
Abstract
Significance:
In trauma care, extensive surgical intervention may be required. Damage control surgery (DCS) is applicable to patients with life or limb-threatening conditions that are incapable of tolerating a traditional surgical approach.
Recent Advances:
The current resuscitation strategy for complex trauma patients includes limiting crystalloid fluids, balanced mass transfusion protocols, permissive hypotension, and damage control resuscitation. Recent technological advancements in surgical critical care have improved outcomes in these critically ill patients.
Critical Issues:
DCS, which is often required in patients with trauma injuries, is typically followed by surgical correction of the injury once the immediate patient survival procedures have been completed. However, DCS and the subsequent injury repair procedures have a high risk for postsurgical complication development.
Future Directions:
Negative pressure therapy modalities can offer clinicians additional adjunctive and cost-effective tools for the management of the trauma care patient, as these systems can be utilized during both the DCS and the postoperative injury management phases of trauma care.

SCOPE AND SIGNIFICANCE
Traumatic injury often requires surgical intervention in a contaminated environment, often involving the removal of foreign objects and debris before definitive closure. Damage control surgery (DCS) has been shown to be applicable for patients with life- or limb-threatening conditions that require life-saving procedures before definitive surgical repair of the injury. 1 –3 Negative pressure wound therapy (NPWT) modalities can offer clinicians additional adjunctive tools for the management of the trauma care patient as these systems can be utilized during both DCS and in the postoperative injury management phases of trauma care.
TRANSLATIONAL RELEVANCE
In trauma care, extensive surgical intervention may be required. Although the trauma surgeon has several available options for patient care, new wound management options are continuously being developed. NPWT systems provide a closed system for wound management that focuses on protecting the wound, closed incision, or open abdomen from the external environment and effectively removing exudate and infectious materials that may detrimentally affect healing. 4,5 This review provides an overview on the current state of trauma care and how negative pressure therapy (NPT) can fit into the patient management plan.
CLINICAL RELEVANCE
When thoracic trauma patients present for care, measures are taken to stabilize breathing and blood loss. Once the patient is stable, a secondary evaluation occurs to identify the presence of life-threatening injuries, and once stabilized, the patient may more safely undergo a definitive surgical correction of the inciting injury. 6 –9 In DCS patients, the severity of the injury and level of wound contamination often confer a higher risk for postsurgical complications and infections in the subsequent injury repair procedures. 10 –12 NPT modalities may offer trauma surgeons an additional tool to help manage these high-risk trauma patients.
BACKGROUND
Patients with trauma injuries often require extensive medical care resulting in high costs. In 2019, the estimated cost of traumatic injury was $4.2 trillion, with more than half the cost attributed to adults aged 25–64 years. 13 These cost estimates include $327 billion for medical care, $69 billion in work loss, and $3.8 trillion in statistical life and quality-of-life losses. 13
In the United States, a total of 181,194,431 traumatic injury patient discharges occurred between 2006 and 2012. 14 More recently, travel restrictions during the COVID-19 pandemic reduced levels of trauma admissions across 18 states (89,813 in 2019 vs. 84,123 in 2020). 15 However, these trauma injuries were associated with longer length of stay (LOS), increased injury severity, and a higher mortality rate. 15
Thoracic trauma has been estimated at 20–25% of all trauma patients worldwide and is the third most common cause of death in polytrauma patients. 16 When thoracic trauma patients present for care, they are initially assessed, and measures are taken to stabilize breathing and blood loss. A secondary patient evaluation is then conducted including hematologic and metabolic laboratory studies and diagnostic imaging to identify the presence of life-threatening injuries. 6 Patients are then started on intravenous antibiotic therapy as these wounds are often contaminated, resulting in an increased chance for infection.
In patients with a life-threatening injury, removal of a foreign object from a penetrating injury followed by exploratory surgery, DCS, and wound closure with flaps or grafts often occurs. In patients with non–life-threatening injuries, debris is cleansed from the wounds, steps are taken for hemostasis, followed by wound closure techniques (surgical closure, closure by secondary intention, etc.).
