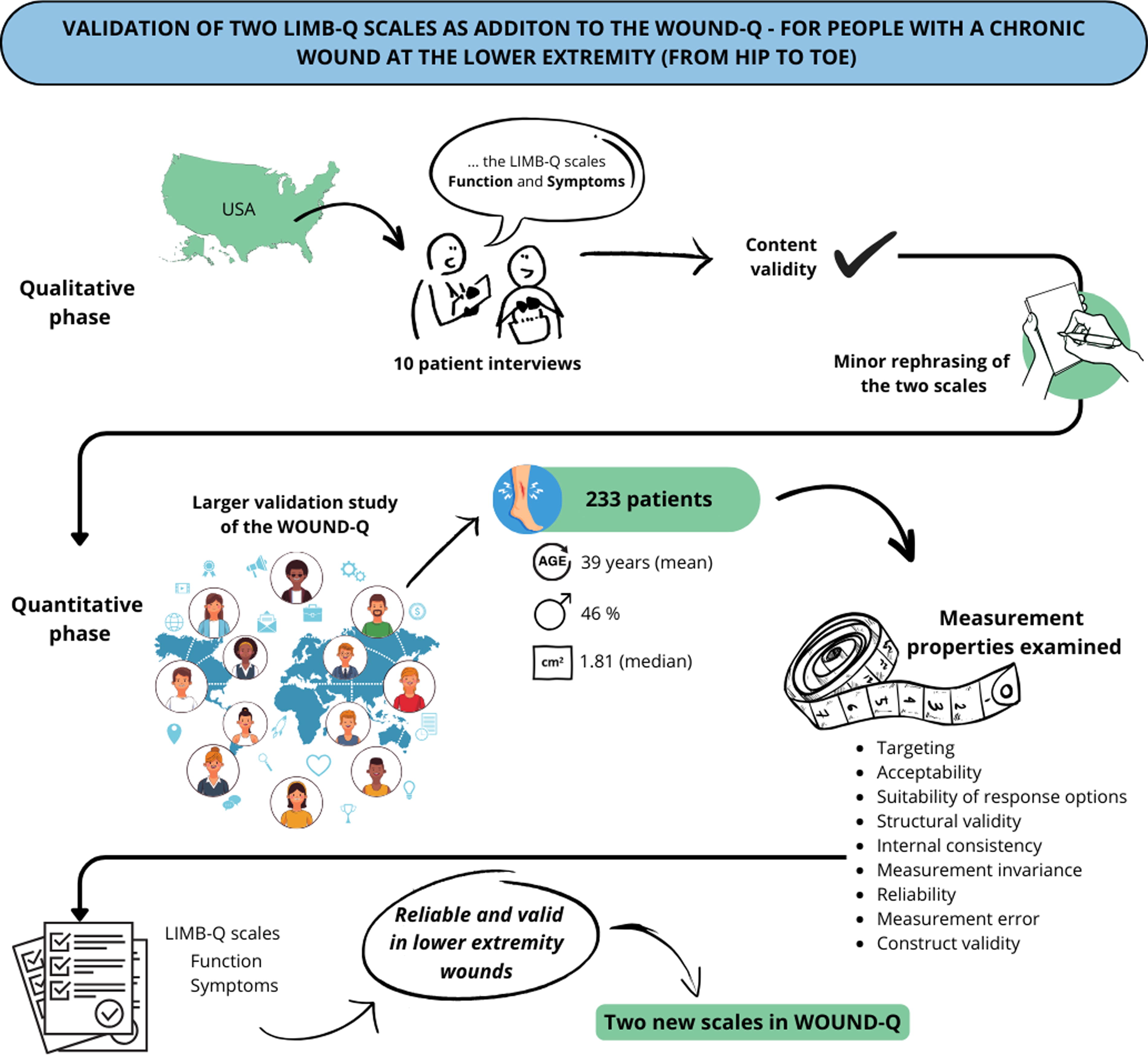
Summary graphic.
