
Abstract
Significance
: Burns result in irretrievable cell damage, which can occur upon exposure to hot surfaces, liquids, gases, ultraviolet or ionizing radiation, and through friction. Standard of care in burn management involves protecting the patient, limiting burn progression, and achieving wound closure. Negative pressure wound therapy (NPWT) and NPWT with instillation and dwell time (NPWTi-d) are two wound management options that have been shown to improve outcomes for burn patients in recent years. This work provides a general review of NPWT and NPWTi-d use in burn wound management. A literature search was performed using PubMed and Embase for peer-reviewed publications and conference abstracts written in English and reporting on burn management using NPWT and/or NPWTi-d from a single manufacturer between 2000 and 2021. All burn types were included.
Recent Advances:
Thirteen studies and 308 patients were available for assessment. Use of NPWT was reported in a majority of studies (n = 11). When conventional NPWT was applied, graft take of >90% was observed and consistent final wound closure was achieved. Two studies described NPWTi-d use for burn wound management. NPWTi-d use promoted granulation tissue development in burn wounds.
Critical Issues:
Limited high-level prospective evidence exists for use of NPWT and NPWTi-d in burn wound management.
Future Directions:
Available literature on the use of NPWT and/or NPWTi-d in burn care has reported improved outcomes in wound bed preparation, which can ultimately lead to final wound closure. The use of these modalities should be considered in management of burn care patients.

SCOPE AND SIGNIFICANCE
Burn injuries remain a critical issue globally, hence the need to improve our approach in this area, which requires focused resources and clinically reproducible protocols. Current wound care regimens employed to manage burn patients are governed by the need to protect the wound, control the wound area, and limit injury progression and complications. The overarching goal of selecting advanced wound care technologies is that they provide adjunctive support in the overall continuum of care and improve clinical outcomes.
TRANSLATIONAL RELEVANCE
Negative pressure wound therapy (NPWT) and the modality with fluid instillation (NPWTi-d) are particularly important in burn care. Mechanistically, the modalities deliver therapy through a closed system and facilitate better regulation of wound conditions while preparing the burn defect to achieve faster definitive closure. A dilution effect observed during the instillation phase of NPWTi-d helps with wound contaminant and infectious material removal without compromising the closed system therapy, which is advantageous for effective burn injury management.
CLINICAL RELEVANCE
This review may be used as a reference when considering revisions to current clinical protocols for burn injury care with adjunctive NPWT or NPWTi-d. Outcomes reported here demonstrate that NPWT technologies can be used in a step-up (transition to wound care requiring an increased level of support, i.e., use of NPWT until surgery can be undertaken) or step-down (transition to wound care that requires a lower level of support, i.e., from NPWT to standard wound dressings) approach to successfully manage a burn injury pre- and postdefinitive closure, while offering certain advantages over conventional dressings.
BACKGROUND
Burns are categorized as thermal, radiation, chemical, electrical, or friction. Burns are then classified as first, second, third, or fourth degree (Fig. 1). When inflammatory mediators are released, edema formation is caused by capillary leakage, resulting in soft tissue loss. Secondary to tissue damage, the injury prevents maintenance of homeostasis, and cell apoptosis releases toxins into the blood stream, directly damaging organs that can also lead to systemic shock. 1 Assessment of a burn involves calculation of the total body surface area (TBSA) and severity based on the anatomic thickness of the defect.
