
Abstract
Significance:
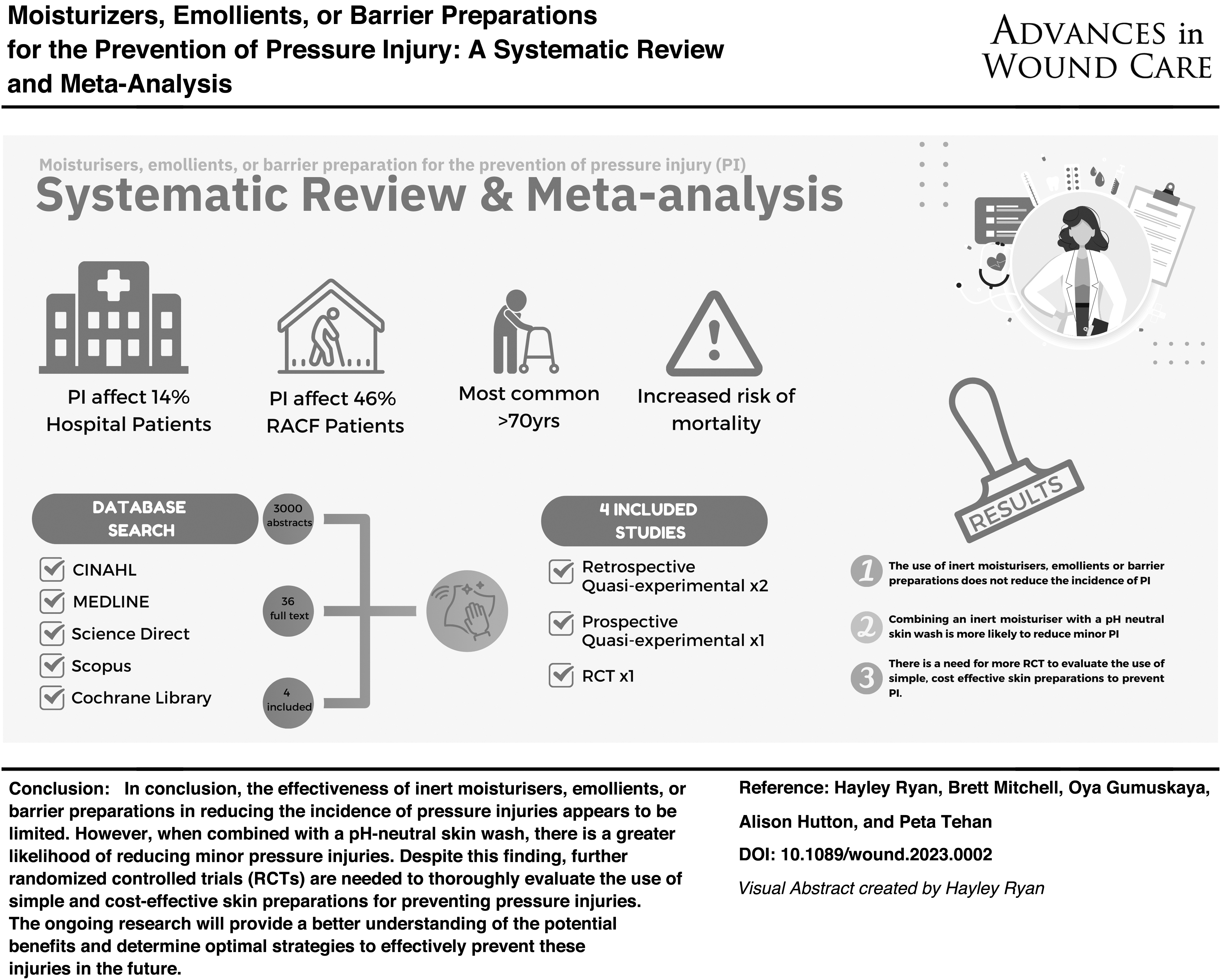
Pressure injuries are prevalent, yet preventable global health care problem estimated to affect 14% of hospital patients and up to 46% of aged care residents. One common prevention strategy is improving skin integrity through emollient therapy to optimize hydration and avoid skin breakdown. Therefore, this study aimed to review the literature and determine effectiveness of inert emollients, moisturizers, and barrier preparations compared with standard care, to prevent pressure injury in aged care or hospital settings.