Damage control surgery
The term “damage control” was originally used to define efforts to salvage a naval vessel. 17 More recently, damage control has been used to describe the use of staged medical interventions following life-threatening trauma injury with a priority for interventions to preserve the patient's life before damage repair is undertaken. Various early iterations of DCS were first reported in the management of combat injuries in the 1900s. 18 By 1982, Kashuk et al. were the first to describe the “vicious cycle” of hypothermia, coagulopathy, and acidosis observed in patients with major abdominal vascular injuries. 19 The authors believed each component was affected by the others and all had equal importance to the initial resuscitation efforts and operative control. One year later, Stone recommended the use of the “truncated laparotomy” when intraoperative coagulopathy was noted. 20 Stone et al. immediately stopped surgery when the patient developed a significant coagulopathy and turned their focus to restoring hemostasis with plans to finish the surgery when the patients were more stable. By the 1990s, Rotondo further defined the concept of DCS, which has since become a vital tool in trauma surgery (Fig. 1). 1,2 Abdominal DCS has three phases: rapid control of life-threatening hemorrhage and contamination with temporary abdominal closure (TAC), either static or dynamic 21,22 ; resuscitation and correction of physiologic derangements, this is initiated in the operating room (OR) and continued in the intensive care unit (ICU); definitive management of injuries and closure of the abdomen. 2,21,22
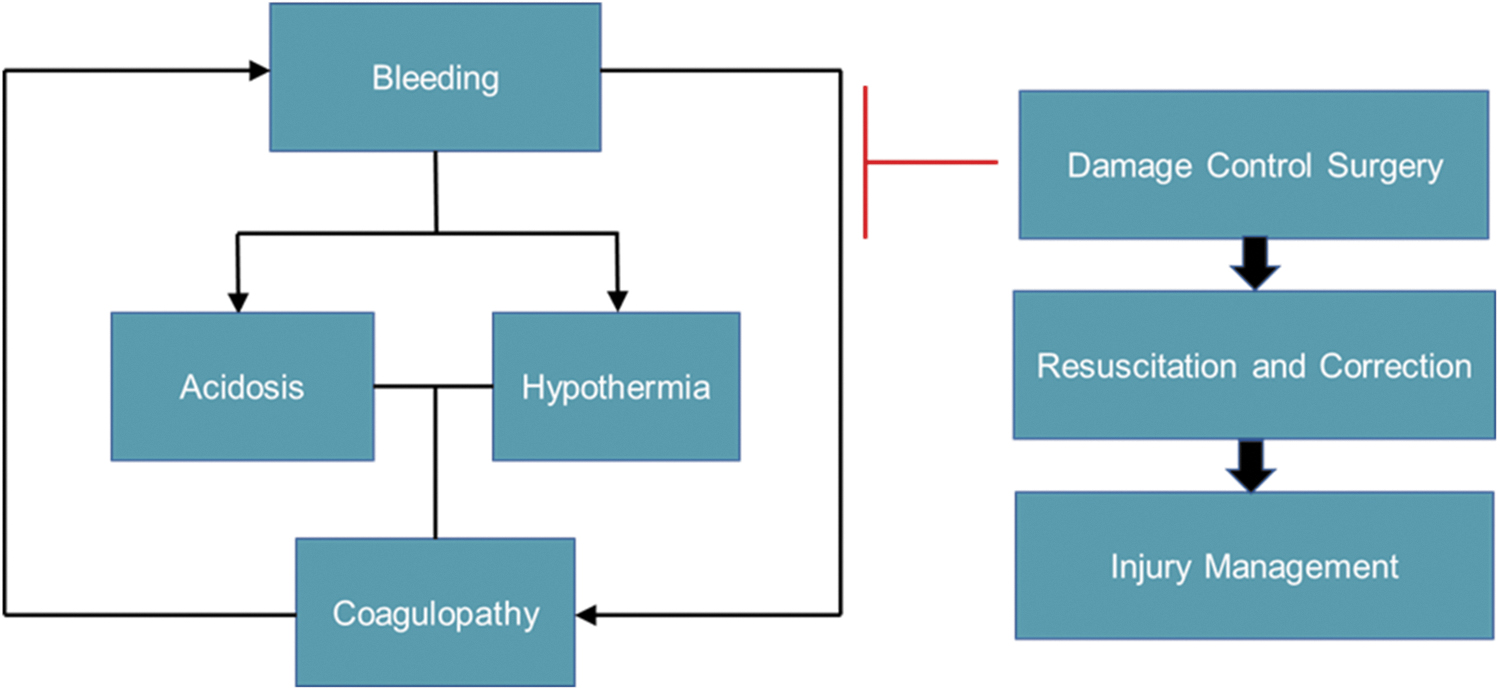
Role of DCS in patient care. DCS restores hemostasis and allows for the patient to undergo resuscitation and correction of physiological derangements caused by the trauma, followed by injury management at a later date. DCS, damage control surgery.