CLINICAL PROBLEM ADDRESSED
The WOUND-Q is a condition-specific PROM developed and validated to measure PROs important to people with chronic wounds. It has recently been identified as the highest quality PROM for chronic wounds. 22 The development and validation of the WOUND-Q have been described previously. 23 –27 Given its modular design, WOUND-Q offers the flexibility to expand by adding new scales that enhance its coverage. The original version of WOUND-Q did not include scales for assessing function and symptoms related to lower extremity wounds. These are important concepts for patients receiving wound treatment, which could be integrated to enrich the PROM’s comprehensiveness. 16
Our group previously developed and validated the LIMB-Q, a PROM for lower extremity trauma patients. 28 –32 We followed the same international, rigorous PROM development guidelines as we did for the WOUND-Q to develop the LIMB-Q. 19,23,28,33 –36 Although the LIMB-Q was developed for lower extremity trauma, patients with limb-threatening soft tissue wounds, independent of the etiology, often undergo very similar treatment pathways. For this reason, our group hypothesized that the LIMB-Q Function and Symptoms scales would be relevant to patients with lower extremity wounds. Therefore, the primary aim of this study was to evaluate the content validity and psychometric performance of the LIMB-Q Function and Symptoms scales in patients with lower extremity wounds.
MATERIALS AND METHODS
This study was performed in two parts: an initial qualitative phase followed by a quantitative phase. Ethics approval for the qualitative phase was obtained at Georgetown University (IRB STUDY 00001591) and for the quantitative phase, from McMaster University (Hamilton Integrated Research Ethics Board [#14946]). A license agreement was obtained to use the EQ-5D-5L. 37
The Function and Symptoms scales
The development of the LIMB-Q has been published previously 28 –32 and followed international guidelines for PROM development. 19,33 –36 Briefly, the LIMB-Q contains 16 independently functioning scales. These scales were developed from 33 qualitative patient interviews, further refined through 12 cognitive debriefing interviews and insights from 43 experts and field-tested in an international sample of 713 patients. The field-test versions of the Function and Symptoms scales had 37 and 17 items, respectively, which were reduced to 15 and 10 items following the psychometric analysis using the Rasch Measurement Theory (RMT). 32 In the qualitative part of this study, we examined content validity for all 54 items. For the RMT analysis, we performed the psychometric analysis for the final set of 25 items.
Content validity: Qualitative phase
Content validity was established through a series of cognitive debriefing interviews. The sample included patients with chronic lower extremity wounds recruited from a multidisciplinary outpatient wound clinic at Georgetown University. This institution has a unique chronic wound and limb-salvage clinic. It is overseen by plastic surgeons but is run by a multidisciplinary team that includes vascular surgery, wound care, physical medicine and rehabilitation, and prosthetists. This clinic manages the chronic and diabetic wounds for the health system. To maximize variability in clinical and demographic variables, purposeful sampling was used. Recruitment took place between June and September 2020. As only the field-test version was available at the start of the study, this version was included in the qualitative and quantitative phases of this study. To adapt the LIMB-Q scales for the chronic lower extremity wound population, minor adjustments were made in the instructions, such as replacing “injured lower limb” with “lower limb.” These modifications are shown in Supplementary Appendix A. Interviews were conducted using an interview guide and performed by one interviewer (TS). Participants were shown the two LIMB-Q scales, Function and Symptoms, during their interview. Feedback was solicited on the comprehensibility and relevance of the instructions, items, and response options, and participants were encouraged to suggest any missing content. All interviews were audio-recorded, transcribed, and coded line-by-line. Coding was conducted in Microsoft Word (Version 2307; Redmond, WA) by N.V.S. and transferred to a Microsoft Excel (Version 2307; Redmond, WA) worksheet for analysis using DocTools.
Field testing: Quantitative phase.