Recent Advances:
Search terms were derived with database searches, including ProQuest, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Medline, Science Direct, Scopus, and the Cochrane library. The Robins1 and Risk of Bias 2 (Rob2) quality appraisal tools were used. A meta-analysis of the effects of interventions was conducted (random effects). Four studies met the inclusion criteria, with heterogeneous quality. Pooling of nonrandomized studies found that the application of emollients, moisturizers or barrier preparations did not significantly reduce incidence of pressure injury compared with standard care (relative risk 0.50, 95% confidence interval: 0.15–1.63, Z = 1.15, p = 0.25).
Critical Issues:
This review suggests that the use of inert moisturizers, emollients, or barrier preparations for preventing pressure injuries was not effective to prevent pressure injury in aged care or hospital settings. However, there was a distinct lack of randomized controlled trials (RCTs), with only one meeting the inclusion criteria. Furthermore, most of the included studies did not report on the frequency of application of the product, making it difficult to determine if application was in line with current international guidelines. One included study, which utilized a combination of neutral body wash and emollient demonstrated a significant reduction in the development of stage one and two pressure injuries. This combination of care may further support skin integrity and should be further examined in future trials.
Future Directions:
Future studies should ideally be RCTs, which control for skin cleansing, and implement an inert moisturizer emollient or barrier preparation as part of a pressure injury reduction bundle of care. Standardization of the application of the product, the volume of product applied at each application, and the quality of the product should also be considered.

SCOPE
It is incredibly important that wound care clinicians have access to level one evidence that evaluates interventions, which are commonly utilized in their practice. This review provides a thorough appraisal of evidence pertaining to the use of moisturizer, emollient, and barrier preparations for the prevention of pressure injury in aged care or hospital settings. These strategies are commonly utilized in aged care and hospital settings due to their simplicity, accessibility, and cost effectiveness. This review demonstrates that the use of these preparations alone does not significantly reduce the incidence of pressure injury.
TRANSLATIONAL RELEVANCE
There is a need for more randomized controlled trials (RCTs) to evaluate the effectiveness of inert skin care regimens, such as moisturizers, emollients, or barrier preparations, to prevent pressure injury in hospital and aged care settings. Further investigation of optimization of skin integrity could also be measured in future studies utilizing these simple, cost-effective skin care preparations, which are broadly used in clinical practice.
CLINICAL RELEVANCE
The prevention of pressure injury in aged care and hospital settings is of the utmost importance given the high prevalence of pressure injury in these settings. 1 Clinicians should consider the use of moisturizers, emollient, and barrier preparations in conjunction with a broader skin care regimen to effectively prevent pressure injury. The use of a pH neutral soap will further support the skin and optimize the integrity to improve capacity to manage shear and pressure.
BACKGROUND
Pressure injuries are a prevalent global health care problem, 2 estimated to affect 14% of hospital patients 3 and up to 46% of aged care residents. 4 Pressure injuries most commonly occur in patients over the age of 70, those with spinal cord injury, malnourished, or intensive care patients. 5,6 Pressure injuries can be painful, negatively impact quality of life, and pose a significant financial burden on the health care system. 4 Furthermore, pressure injuries can result in hospital admissions, increased length of hospital stay, and increased mortality. 7 Pressure injuries are largely preventable, particularly if individuals at risk are identified early to enable prevention strategies to be implemented. 1
Identifying individuals at high risk is done using validated pressure injury risk assessment tools such as Braden or Waterlow scales. 8 Risk assessment tools assist with triaging appropriate and timely pressure injury preventative care to avoid skin deterioration and wound development. 1 While risk assessment tools are considered an essential component to implement pressure injury prevention strategies, use of the tools alone is not adequate to reduce incidence of pressure injury. 1 The prevention of pressure injury requires a multifaceted approach, which may include regular repositioning, early mobilization, implementing appropriate support surfaces, nutrition assessment and management, and preventative skin care. 9
Preventative skin care focuses on optimizing skin integrity to prevent skin breakdown. This includes strategies, such as keeping skin clean and appropriately hydrated, avoiding use of alkaline soaps and cleansers, cleansing the skin promptly after episodes of incontinence, and protecting skin from excess moisture with barrier products. 2 This is particularly important in older people, where age-related skin deterioration further complicates skin integrity. Thinning of the epidermis and dermis results in increased vulnerability to mechanical trauma, particularly shearing and friction, making skin more susceptible to injury and breakdown. Multiple studies have described friction as a factor that leads to stage I and Stage II pressure injuries, 10 with shear and pressure leading to deeper, stage III and IV pressure injuries.