General trends in DCS
Initially described in exsanguinating truncal trauma and visceral injury, DCS has been shown to be a treatment modality that may be applicable for any patient with life- or limb-threatening conditions, incapable of tolerating a more traditional surgical approach. 1 –3,23 These patients may have a severe degree of physiologic insult in the preoperative or intraoperative setting. An expert panel review found that the most reported indications for DCS were as follows: hypothermia (temperature <34°C); clinical or laboratory evidence of coagulopathy; evidence of persistent cellular shock (pH <7.2, base deficit >15 M, lactate >5 mM O2 consumption index <100 mL/min/m2); prothrombin time and partial thromboplastin time >1.5 times normal and absence of visible blood clots during operation or diffuse oozing from injured tissues; and development of intraoperative ventricular arrhythmias. 3
DCS may be applied to a variety of conditions, from trauma to the septic abdomen, owing to its underlying simplicity and efficacy. The DCS concept has expanded outside the abdomen and evolved to include damage control thoracotomy and orthopedic damage control, which are often performed in the polytrauma patient. 8,9,24 –27 An early and rapid identification of the shock state is fundamental coupled with an abbreviated index operation, closure and transfer to the ICU for further resuscitation before definitive repair, and fascial closure at subsequent operations. 8,9,24 –27
The current resuscitation strategy for complex trauma patients includes limiting crystalloid fluids, balanced mass transfusion protocols, permissive hypotension, and damage control resuscitation. Recent technological advancements have been developed for surgical critical care, such as modern variable ventilator modes, more effective, adjunctive hemostatic agents, and core body temperature regulation devices. Together, these resuscitation strategies and technological advancements have improved outcomes in these critically ill patients. 17,23
USE OF NEGATIVE PRESSURE THERAPIES IN THORACIC TRAUMA
Traumatic injury often requires surgical intervention. NPT can offer clinicians additional tools for wound management in the trauma care patient. Negative pressure therapies can be utilized during both the DCS and the injury management phases of trauma care.
Traditional negative pressure wound therapy
Traditional negative pressure wound therapy (NPWT; 3M™ V.A.C.® Therapy; 3M Health Care, St. Paul, MN) uses foam dressings to apply negative pressure across the wound bed allowing for the removal of exudate and infectious materials, drawing the wound edges together, and promoting granulation tissue development and local tissue perfusion. 28 Traditional NPWT can be used with a reticulated open cell foam dressing (ROCF) with or without silver (3M™ V.A.C.® Granufoam Silver™ Dressing or 3M™ V.A.C.® Granufoam™ Dressing; 3M Health Care), or a polyvinyl alcohol dressing (3M™ V.A.C. ® Whitefoam™ Dressing; 3M Health Care), which can be placed into explored tunnels and areas of undermining.