Sample and recruitment
The LIMB-Q Function and Symptoms scales were administered to an international sample of patients with chronic lower extremity wounds identified in Prolific Academic (“Prolific” www.prolific.com), an online patient research platform. Data were collected using a REDCap (Research Electronic Data Capture) survey and collected as part of a larger study examining the psychometric performance of 9 WOUND-Q scales across various chronic wound types in an international community-based sample. 25 In Prolific, an initial screen was administered in August 2022 to identify people aged 18 years and older who were fluent in English and had one or more chronic wounds located anywhere on their body. A chronic wound was defined as a wound that had lasted at least 3 months. Eligible patients were then invited to complete the survey in September 2022. Participants who reported a wound on their leg, ankle, foot, or toe using branching logic were invited to answer the LIMB-Q Function and Symptoms scale. The survey did not specify the anatomical definition of the leg. Based on common knowledge, the leg should be understood as the region from the hip to the ankle. In addition to completing the scales, participants answered questions about wound characteristics, treatments, and demographic information. They also completed the EQ-5D-5L, 37 a generic HRQL PROM that has been validated in venous leg ulcers. 38 –40 The EQ-5D-5L consists of two sections. One part describes health states by five dimensions, rated from level 1 (no problem) to 5 (unable/extreme problems). The second part is the EQ-VAS, where participants rate their overall health state from 0 (worst) to 100 (best). EQ-5D assessments were used to examine convergent validity. At the end of the survey, participants were invited to participate in a test–retest reproducibility (TRT) study seven days after the initial assessment. We aimed to include about 100 assessments in REDCap for the test–retest survey. Since the number of assessments for the TRT survey was limited, participation was on a first-come-first-serve basis. In the main survey and TRT, participants were able to skip answering any of the scale items. All participants were paid a minimum of 10 GBP per hour.
Scoring of PROMs
Scores for the Function and Symptoms scales were computed by adding the raw scores of the scales to get a total raw score. For cases with missing data with less than 50% of the scale’s items, the within-person mean for completed items was imputed before computing the total raw score. The total raw scores were converted to the continuous score (0–100) using the LIMB-Q scoring key. 32 EQ-5D index scores for each dimension and the overall global score were computed using the UK normative values. 41
STATISTICAL ANALYSIS
Psychometric analyses were performed on the final versions of the two LIMB-Q scales to assess the applicability of these scales across clinical conditions. Psychometric analysis used RMT analysis and followed COSMIN (COnsensus-based Standards for the selection of health Measurement INstruments) standards for psychometric performance.
42
RMT analysis examines how responses to items on a scale align with what is expected by the measurement model.
43
In the Rasch model, scales should be unidimensional, and items should map out a clinical hierarchy. When data fit the Rasch model, the scale has interval-level measurement properties, making it suitable for parametric statistics.
43
The RMT analysis was conducted with RUMM2030 software (RUMM version 2030, RUMM Laboratory Pty Ltd, Duncraig, Western Australia, Australia, 1998–2023),
44
using the unrestricted Rasch model for polytomous data.
45
Descriptive statistics, test-retest analysis, and construct validity analyses were performed using SPSS (Version 28; IBM Corporation, Armonk, NY, USA). The following psychometric tests were carried out: Fit statistics: Three-item fit statistics—(1) item characteristic curves (IC), (2) item fit residuals (item–person interaction), and (3) χ
2 values (item–trait interaction)—were performed to examine if the scale items measure the same underlying construct. IC were visually inspected. Fit residuals are considered ideal within ±2.5. Nonsignificant Bonferroni-adjusted χ
2 values indicate that the items fit the Rasch model. Category threshold order: Threshold maps were examined to ensure that the response options functioned as intended, for example, lower values on the scale representing lower positions on the continuum. Targeting: Person–item threshold distribution (item-map) and the proportion of participants scoring outside the scale were assessed graphically and statistically, to evaluate if the items within each scale effectively measured the construct experienced by the sample. Persons and item locations should be mirrored on the item-map for a scale to be targeted. The proportion of participants with extreme scores (ceiling or floor effects) and those skipping items (missing data) were calculated for each scale. A floor/ceiling effect was considered significant if ≥15%,
46
whereas the item-level missing data should be <10%.
47
Stability: Differential item functioning (DIF) was examined to determine if the items were responded to differently by different subgroups in the sample. We examined DIF by age group (<35 vs. ≥35 years), gender (man vs. woman), and sample (current sample vs. LIMB-Q sample). Random samples were selected to ensure a balanced size in each group. We performed DIF for scales with at least 75 participants in each subgroup. The analysis was conducted three times for each scale to determine if any DIF detected was stable. Items with significant Bonferroni-adjusted χ
2 values were split by the relevant patient characteristics. To judge if the items with DIF impacted the scale scoring, we computed Pearson correlations for original and adjusted person locations. DIF by sample was examined to evaluate if the LIMB-Q scoring keys were valid in the study sample. Dependency: Correlations between items in each scale were conducted to examine if a person’s response to one item influenced the response to another item. Item pairs with correlations >0.2 were included in subtest analysis to assess their impact on scale reliability. Reliability and reproducibility: Internal consistency was evaluated by Cronbach alpha.