It is proposed that by optimizing skin integrity through the use of emollients and other preparations, that skin is more resilient to friction forces and therefore may contribute to reducing pressure injuries.
Further age-related skin changes include atrophy of sweat glands, reduced stratum corneum lipids, structural changes to the stratum corneum, and reduced movement of water from dermis to epidermis, all of which contribute to dry skin and xerosis. It is therefore critical that aging skin is consistently rehydrated and sealed to maintain hydration. Emollients aid the barrier function of the skin as they improve the oil and lipid levels, restore protective function, 11 and reduce damage, such as fissuring. 12 The use of moisturizers increases epidermal water content, with lotions also having been proven effective for treatment of xerosis, and barrier preparations may also assist optimize skin integrity. 13
While the use of emollients, barrier wipes, and moisturizers in clinical practice may be beneficial in reducing pressure injury incidence, clinicians have expressed confusion and a lack of knowledge on different topical treatments due to the large variety currently available. 14,15 Chan et al. further confirmed this in their cross-sectional study, demonstrating the wide variety of emollient formularies available across the United Kingdom, and the increased risk of confusion for prescribers. This research also elicited that cost, and patient preference was the most common reasons for recommending a specific emollient type. 5
It has been recommended that only a small number of cost-effective emollients should be available in clinical practice that are proven to be effective. 16 In addition, previous research has been inconclusive or conflicting in determining the best topical preparation for protecting skin integrity from breakdown. 16 A previous study by Lewis-Byers and Thayer indicated that a no-rinse cleanser and a barrier cream combined was superior to soap and water combined with moisturizer for protecting skin integrity. 17
A prospective study by Bale et al., which compared the effect of two skin care protocols on skin condition, showed that implementing a skincare regime that included a spray cleanser, barrier creams, and barrier films resulted in fewer stage I pressure injuries to the buttocks, sacrum, and ischial tuberosities compared with usual care. 14
Skincare products can vary in their formulation and be considered as containing active ingredients, or can be classified as inactive (inert). Inert products are more commonly used in hospital and aged care settings, 18 and function by creating an impermeable layer on top of the skin, which inhibits transepidermal water loss. 19 For the purposes of this review, to compare and pool products of similar formulation and action, it was decided that only inert (inactive) preparations would be included. Therefore, there is a need to understand the current evidence and effectiveness of inert moisturizers, emollients, or barrier preparations to prevent pressure injury in aged care and hospital settings.
This study aims to systematically review the evidence on inert moisturizers, emollients, or barrier preparations, compared with standard care to prevent pressure injury in adults in aged care or hospital settings and evaluate the overall effect of inert moisturizers, emollients, or barrier preparations on the prevention of pressure injuries.
METHODS
This systematic review was developed according to the recommendations described in the preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines. 20 This systematic review protocol has been registered with the international prospective register of systematic reviews, PROSPERO. The registration number is CRD42021226550. Before registration, the protocol was reviewed by three researchers and assistance provided by a University Librarian.