Open abdomen NPT
Open abdomen negative pressure therapy (OA-NPT, 3M™ AbThera™ Open Abdomen Negative Pressure Therapy; 3M Health Care) combines TAC with continuous negative pressure to remove fluid from the abdominal cavity, draw fascial edges together, and help protect the abdominal contents from external contamination. 29 –31
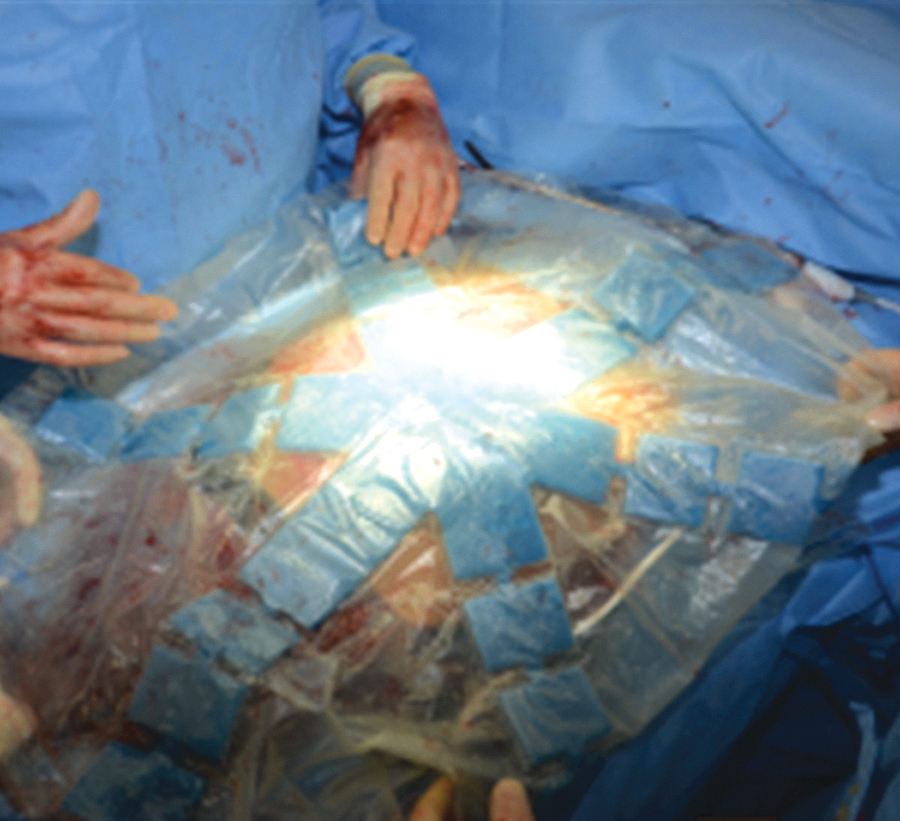
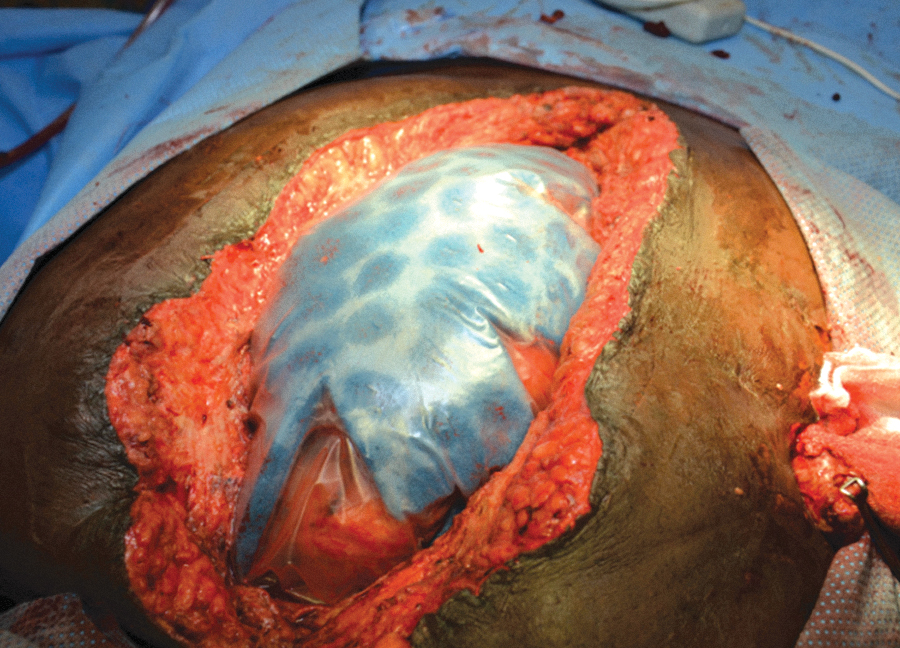
OA-NPT is used with a nonadherent fenestrated polyurethane layer (3M™ AbThera™ Fenestrated Visceral Protective Layer; 3M Health Care) that separates the bowel viscera from the abdominal wall and distributes negative pressure throughout the open abdomen to facilitate fluid removal from the paracolic gutters (Figs. 2 –4). OA-NPT can be used with either a perforated hydrophobic, ROCF dressing (3M™ AbThera™ Perforated Foam; 3M Health Care) or a collapsible ROCF dressing (3M™ AbThera™ Advance Perforated Foam, 3M Health Care). These dressings provide a uniform distribution of negative pressure to the nonadherent polyurethane layer to help aid with fluid removal (Figs. 5 and 6). Under negative pressure, these dressings provide medial tension to help reduce fascial retraction and loss of domain. 29 –31 The collapsible foam dressing was designed to collapse medially while maintaining vertical rigidity under negative pressure to actively facilitate drawing the wound edges together (Fig. 7).