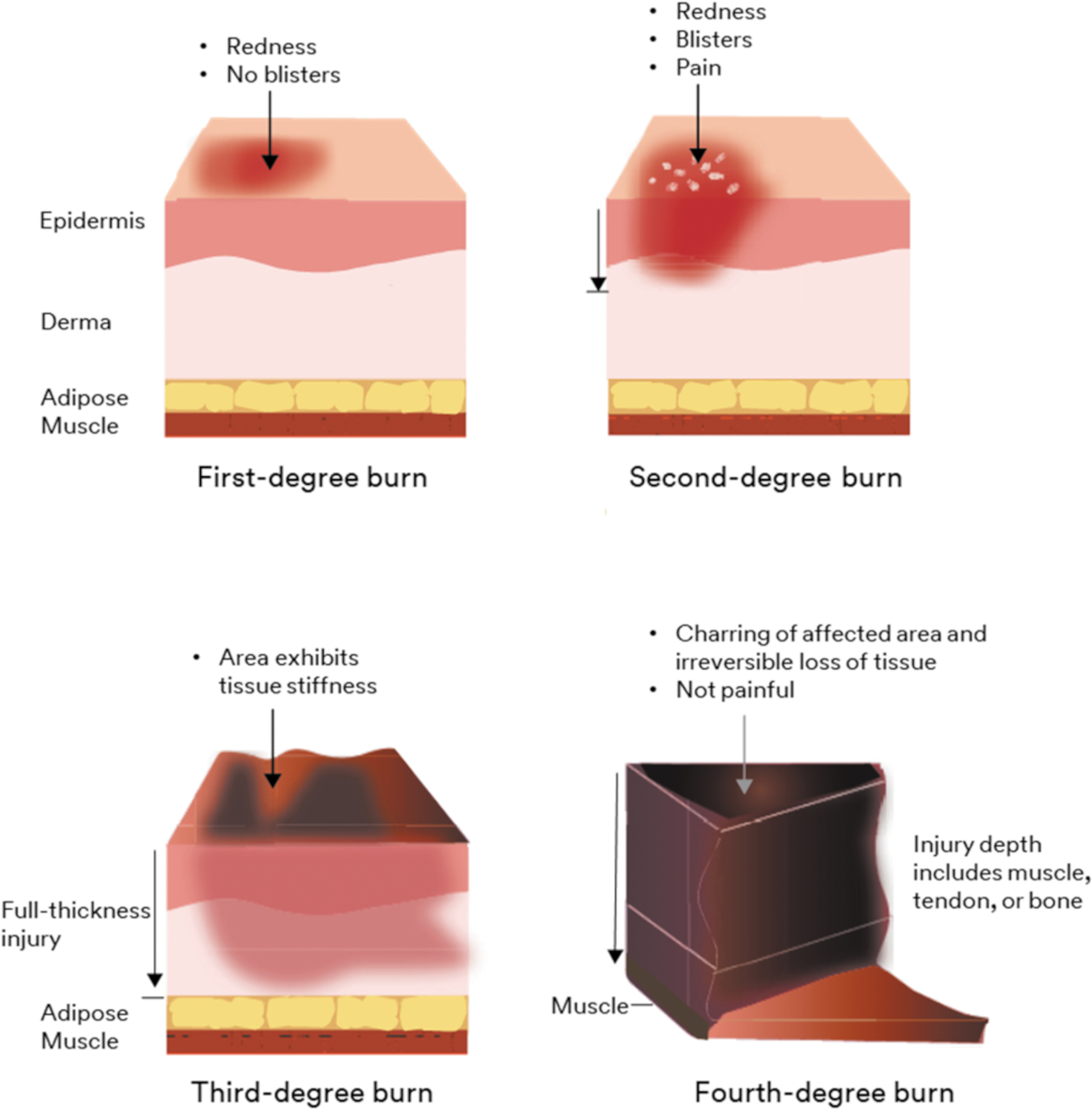
Burn injury classification.
Upon presentation, general clinical therapy options are as follows: cool the wound to minimize burn progression while maintaining stable core body temperature, surgically debride the necrotic tissue, and stabilize the patient's condition. Next steps include preparing the wound for definitive closure, treating the infection prophylactically, and managing pain. Once the patient is stable, the clinician should proceed with soft tissue reconstruction and prevent blood clot formation in patients with severe burns (Fig. 2). Burn injuries require prompt intervention to achieve definitive closure of the exposed defect to limit wound progression and circumvent complications.