48
Person Separation Index (PSI) was used to examine the scales’ ability to differentiate between people in the sample. TRT was evaluated by one-sample t-test to determine if the mean difference in the scale scores between the first (T1) and the second (T2) assessment was different from zero and by intraclass correlation coefficients (ICCs) using the two-way mixed-effect model, based on average measurements as we deal with group statistics, evaluating for absolute agreement between scale scores.
49,50
The mixed-effect model was chosen, as the time point was fixed. Absolute agreement was chosen, as agreement between scale scores at T1 and T2 and systematic differences in the participant’s scores were of interest. Systematic bias is not included when evaluating for consistency. Only participants who indicated that they did not experience an important change in the construct measured by the scale between the T1 and T2 were included in the TRT analysis. Reliability coefficients ≥0.70 were considered acceptable.
42,46
Measurement error: The standard error of measurement (SEM) was conducted based on participants stating no important change between T1 and T2, using the formula SEMconsistency = ((T1(SD) + T2(SD))/2) × √(1-ICCagreement). The SEM was converted into the smallest detectable change (SDC). The SDC was computed on a group level with the formula SDCgroup = (1.96 × √2 × SEM)/√n. 46,51,52 The SDCgroup indicates the minimum score change needed to ensure it is true and not a product of measurement error between groups. The SDC is based on the SEM, which is the error around each person’s scale score. Regardless of the person’s location on the scale’s continuum (0–100), the SEM is assumed to be constant. However, scores at the floor and ceiling are less precise than scores at the center. Furthermore, the distribution of scale scores (standard deviation), which is dependent on the study population, affects the SEM. As a result of these limitations, the SDC is not recommended for decision-making at the individual patient level. 51
Construct validity: To examine convergent validity, correlations were computed between the scores of the Function, Symptoms, EQ-5D dimensions, EQ-5D global, and the EQ-VAS. COSMIN criteria state that correlations should be ≥0.50 for scales measuring similar constructs, 0.3–0.5 for scales with related but dissimilar constructs, and <0.3 for scales with unrelated constructs. 42 Hypotheses for convergent validity are available in Supplementary Appendix B. Furthermore, we hypothesized that the number of wounds would correlate <0.3 with the LIMB-Q Function and Symptom scores. Lastly, we hypothesized that participants with lower levels of mobility, measured by the EQ-5D Mobility dimension, would have lower scores on the Function scale. The last hypothesis of discriminative ability was examined by one-way analysis of variance (ANOVA) and post hoc analysis. Participants were classified into four mobility groups: no problems walking about, slight problems, moderate problems, and severe problems. Homogeneity of variance between the groups was tested by Levene’s test. For construct validity analysis, parametric and nonparametric tests were used depending on data normality. Continuous data were inspected for normal distribution by QQ plots and statistically by skewness and kurtosis. Kurtosis and skewness should be within ±2 for data to be considered normally distributed. 53
RESULTS
Qualitative phase
We performed 10 cognitive interviews with 5 men and 5 women. The mean age of the sample was 59.7 years (range 37 to 71 years). The sample included one person who had an active wound, two with a wound that had healed, and seven who had an amputation for a lower extremity wound. Most of the latter group had amputations because of a diabetic foot wound (n = 6). Participant demographics and quotes about relevance, comprehensibility, and comprehensiveness are in Supplementary Appendix C. Most participants found the content of the two scales relevant and easy to understand. A participant who did not have symptoms reported that the Symptoms scale was not relevant. The remaining participants found the two scales comprehensive and relevant to their lower extremity wound or subsequent amputation.