Fenestrated polyurethane layer.
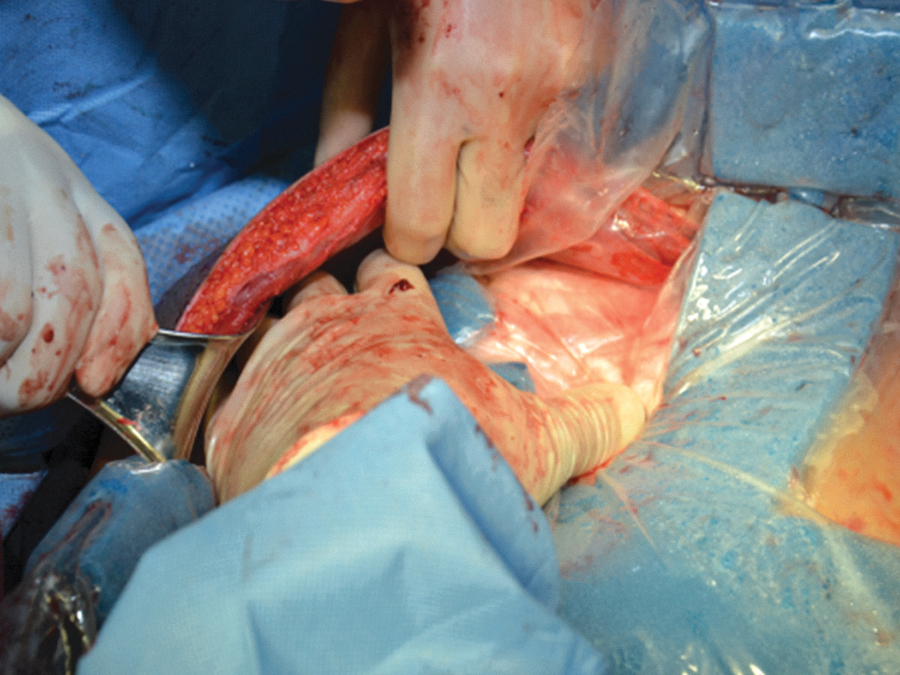
Placement of the fenestrated polyurethane layer into the abdominal cavity, ensuring contact with paracolic gutter.
Example of proper placement of the fenestrated polyurethane layer.
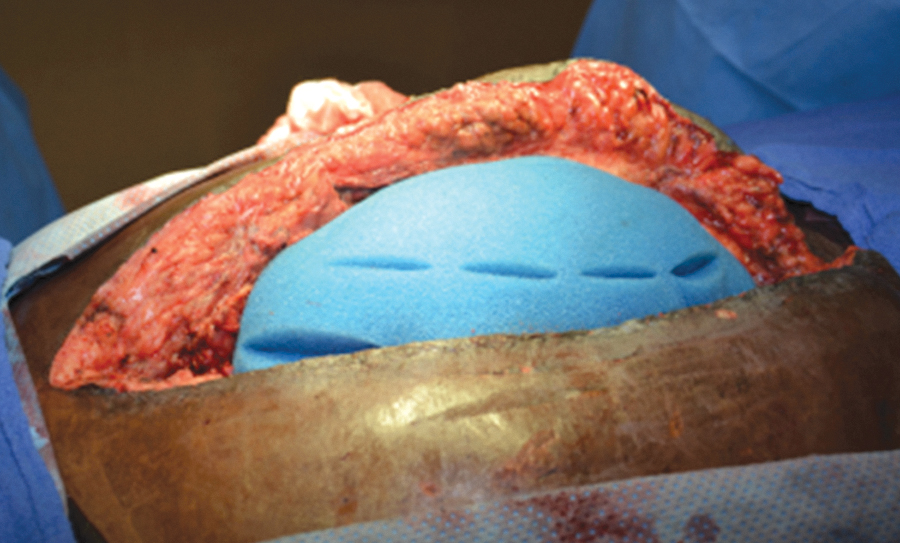
Application of OA-NPT foam dressing over the fenestrated polyurethane layer. OA-NPT, open abdomen negative pressure therapy.