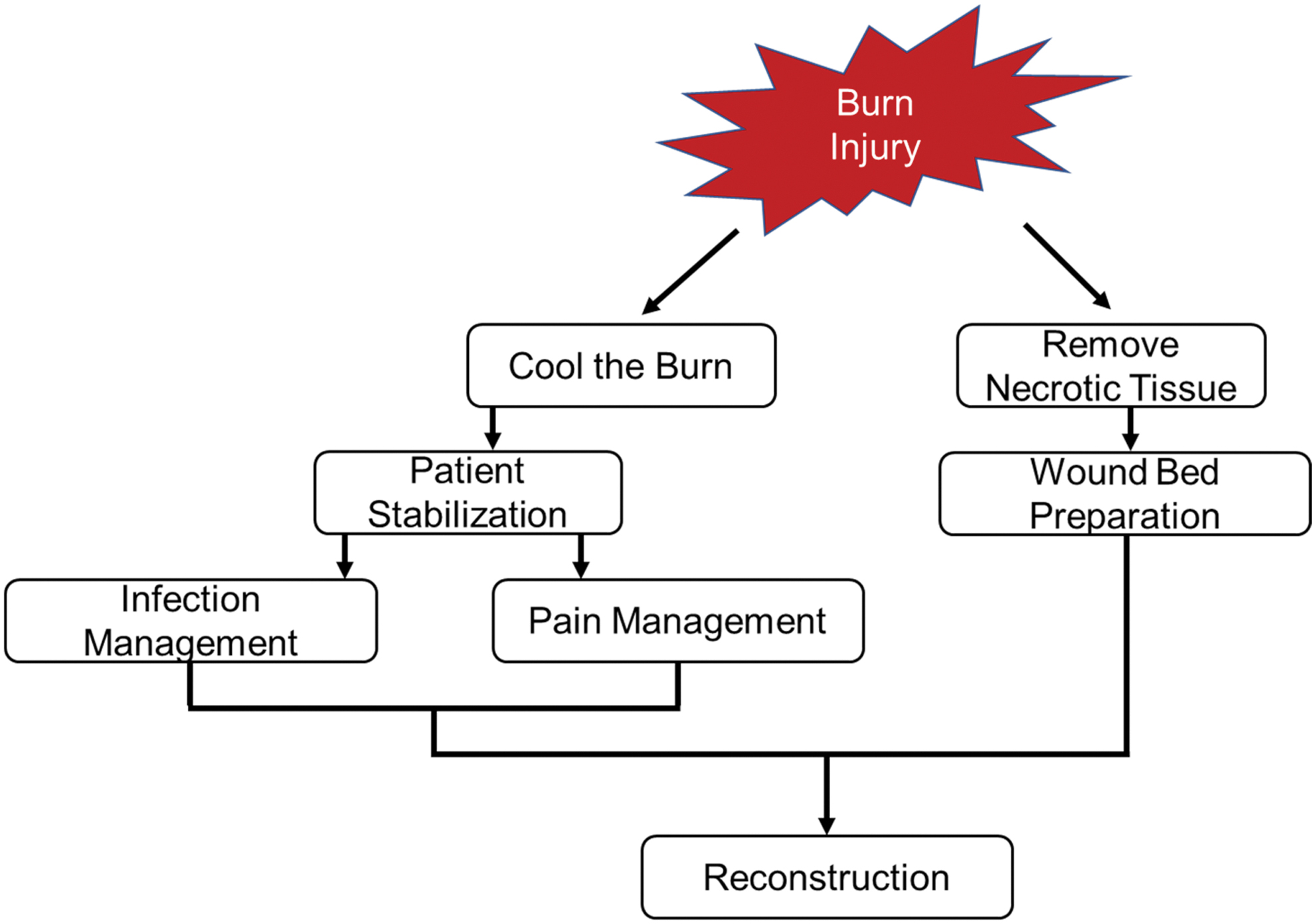
Stages of burn injury management.