Search strategy
Databases searched were the Cumulative Index of Nursing and Allied Health Literature (CINAHL), Medical Literature analysis and retrieval system online (MEDLINE), ScienceDirect, Scopus, ProQuest, and the Cochrane library. Search terms were derived for MEDLINE (Table 1) and adjusted for other databases accordingly. No language or date limiter was applied, with studies from the inception of each database until the 6th of June 2022 included. Reference lists of relevant articles were also hand searched for potentially pertinent suitable articles.
MEDLINE search strategy
Inclusion and exclusion criteria
Studies published in English and conducted in adult populations (>18 years of age) were included. Studies that were conducted in residential and aged care facilities and hospital settings were included only. Residential aged care facilities were defined as long-term care facilities, aged care, nursing homes, and residential aged care. Interventions were limited to barrier preparations (films, creams, wipes), inert moisturizers, and/or emollients, as defined by the Prevention and Treatment of Pressure ulcer/Injuries clinical practice guideline. 2 Study designs included randomized control trials, case–control, quasi-experimental, and cohort studies.
Studies conducted on participants with spinal injuries or incontinence-associated dermatitis as the primary outcome of interest were excluded, as the clinical management of these conditions differs substantially, therefore, introduces substantial heterogeneity. Studies focused on management of existing pressure injuries were not eligible for inclusion. Studies comparing two different types of emollient creams, barrier wipes, moisturizers, and did not have a control group were excluded as they did not answer the aim of this study.
Other exclusions were studies undertaken in community or outpatient settings and interventions that use cosmetic products as the primary intervention. Studies using products, which were considered active, such as hyperoxygenated fatty acid oils, were gel based, or were oils, were not included. Studies that used a combination of methods to manage or prevent the incidence of pressure injury, where the individual effect of barrier creams, barrier wipes, moisturizers, emollients, or barrier films were not identifiable, were also excluded.
Study selection and data extraction
The two authors (H.R. and P.T.) independently conducted the literature search and extracted the title and abstract data into Covidence®. Two authors (H.R. and P.T.) then independently screened the titles and abstracts for inclusion according to the criteria. If differences arose, a third party (B.M.) judged the abstract for inclusion or exclusion. Full texts of relevant studies were then obtained, and two authors independently screened these for relevance (H.R. and P.T.) with differences judged by a third party (B.M.). Articles deemed to have relevant data for the systematic review and meta-analysis were then included.
A data extraction table was formulated, and two authors, independent of each other, completed the data extraction (H.R. and P.T.). For each eligible study, the following data were extracted: author, year of publication, study design, setting, control group, intervention group, mean age and range, intervention, comparator, product specifications, outcomes, anatomical location of the wound, pressure injury grading system, randomization information, and an overview of the results (Supplementary Material S1).
Quality appraisal
Quality and risk of bias for the included articles were assessed independently by two authors using two tools, depending on the study design. Version two of the Cochrane risk-of-bias tool for randomized trials (RoB 2) was used for the randomized controlled studies. 21 For nonrandomized control studies, the ROBINS-I tool was used. 22 These tools were selected as they are considered to be reputable and robust. There was a need to utilize two quality appraisal tools due to the inclusion of nonrandomized trials.
Analysis and synthesis
All data extracted were managed on an excel spreadsheet and are presented in a comprehensive, evidence-based table (Supplementary Material S1), where the evidence is synthesized and summarized. Pooling and analysis of data was carried out using Review Manager software (RevMan 5.3; Cochrane Collaboration, Oxford, UK). A meta-analysis of the effects of the interventions was conducted. A random-effects model for meta-analysis was used. This method incorporates the error of estimates within studies and the weight of the study on the expected outcome.
The heterogeneity among the studies was assessed, the I 1 statistic was used to determine the degree of heterogeneity, and interpreted in line with Cochrane recommendations 23 (0–40% might not be important, 30–60% may represent moderate heterogeneity, 50–90% may represent substantial heterogeneity, and 75–100% considerable heterogeneity). 24 Assessment of publication bias was assessed using a funnel plot (Supplementary Appendix SA1).
RESULTS
The database search identified 3,000 citations. Following title and abstract screening, 36 studies were deemed appropriate for full-text review and assessed for eligibility. Four studies met the inclusion criteria and were included in the review (Fig. 1).