Quantitative phase
Study participants
Of the 421 participants recruited for the WOUND-Q study, 233 participants had a chronic lower extremity wound and completed one or both of the two new scales. 25 The sample consisted of 108 (46%) men, 122 (52%) women, and 3 (1%) people who identified as another gender. The mean age was 39.3 years (standard deviation [SD] 14.2 years, range 19–80 years). A total of 125 (54%) participants were ≥35 years old. Most people identified as Whites (n = 156, 67%), followed by Blacks (n = 49, 21%). In the sample, 66 (28.3%) participants currently smoked or vaped. A third (n = 73, 31%) reported no comorbidities, 86 (37%) reported 1, and 74 (32%) reported >1. Dependency of a supportive device (e.g., crutches, prosthesis, wheelchair) to move around was reported by 41 (18%) participants. Most participants had one chronic wound (68%). The median self-reported wound size (width × length) was 1.8 cm2. The leading cause for the wounds was trauma (35%), and for most participants (n = 123, 53%), the duration of the wound was between 3 and 6 months. Table 1 presents further demographic, clinical, and wound characteristics.
Demographic and clinical characteristics of the 233 participants
*Able to choose multiple.
**From hip to toes.
***From hip to ankle.
SD, standard deviation.
Psychometric findings
Psychometric data derived from the RMT analysis are presented in Table 2, Table 3, and Supplementary Appendix D and are described next.
Function and Symptoms scales and scores
Percent of respondents with 0 in score.
Percent of respondents with 100 in score.
Percent of respondents with at least one missing item (item-level).
No., Number.
RMT scale-level statistics
Total items and number of item pairs with residuals >0.2.
α, Cronbach alpha; DF, degrees of freedom; extr, extremes; No., number; PSI, Person Separation Index; RMT, Rasch Measurement Theory.
Test–retest statistics and measurement error statistics
Owing to change in scale construct.
Testing if mean change between T1 and T2 is different from zero, two-tailed p value.
Average measure as we deal with group statistic.
CI, confidence interval; ICC, intraclass correlation coefficient; SDC, smallest detectable change; SEM, standard error of measurement; T1, first assessment; T2, second assessment, seven days later.
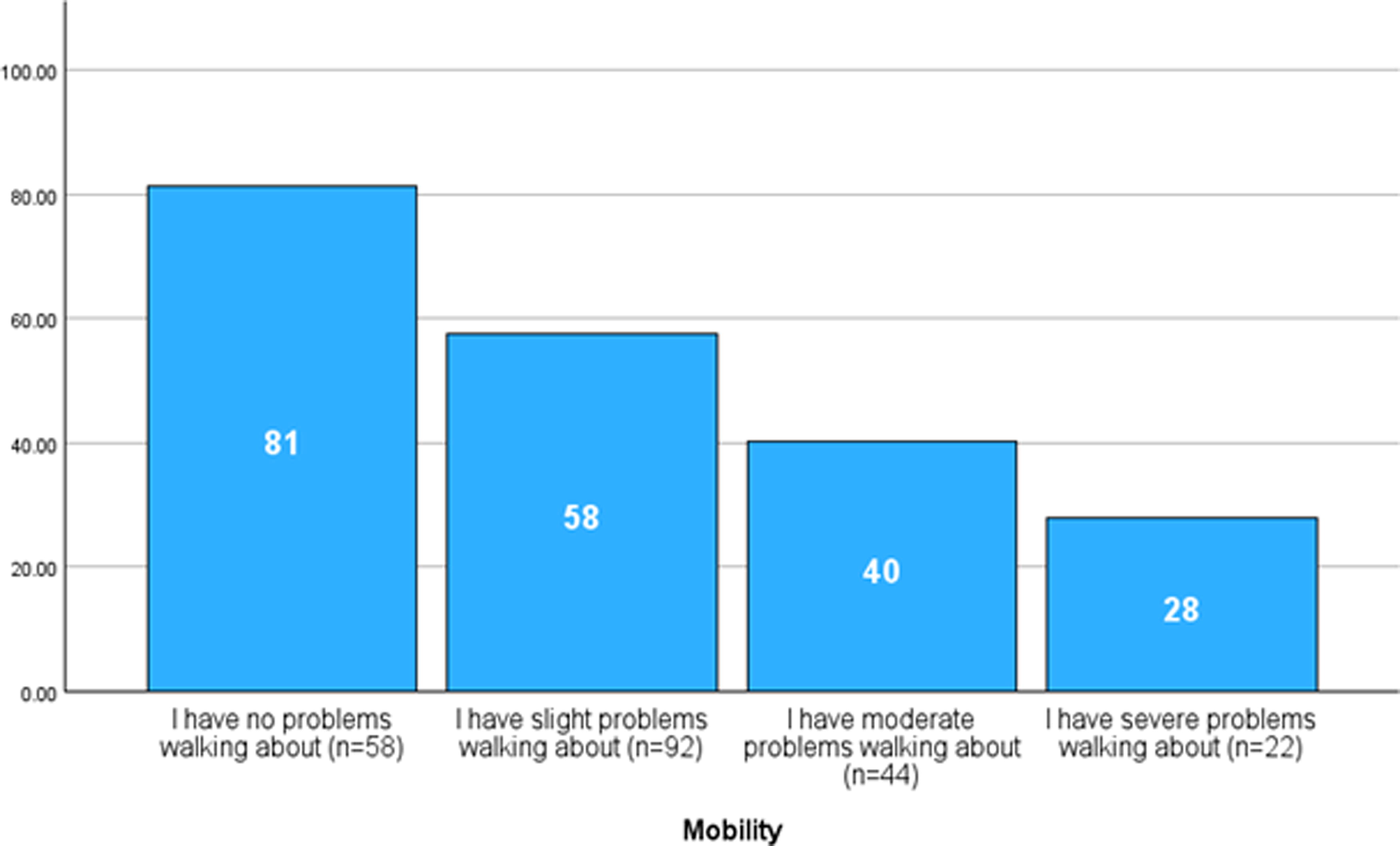
Mean score of the Function scale by four mobility groups. All mean scores differed significantly (p < 0.05) between the four groups based on Welch’s ANOVA and Games–Howell post hoc analysis. ANOVA, analysis of variance.
DISCUSSION
This mixed-methods study examined the psychometric properties of the two LIMB-Q scales, Function and Symptoms, in 233 patients with chronic lower extremity wounds. The 10 cognitive interviews with patients with a history of a chronic wound provided evidence that the scales measured relevant concepts and that nothing important was missing from them. Our field-test study provides evidence that the Function and Symptoms scales were psychometrically valid and reliable outcome measures in patients with all types of chronic lower extremity wounds.
The importance of PROMs for benchmarking, patient-centered care, research, and outcome monitoring in chronic wounds is well grounded. 21,54,55 Numerous different condition-specific PROMs have been developed for wound patients, with most focused on specific types of wounds. 22,24 Systematic reviews have identified a need for well-developed and valid PROMs for patients with diabetic foot or venous leg ulcers. 56,57 The WOUND-Q is a promising PROM designed for all types of chronic wounds. In a review of 33 wound-specific PROMs, the WOUND-Q was recommended for use in research and clinical care. 22 Currently, this PROM is used in the statewide program “Leading Better Value Care” in New South Wales, Australia. 58