Globally, the prevalence of burn injuries has been decreasing, particularly in high-income countries; however, rates remain high in low/middle-socioeconomic geographies. 2 –4 Exposed soft tissue and the immunocompromised state of the patient are contributing factors to the raised risk of infection. 5 Avoiding infection and preventing sepsis are the two major medical challenges that clinicians face during burn management, aside from closing the defect. Infection and sepsis are linked to 33–80% of deaths in burn patients. 6 Early intervention postinjury and preparation of the wound bed for prompt primary closure (flap/graft) are key clinical goals attributed to successful burn closure rates and healing. 7 –9
The quality of burn care is correlated with a multidisciplinary team approach and multifaceted treatment plan. 10 Medical technology is one adjunctive element that plays a supporting role in the continuum of care. Conventional burn injury management techniques are limited by wound TBSA percentage, dressing capacity to control high exudate volumes, dressing size, and the dressing's occlusive properties. 11 –13 Availability of healthy donor sites, delayed wound closure, and challenges with wound fluid control raise the risk of wound contamination and infection. As such, alternative burn wound management techniques need to be explored.
Active wound care therapies have significantly improved the standard of care for burn patients in recent years, although access to active wound care such as NPWT and NPWTi-d is limited in low- and middle-income countries. 14 NPWT (3M™ V.A.C.® Therapy; 3M Health Care, St. Paul, MN) and the enhanced modality with fluid instillation, NPWTi-d (3M™ Veraflo™ Therapy; 3M Health Care), are two recognized technologies that have been successfully used to manage complex wounds. Mechanistically, NPWT and NPWTi-d both promote wound healing conditions by creating a closed regulated environment for wound management (Table 1).
Negative pressure therapy mechanisms of action
NPWT, negative pressure wound therapy; NPWTi-d, negative pressure wound therapy with instillation and dwell time.
For NPWT, wound bed preparation and healing are driven by a customizable, semirigid, reticulated, open-cell foam–wound interface that initiates a microdeformation effect under subatmospheric conditions. 15 Exudate management, edema reduction and/or control, temporization, wound bed preparation, and bolstering grafts for definitive closure are key clinical objectives of NPWT in burn wound management. The NPWT mechanisms of action enable continuous removal of wound fluid while protecting the defect from external contaminants, limiting burn progression, and decompressing the injury site.
NPWTi-d combines the features of NPWT with wound cleansing. A topical wound solution is instilled into the wound bed; allowed to remain in place to dilute and solubilize debris, exudate, and infectious materials; and then removed during the subsequent negative pressure cycle. The wound cleansing effect generated by NPWTi-d favorably improves the wound condition and helps reduce time to primary closure of the soft tissue defect compared with standard-of-care techniques. 15,16
This literature review was conducted to assess the use of NPWT and NPWTi-d in management of burn injuries. The advanced negative pressure technologies described in this report demonstrate a solid foundation, which may be utilized to prepare the wound bed for closure and, in the case of NPWT, help bolster skin grafts to reestablish the natural skin barrier more rapidly.
RATIONALE
A 2014 Cochrane review aimed to investigate and summarize the outcomes of studies describing NPWT management of partial-thickness burns. The inclusion criterion was restricted to randomized control trials (RCTs). Only one interim RCT report met the search criterion and limited author's capacity to present outcomes and conclusions at the time of publishing. 17 High-level studies are still lacking in the area of NPWT and NPWTi-d management of burn injuries. This work presents a general review of the use of one NPWT system and one NPWTi-d system in burn wound management.
METHODS
A literature search was performed in PubMed and Embase using the following search terms: negative pressure wound therapy, vacuum-assisted closure, negative pressure therapy, subatmospheric therapy, burn, thermal injury, or frostbite. Peer-reviewed publications and conference abstracts, written in English, and reporting on burn management using NPWT and/or NPWTi-d from a single manufacturer (3M Health Care) between 2000 and 2021 were included. Only a single manufacturer was identified to reduce variability in the analysis. All burn types were included.
RESULTS
A total of 32 publications were identified during the literature search. A full-text review identified 21 articles, following removal of duplicates. Eight articles were excluded for descriptions of alternative NPWT technologies (n = 5), for not mentioning the NPWT system use (n = 1), and for methods not indicated for use (n = 2). Thirteen articles with 308 patients were included in the review (Fig. 3, Tables 2 and 3). 12,13,18 –28 Article types included a randomized controlled trial (RCT, n = 1), retrospective studies (n = 6), and case series/reports (n = 6).