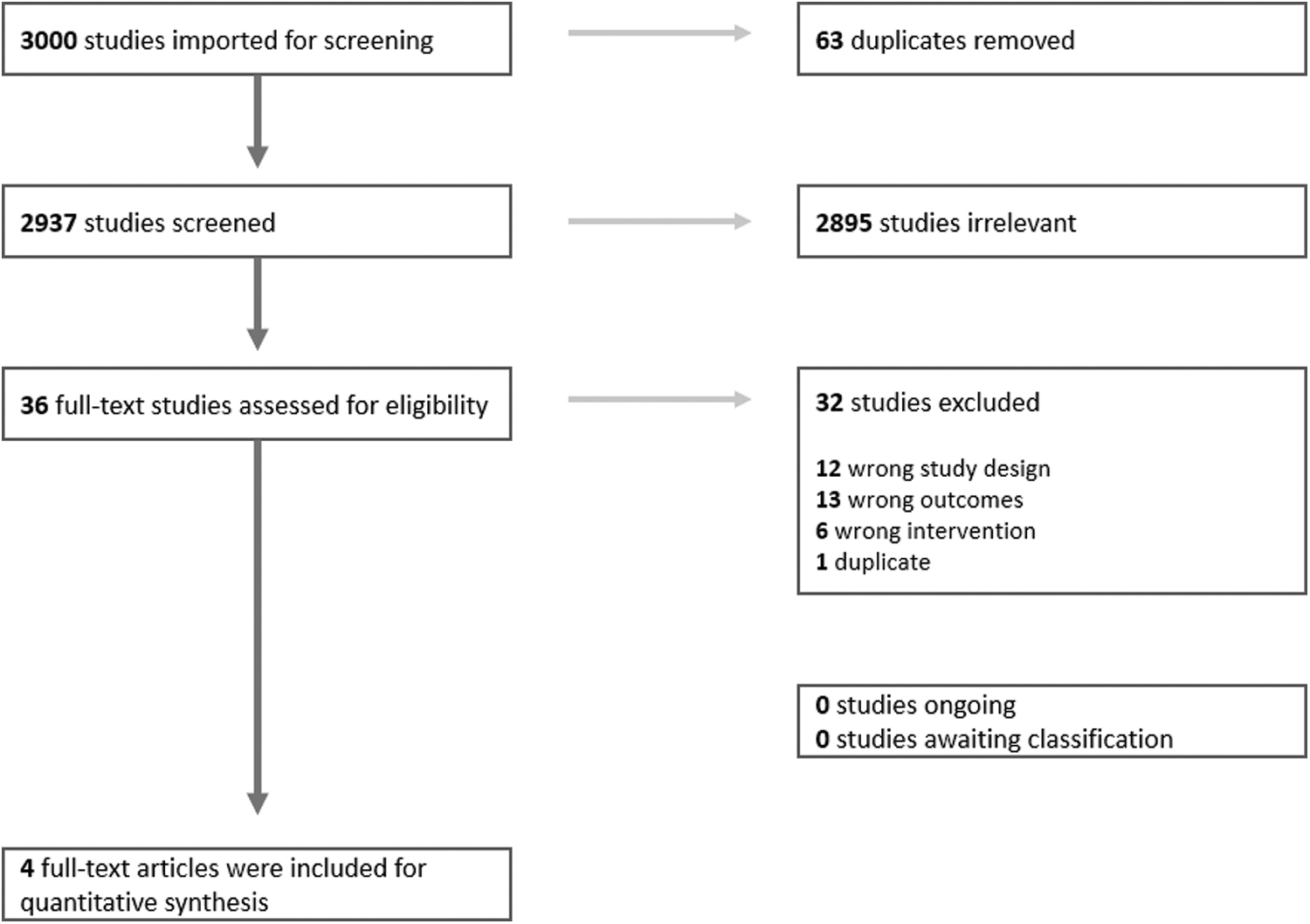
PRISMA Flowchart of articles identified and included for analysis and synthesis.