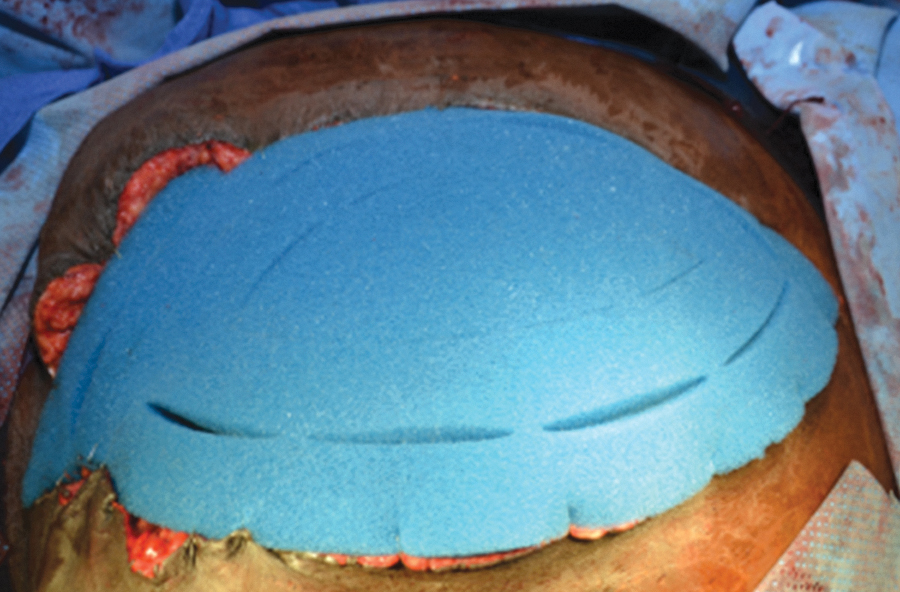
Application of a second OA-NPT foam dressing so that dressing is flush with skin level.
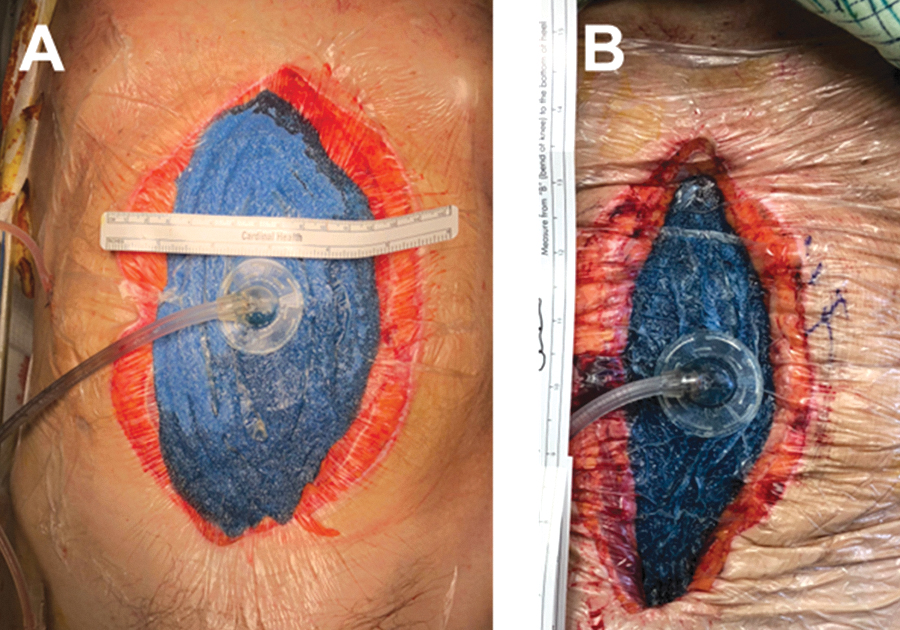
Example of OA-NPT dressing drawing wound edges together.