When incorporating new scales into a PROM, their psychometric performance must be examined in the target population to assess whether valid conclusions can be drawn from these measures. Both scales we tested fulfilled the demands of the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) criteria on measurement properties. 42 The RMT analysis revealed that each scale’s items successfully mapped out a clinical hierarchy covering the experiences and abilities of the population (target to sample). The LIMB-Q scoring key was found valid for use in chronic lower extremity wound patients as the items with DIF did not impact the scoring of the two scales. Having the same scoring key makes it possible to directly compare patients with lower extremity wounds with patients undergoing reconstruction or amputations due to trauma. Regarding reliability, the Function scale had some items that evidenced local dependency, although this did not have an important impact on scale reliability. Based on ICC estimates, the scales were found applicable for decision-making at group level, as ICC estimates and 95% confidence interval (CI) were >0.7. 59,60 The SDC is a valuable tool to help interpret if there is a change in score outside of measurement error, but opposite to the minimal important difference (MID), it does not report if the patients find the change important. 52,61 However, anchor-based MIDs do not consider measurement error, and to conclude that a change in score is clinically important and not a result of measurement error, the SDC should ideally be smaller than the MID. 61 –63
This study has some methodological considerations. The cognitive interviews were performed at a single site in the United States, which can limit its generalizability. Also, the participants consisted mainly of people with prior wounds that had either healed or been managed with an amputation. It is possible there could have been recall bias when judging the relevance and comprehensiveness of the scales. We feel this is unlikely as participants had rich experiences with lower extremity wounds, and those with amputations would have gone through a lengthy attempt at limb salvage. Given the sample, our findings suggest that the scales apply to patients before and after amputation. Further research examining the finalized scales’ content validity in a sample of patients with lower extremity wounds could confirm these findings. Having scales that are relevant to patients before and after amputation is essential, as amputations among patients with diabetes are preceded by a wound in more than 80% of cases. 64,65 It has been found that amputations can improve mobility, reduce symptoms in the lower extremities, and enhance HRQL compared with living with an ulcer. However, the evidence is contradictory, and there is a need for more knowledge about the patient’s perspective to guide decisions regarding nonemergency lower extremity amputations. 66 The Function and Symptoms scales could provide important insights throughout this trajectory. The quantitative part of the study tested the scales in an international online sample. In using the online research platform Prolific, individuals self-select to participate, and all data were patient-reported, which we could not verify. Data from crowdsourcing platforms have been found reliable and valid, 67 –70 but participants were paid for their time, which might have motivated some to participate. 