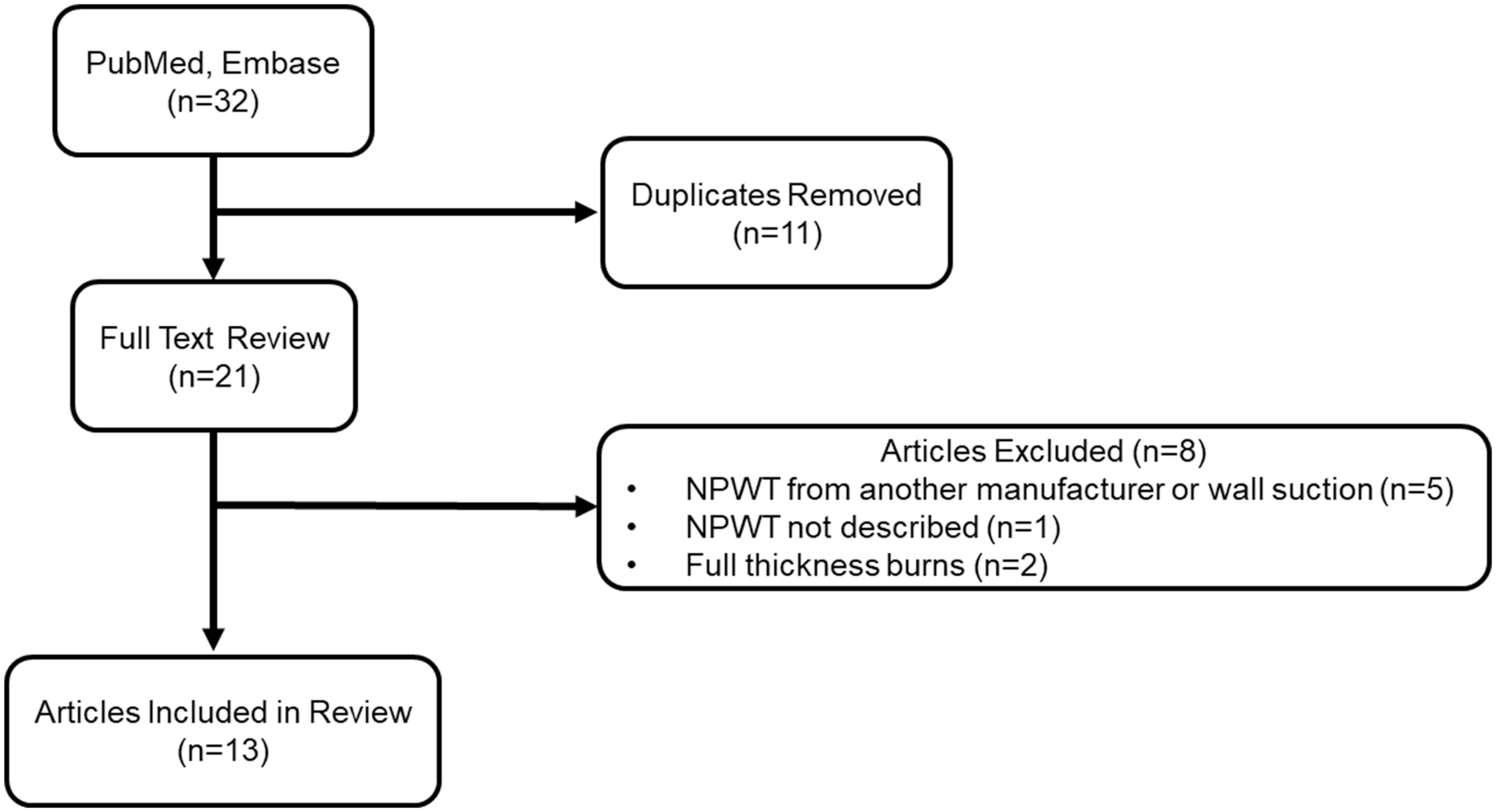
Flow diagram of article selection for review.