NPWT with instillation and dwell time
NPWT has evolved to include wound cleansing capabilities. This negative pressure wound therapy with instillation and dwell time (NPWTi-d [3M™ Veraflo™ Therapy; 3M Health Care]) utilizes a topical wound solution that is instilled into the wound bed for a user-determined amount of time and is removed during the negative pressure cycle. NPWTi-d cleanses the wound bed, dilutes, and solubilizes infectious material and debris, removes exudate and infectious material, and promotes granulation tissue development.
Four dressings are available for use with the NPWTi-d system. These dressings are less hydrophobic than the traditional NPWT dressings allowing for even distribution of the topical wound solutions across the wound bed. 32 Each dressing type has its own benefits and features allowing the clinician to tailor NPWTi-d to the needs of the wound. NPWTi-d dressings (3M™ V.A.C. Veraflo™ Dressing; 3M Health Care) can be used for open wounds with shallow undermining or tunnel areas. Cleansing dressings (3M™ V.A.C. Veraflo Cleanse™ Dressing; 3M Health Care) can be used for complex wound geometries including explored tunnels or undermining. 33,34 Dressings with through holes (3M™ V.A.C. Veraflo Cleanse Choice™ Dressing; 3M Health Care) are used when thick exudate is present and is a 3-piece dressing. The one-piece dressing with through holes (3M™ Veraflo™ Cleanse Choice Complete™ Dressing; 3M Health Care) is also used for wounds with thick exudate; however, this version consists of one dressing piece allowing for quick application.
The combination of NPWTi-d with the dressings containing through holes provide hydromechanical removal of infectious materials, nonviable tissue, and wound debris, which reduces the number of surgical debridements required, in addition to promoting granulation tissue development. 35,36
Several topical wound solutions are available that can be used with NPWTi-d. These include normal saline, hypochlorite-based solutions, silver nitrate (0.5%), sulfur-based solutions, biguanides (polyhexanide), and topical lidocaine. 33 –37 No instillation solution is superior to another; however, a recent consensus publication did recommend normal saline for most wounds and use of a topical antiseptic solution for wounds with acute infection or high levels of bacterial colonization when infection management protocols are also used. 37
Closed incision NPT
Another iteration of NPWT is closed incision negative pressure therapy (ciNPT; 3M™ Prevena™ Incision Management System; 3M Health Care). ciNPT utilizes foam dressings to apply negative pressure over clean, closed incisions and the surrounding soft tissue. The dressings available are anatomically adaptable and can remain in place for up to 7 days. ciNPT helps manage and protect surgical incisions and surrounding tissue by protecting the incision from external contaminants, helping to hold the incision edges together, decreasing lateral tension on the incision, reducing edema, and removing fluids and infectious materials. 38 –41 A variety of dressings with different shapes and sizes are available for use with ciNPT. These include a customizable dressing (3M™ Prevena™ Plus Customizable Dressing; 3M Health Care), which can be cut to fit the incision length, an integrated one-piece dressing available in three different lengths (3M™ Prevena™ Peel and Place Dressing; 3M Health Care), and multiple size and shape offerings with expanded coverage area to help manage the incision and surrounding tissue envelope (3M™ Prevena Restor™ Dressings; 3M Health Care). 38 –41
USE OF NEGATIVE PRESSURE THERAPIES IN TRAUMA CARE
For traditional NPWT, early use (1 or 2 days from admission) in traumatic wounds was shown to significantly reduce LOS, treatment duration, ICU stay, and total and variable costs per patient discharge compared with patients who received NPWT on day 3 or later. 42
NPWTi-d can also be beneficial for use in traumatic wounds for wound cleansing, providing hydromechanical removal of debris, exudate, infectious materials, and nonviable tissue. NPWTi-d can also help promote granulation tissue development that can reduce the time to final closure in traumatic wounds. 43 –45 Early use of NPWTi-d (within 1 day of admission) was also associated with reduced treatment length, LOS, number of surgical debridements, OR visits, days until final OR procedure, and wound-related readmissions compared with late use of NPWTi-d (within 7 days of admission). 45 In addition, a $10,877 reduced mean cost of index admission was also associated with early NPWTi-d use. 45