General characteristics and overview of included studies
Study designs of the included studies were varied, two were retrospective quasi-experimental, 25,26 one was prospective quasi-experimental pretest/posttest design study, 27 and one was a RCT. 28
Participant numbers ranged between 47 participants, (18 in the control group, and 29 in the intervention group), 28 and 136 participants (136 in the control and 136 in the intervention group). 27 Three studies included elderly patients within long-term care facilities, 25,27 –29 and one study included elderly patients in a hospital setting. 26 Participant age range was 65 to 100. Clever et al. had both the youngest and oldest reported age. 25 One study did not report age range. 26 Three of the four studies were conducted in the United States of America, 25 –27 and one in the Netherlands. 28
Interventions
Study interventions all aimed to reduce incidence of pressure injury. The interventions used in the included studies were heterogeneous, and included a range of topical products, including a generic emollient, 26 a moisturizer—(dimethyl sulfoxide 5%), 28 and two barrier preparations (Table 2). 25,27 Application of the emollient, moisturizer, and barrier preparations was also heterogeneous, with included studies having product applied by either a hospital 24 or aged care staff member, the resident or their carer. 25,27,28 The amount of product used was not able to be determined from any of the included studies. No barrier wipes as interventions were used within the included studies. The intervention in the study by Hunter was a skin care regimen, which included the use of a barrier preparation in conjunction with neutral body wash. The neutral body wash was considered standardization of the participants' skin cleansing regime, rather than an independent intervention.
Intervention topical agents
The reporting of the comparator (or control) arm of each study was varied. One study simply described the pressure injury prevention protocol, which was standard in the facility, which included daily skin assessment, use of standard pressure-reducing support surfaces, repositioning program, dietary monitoring, treatment of comorbidities, and use of pads or briefs for incontinence. 25
The study by Hunter et al. reported standard nursing care as the control arm. This consisted of assessment of risk of pressure injury with the Braden Scale, relieving localized pressure, use of support surfaces, regular repositioning, hydration therapy, and nutrient supplements. Furthermore, in cases of incontinence and high risk of skin breakdown, additional measures were put in place, which included the use of a barrier cream in the affected areas.