Summary of negative pressure wound therapy evidence included in this review
ND, not disclosed.
Summary of negative pressure wound therapy with instillation and dwell time evidence included in this review
ND, not disclosed.
NPWT use in burn management
Use of adjunctive NPWT was reported in a majority of the studies (n = 11) and patients (n = 291, Table 2). 12,13,18 –26 The primary clinical goal of NPWT use was to prepare the exposed soft tissue injury to heal through secondary intention or to bolster a graft following primary closure. Delayed primary closure was the most reported method of wound closure across the 11 studies. Graft uptake, when NPWT was utilized as a bolster, was reported to be >90% across the publications.
The frequency of dressing changes ranged from 2 to 5 days, depending on how NPWT was utilized. Studies where NPWT was used to prepare the wound for grafting reported more frequent dressing changes than those that used NPWT as a bolster. The average duration of therapy ranged from 2.0 to 17.4 days. As burn injuries can be highly variable in size, geometry, anatomical location, and etiology, it is not unexpected that there were differences in the duration of therapy.
The Bloemen et al. RCT assessed 86 patients with thermal burns. Patients received either dermal substitutes alone or followed by skin grafts with and without NPWT. In patients who received NPWT, lower rates of postoperative contamination, reduced erythema, and increased elasticity ratios were observed. Complication rates, graft take, and percent wound epithelialization were similar between all groups. 20 Bloemen et al. demonstrated that functional scar outcomes could be improved if topical NPWT in combination with a dermal substitute was employed. 20
Waltzman and colleagues assessed the use of NPWT as a bolster for partial-thickness skin grafts in 67 patients with third-degree burns resulting from thermal, chemical, electric, or friction burns. 21 Average percent graft take was reported at 99.5% ± 1.5% across all patients and none of the patients returned to the operating room. 21 The authors reported that the ability of NPWT to conform to the wound contours and ability to cover a large surface area contributed to graft securement.
Fischer et al. described NPWT use as a bolster for skin grafts in 12 patients with large surface area thermal burns. 12 A 97% average graft take was reported with no infections. On average, the patient length of stay was 37.9 days. In two patients with TBSA >35% affected by the burn, NPWT use helped reduce the length of stay compared with the average length of stay reported by the American Burn Association for the patient's age and TBSA. 12
A study examining the use of NPWT in 50 patients with thermal, chemical, or friction burns reported an average graft take of 99.2% ± 2.8% and an average postoperative healing time of 16 ± 6 days. 23 Only one patient required regrafting. 23 Eyvaz et al. evaluated the use of NPWT in 39 patients with electrical burns. 25
In this study, NPWT was used for wound bed preparation and as a bolster for skin grafts. NPWT was reported to successfully prepare the debrided burn wound for grafting in 24/27 patients and act as a bolster for initial placement of skin grafts in 7/8 patients and as a bolster for secondary grafting following graft loss in 4/4 patients. 25
Ehrl and colleagues reported that NPWT was a safe and effective modality for management of debrided hand burn wounds. 26 Hand burn patients were assessed, on average, 35 months after injury. A total of 85.1% of patients were able to fully extend their fingers and 78.7% of patients were able to close their fists. For all patients, the mean disability score was 13.8, indicating limited loss of use following the injury. 26
NPWT use within the case series/reports was employed for wound bed preparation after debridement or to bolster skin grafts. 13,18,19,22,24 In these articles, NPWT use was reported to promote the development of granulation tissue, reduce time to closure, remove exudate and infectious materials, and help improve skin graft take.
NPWTi-d use in burn management
Two studies described NPWTi-d application in management of 17 patients with various burn injuries (Table 3). NPWTi-d was utilized to cleanse the debrided burn wound and promote granulation tissue development. Normal saline, quarter-strength Dakin's solution, or mafenide solution was instilled into the wound bed. Instillation dwell times ranged from 6 to 20 min, followed by continuous negative pressure for 3–6 h.