71,72 Our chronic wound sample was relatively young, resulting in a higher proportion of people with traumatic wounds. However, a 50% increase in the proportion of younger persons <65 years with a wound was found in the United Kingdom between 2012 and 2018, stating that wounds are not only a condition in older people. 2 Lastly, the Function scale is only applicable to patients who can walk. Owing to the small sample size, DIF could not be examined for subgroups based on the type of assistive device used (e.g., boots, crutches, walker), neuropathy, or by treatment approach (e.g., amputation, reconstruction), factors that can impact balance and walking ability. However, no DIF was found in a sample of patients with lower extremity traumas who were treated with either fracture surgery or reconstruction/amputation, providing evidence that the Function scale works the same across these treatment types. 32
As wound closure can take months to years or may never be achieved, it is critical to provide wound management that can improve outcomes that are important to patients. By validating and adding the Function and Symptoms scales to the WOUND-Q, it is possible to measure how chronic lower extremity wounds and their treatment affect patients from their perspective. Implementing these scales in clinical care may improve patient–provider communication, shared decision-making, and better treatment outcomes. 20,21,55 In conclusion, we have demonstrated the psychometric properties of the Function and Symptoms scales in adults with chronic lower extremity wounds. The scales were well-targeted, reliable, and valid, making them suitable for integration into the WOUND-Q. The WOUND-Q now comprises 15 independently functioning scales with these additions. The WOUND-Q can be accessed at qportfolio.org/woundq/
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors want to acknowledge the patients’ interest and participation in this study. Furthermore, they would like to thank Tanvee Singh and Paige Dekker, who recruited and conducted the cognitive interviews. A.F.K. received funds from the Department of Pediatrics, McMaster University, for data collection. Grants were given from Odense University Hospital (grant number A4774) and the Region of Southern Denmark (grant number 21/58368) to N.V.S.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the article as follows: study conception and design: N.V.S. and A.F.K.; data collection: N.V.S., A.F.K., C.R., L.R.M., and K.L.F.; analysis and interpretation of results: N.V.S., A.F.K., and C.R.; draft article preparation: N.V.S., L.R.M., A.F.K., C.R., and L.R.P. All authors reviewed the results and approved the final version of the article.
AUTHOR DISCLOSURE AND GHOSTWRITING
L.R.M. is a codeveloper of the LIMB-Q, and A.F.K. and A.L.P. are codevelopers of the WOUND-Q and LIMB-Q and would receive a share of any license revenue in for-profit studies. A.F.K. provides research consulting services to pharmaceutical companies through EVENTUM Research. The rest of the authors have nothing to disclose.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Appendix A
Supplementary Appendix B
Supplementary Appendix C
Supplementary Appendix D
Supplementary Appendix E
ABBREVIATIONS AND ACRONYMS
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.