In Shannon's (2009) retrospective quasi-experimental study, the preintervention arm was described as standard care, which consisted of education, pressure redistribution, nutrition, and timely removal of urine and feces. A skin care regimen was not in place, however, Shannon reported that an ad hoc and inconsistent application of a variety of different skin preparations was likely being applied in the preintervention period.
The RCT by Houwing described the control arm as 30° position change every 6 h for 4 weeks. This study included three arms, a control arm, a placebo arm, and an intervention arm. This study used the control arm as the comparator, which did not include any skin care intervention.
The classification of pressure injury using validated staging/grading methods was varied, with only one study using the European Pressure Ulcer Advisory Panel, 28 one study used the Agency for health care policy and research, 27 another study used the facility quality indicator profile minimum data set. 25 Shannon et al. did not indicate if a classification system was used. 26 Three of the studies used the Braden risk assessment tool. 26 –28 One study by Clever inclusion criteria focused on those over the age of 65 years and their level of mobility. 25
Quality assessment
Results of the ROBINS-1 and Rob-2 quality appraisal tools are presented in Figs. 2 and 3, respectively. Overall risk of bias was low in the nonrandomized studies (Fig. 2), with the randomized study having some concerns of risk of bias (Fig. 3). It was difficult to assess possible bias in several studies due to inadequate reporting. Of particular relevance to the quality appraisal, the RCT by Houwing et al. assessed with Rob-2, demonstrated an unclear risk of bias. 28
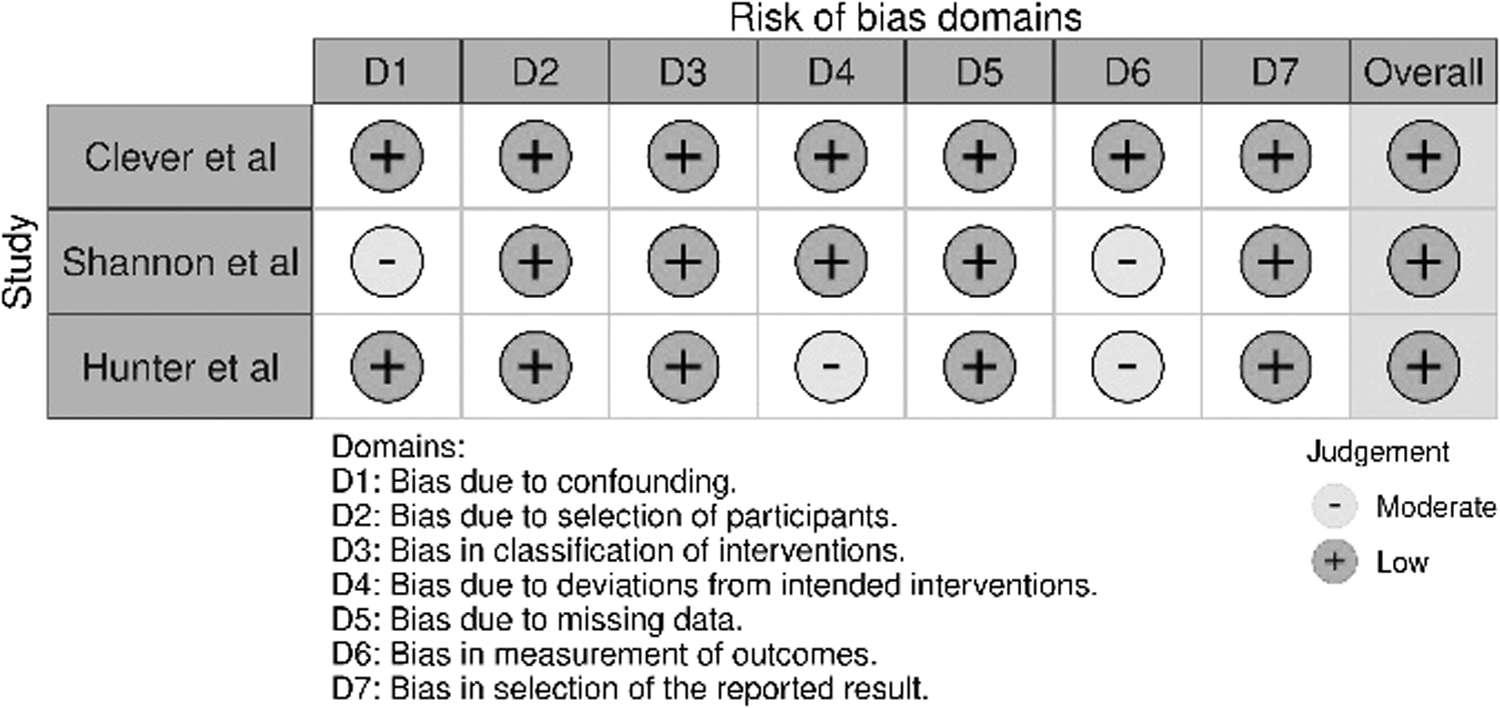
Results from ROBINS-1 Quality Appraisal.

Results from ROB-2 quality appraisal.
This study included three arms: a control group that provided 30° position changes every 6 h over 4 weeks, a placebo group that included the same as the control group, plus a 3-min massage with an indifferent cream and a dimethyl sulfoxide in vaseline–cetomacrogol cream (DMSO-cream) group that included the same as the placebo group. However, instead of the indifferent cream, 5% dimethyl sulfoxide in vaseline–cetomacrogol cream (DMSO-cream) was used. Houwing et al. was not clear on how they generated the random sequence, with the study also being unclear of the method used for concealment. 28
Houwing et al. used topical agents that were blinded to participants; however, it was not clear how blinding of the outcome assessor occurred. 28 The outcome assessor was also blinded to what group the hospital ward was in and it was unclear if the participants knew, which group they were placed in.
Additionally, there was no evidence of publication bias and the funnel plot is included as Supplementary Appendix SA1.