Conditions for NPWTi-d were tailored to the burn etiology and size and depth of the wound. The average duration of therapy ranged from 4 to 10 days across the two studies. The frequency of dressing changes was only reported in one study as every 2–3 days. A step-down approach to traditional NPWT, following definitive closure, was then employed to bolster and protect the reconstructed skin barrier.
Blome-Eberwein et al. reported on the use of NPWTi-d in a total of 15 patients with debrided burn wounds. 27 In these patients, the pain score during NPWTi-d use was an average of 3.20 ± 2.18. The average length of stay was 30.7 ± 29.2 days, time to wound closure was 7.73 ± 4.01 days, and average time to wound healing was reported as 27.5 ± 24.3 days. 27
The Gómez-Ortega et al. case series reported on NPWTi-d use in two patients with electrical burns. 28 NPWTi-d was used to prepare the debrided burn wound for closure and promote development of granulation tissue. In these two patients, use of NPWTi-d resulted in increased development of granulation tissue and wound closure within 4–5 days. 28
DISCUSSION
Burn wounds require prompt intervention and rapid closure of the exposed defect to limit injury progression and circumvent complications. Therefore, any advanced wound care technology considered for use in burn care must address the needs of the burn wound; remove exudate, debris, and infectious materials; promote development of granulation tissue; provide a barrier to external contaminants; and help reduce time to wound closure. NPWT and NPWTi-d may provide clinicians another option for burn wound management.
This review aimed at presenting a broader overview of the current trends in the use of negative pressure-based technologies for management of burn injuries. The goal of NPWT and NPWTi-d use in burn care is to limit bacterial load progression and stabilize the burn injury while preparing the wound for closure through primary intention. The clinical efficacy of the two therapies is not limited to wound size or wound fluid management capacity, which is an additional advantage these modalities have over standard dressings.
Additionally, NPWT and NPWTi-d dressing changes occur every 2–3 days, reducing the frequency compared with standard dressings, which often require daily changes. The NPWT modalities described in this review have excellent potential for burn wound management if one considers the pool of evidence combined with reported outcomes in general wound management studies.
Traditional NPWT works to remove exudate and infectious material, facilitates macro- and microdeformation of the exposed injury to encourage neogenesis of soft tissue, and can be used to bolster a skin graft or flap after placement. NPWT use should be considered in debrided burn injuries when minimal to moderate amounts of exudate are observed within the wound bed or for use as a bolster for skin grafts or dermal substitutes.
Under a closed environment, the physical effect of continuous NPWT decompresses the injury site, while protecting the exposed soft tissue from external contaminants, and helps remove wound exudate and infectious materials. One must also respect the importance of a closed system that facilitates better control and regulation of the wound conditions for patients with compromised wound healing ability.
Adjunctive use of NPWT as a bolster for skin grafts remains the most common usage of NPWT in burn wound management. In the 11 studies identified in this literature review, NPWT use resulted in development of granulation tissue, reduced time to wound closure, and >90% graft take when used over skin grafts. Only the Bloemen et al. RCT reported on groups of burn patients who did not receive NPWT. 20
In this study, the authors reported lower rates of postoperative contamination, reduced erythema, and increased elasticity ratios with NPWT use. However, the RCT's main focus was assessing the effect of dermal substitute use with NPWT on scar quality after burn injury.
In complex nonhealing wounds, health economic assessments have reported increased cost savings with the use of NPWT compared with standard dressings or other negative pressure settings. 29,30 Neither of these health economic assessments included burn wound management; however, their results suggest that the reduced dressing change requirements and system features may help reduce patient cost of care. Despite the limited evidence available, positive clinical results were reported with NPWT use in burn wound patients by 11 studies in this review. Larger, randomized controlled studies are needed to fully assess the clinical and health economic efficacy of NPWT use in burn wound management.
NPWTi-d enables cleansing of the wound, followed by a negative pressure cycle to remove the solubilized debris, slough, infectious materials, and exudate, while promoting development of healthy granulation tissue. NPWTi-d use in burn patients, along with appropriate infection treatment protocols, should be considered if slough, devitalized tissue, debris, high amounts of exudate, or infectious materials are observed in the wound bed.