In trauma patients requiring open abdomen management, OA-NPT can provide clinicians with a TAC option that allows for access to the abdominal cavity while protecting the abdominal contents and helping to reduce loss of domain. In patients undergoing emergency laparotomy, use of OA-NPT resulted in primary fascial closure with no increase in intra-abdominal pressure or development of other gastrointestinal complications. 46 Similarly, a systematic review reported high rates of fascial closure with commercial OA-NPT systems compared with other open abdomen temporary closure methods. 47 A meta-analysis of OA-NPT found reduced postoperative mortality rates and length of ICU stay in patients who received OA-NPT methods compared with patients who did not receive OA-NPT. 48 A retrospective study reported significantly higher number of OA-NPT patients who underwent midline fascial closure compared with the Barker technique for TAC. 31 In addition, the authors suggested that the added cost of OA-NPT was offset by the improved patient outcomes and cost-savings from fascial closure. 31
Use of ciNPT following surgical closure of trauma injuries may also provide a clinical benefit to patients. A retrospective single-institution cohort study reported that with use of ciNPT following chest wall reconstruction after sternal and/or rib fractures, none of the 71 patients developed surgical site infection during hospitalization or within 2 months of discharge. 49
CONCLUSION
In complex thoracic traumatic injury, use of NPWT modalities (including traditional NPWT, OA-NPT, NPWTi-d, and ciNPT) promote granulation tissue development, help reduce loss of abdominal domain, cleanse the wound bed, and manage the closed surgical incision and surrounding soft tissue resulting in positive clinical benefits for trauma patients.
SUMMARY
Thoracic trauma has been estimated at 20–25% of all trauma patients worldwide. 16 When thoracic trauma patients present for care, patient stabilization methods are initially used followed by management of the trauma injury. 6 In patients with a life-threatening injury, removal of a foreign object from a penetrating injury followed by exploratory surgery, DCS, and wound closure with flaps or grafts often occurs.
NPT can offer clinicians additional tools for the management of a trauma care patient as they can be utilized during DCS and injury management phases of trauma care. Traditional NPWT applies negative pressure across the wound bed allowing for the removal of exudate and infectious materials, drawing the wound edges together, promoting granulation tissue development and local tissue perfusion. NPWTi-d can also be beneficial for trauma wounds needing cleansing as it provides hydromechanical removal of debris, exudate, infectious materials, and nonviable tissue. For patients requiring open abdomen management, OA-NPT can provide clinicians with a TAC option that allows for access to the abdominal cavity while protecting the abdominal contents and helping to reduce loss of domain. ciNPT use following surgical closure of trauma injuries may also provide a clinical benefit to patients by maintaining a barrier to external contamination, helping hold the incision edges together, decreasing lateral tension on the incision, reducing edema, and removing fluids and infectious materials.
TAKE HOME MESSAGES
Thoracic trauma has been estimated at 20–25% of all trauma patients worldwide.
In patients with life-threatening injury, DCS has allowed the use of staged medical interventions to preserve the patient's life before damage repair is undertaken.
Negative pressure therapies can offer the trauma surgeon additional tools in the management of complex trauma patients.
Footnotes
ACKNOWLEDGMENT
The author thanks Julie M. Robertson, PhD (3M Health Care) for assistance with article preparation and editing.
AUTHORs' CONTRIBUTION
The author contributed to the design, development, writing, reviewing of this work, and gave final approval for publication. All authors assume responsibility and accountability for the article.
AUTHOR DISCLOSURE AND GHOSTWRITING
Dr. Fernández is a consultant for 3M Health Care. All authors contributed to the writing on this article, no ghostwriters were used.
FUNDING STATEMENT
This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
ABOUT THE AUTHOR