NPWTi-d use may also be considered if wound bed desiccation is a clinical concern. The functional advantage of NPWTi-d is that the closed system may limit introduction of external contaminants into the wound while providing wound cleansing features. As infection is a fundamental concern for burn patients and establishing a definitive skin barrier promptly is a critical requirement, NPWTi-d shows excellent potential to elevate the effect of NPWT in burn injury management.
However, NPWTi-d is not recommended for use when a dermal substitute or skin graft has been applied. Instillation of a topical wound solution can saturate the skin substitute or graft and inhibit graft take. As such, NPWTi-d is best utilized for wound cleansing and wound bed preparation of the debrided burn injury before use of dermal substitutes or skin grafts.
Limited published data are available for the use of NPWTi-d in burn wound management. Although only two studies reported on NPWTi-d use in burn patients, both studies reported reduced time to closure, with no complications. This indicates that NPWTi-d can safely help with wound bed preparation in patients with burn injuries. Similarly, a recently published meta-analysis investigating the use of NPWTi-d in management of complex soft tissue defects reported consistently shorter time to wound closure compared with standard-of-care techniques, which include conventional dressings and traditional NPWT. 16
Although this meta-analysis incorporated a variety of wound types, it does indicate that NPWTi-d can be used effectively to promote wound healing. Additionally, the outcomes of the meta-analysis were then modeled on actual cost data for patients hospitalized in the United States, the United Kingdom, and Germany. Outcomes reported were fewer resource requirements and earlier patient discharge in patients receiving NPWTi-d compared with standard dressings, which may decrease the cost of wound management. 31
However, this study reported on NPWTi-d use across a hospitalized patient population with undefined wound types. Burn management was not described or the focus of the cost analysis. As such, more investigations are required to fully assess the potential clinical and health economic outcomes following NPWTi-d use in burn wound management.
SUMMARY
Burn wounds require prompt intervention and rapid closure to limit injury progression and complications. A literature review was conducted to assess the use of NPWT and NPWTi-d in management of burn injuries. Positive clinical outcomes following use of NPWT and NPWTi-d were reported by all 13 studies in this review. This review demonstrates that traditional NPWT is the more common negative pressure modality if use is considered in burn injury management protocols.
Increased adoption of advanced NPWT techniques combined with future targeted prospective studies should increase confidence in the advanced therapies. As such, the use of NPWT and NPWTi-d should be considered in management of burn care patients as evidence generation efforts aid in expanding the pool of data accessible to clinicians.
TAKE-HOME MESSAGES
Burn wounds require prompt intervention and rapid closure to limit injury progression and circumvent complications.
Advanced wound care technology considered for use in burn care must address the needs of the burn wound, provide a barrier to external contaminants, and help reduce time to wound closure.
NPWT and NPWTi-d may provide another option for burn wound management.
Footnotes
ACKNOWLEDGMENTS
The author would like to thank Julissa Ramos, PhD, and Julie M. Robertson, PhD (3M Health Care), for assisting with manuscript preparation and critical review. The author thanks Maritza Quintero, PhD (3M Health Care), for manuscript editing and Chris Lessing, PhD (3M Health Care), for his academic guidance and insightful discussions. The author also thanks Christina Hernandez (3M Health Care) for assistance with figure development and production.
AUTHOR CONFIRMATION
The author contributed to the design, development, writing, and reviewing of this work and gave final approval for publication. The author assumes responsibility and accountability for the article.
AUTHOR DISCLOSURE AND GHOSTWRITING
E Nuhiji is a paid employee for 3M Health Care. The author contributed to the writing of this article, no ghostwriters were used.
ABOUT THE AUTHOR
Dr. Nuhiji is a regular keynote speaker at international conferences and has published in several high-impact peer-reviewed journals. Since moving into the medical device industry in 2011, he has developed into a respected specialist in medical affairs, in particular, evidence generation and dissemination projects across Asia Pacific and Europe, Middle East, and Africa.
FUNDING INFORMATION
This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.