Results from randomized control study
The one included RCT, by Houwing et al., examined pressure injury incidence at the heels and buttocks. They demonstrated that there was no statistically significant difference in pressure injury incidence between the three intervention groups on the buttocks. 28 There was an increase in pressure injury (stage I or II) in one of the intervention groups, the topical 5% DMSO group (moisturizer) for the heel location.
Meta-analysis
Only nonrandomized trials were able to be pooled, due to only one randomized trial being included.
Pressure injury incidence (primary outcome)
Results for the dichotomous variables are presented in Fig. 4 as risk ratios (RRs) with a 95% confidence interval (CI). This RR is the overall ratio of risk of the pressure injuries developed within the studies' experimental group divided by the control groups to compare the two. Three nonrandomized trials evaluating the effectiveness of an emollient, moisturizer, or barrier cream to prevent the incidence of pressure injury were included in the model. In the nonrandomized studies, we used a random-effects model due to considerable heterogeneity (I 2 81%). Findings noted skincare regimens did not significantly reduce the incidence of pressure injury compared with standard care in nonrandomized studies, (relative risk 0.50, 95% CI: 0.15–1.63, Z = 1.15, p = 0.25) (Fig. 4).
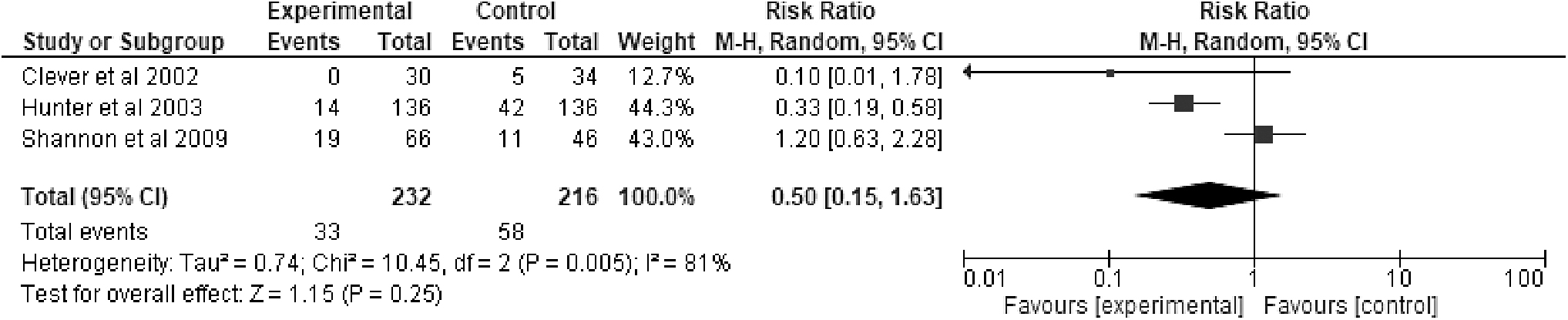
Forest plot of all nonrandomized studies.
DISCUSSION
This research aimed to (1) systematically review the quality of the existing literature on the effect of inert moisturizers, emollients, or barrier preparations on the prevention of pressure injury, and (2) to determine the effect of inert moisturizers, emollients, or barrier preparations compared with standard care on the prevention of pressure injury in aged care or hospital settings. The nonrandomized studies, all demonstrated a low overall risk of bias using the ROBINS-1 tool, therefore, had good overall methodological quality. The meta-analysis of three nonrandomized trials demonstrated that inert moisturizers, emollients, or barrier preparations were not effective in preventing pressure injury (Fig. 4) in aged care or hospital settings.
The RCT also did not demonstrate a significant reduction in pressure injury incidence. 28 One of the included quasi-experimental studies showed a statistically significant reduction in incidence of stage I and II pressure injury in aged care residents. 27 Hunter et al. utilized a lanolin-based skin protectant barrier preparation, while controlling for cleansing of the skin, by using an all-purpose neutral body wash, which aimed to further support moisturize balance of the skin. 27
This supports current guidelines, which advise against using alkaline soaps and cleansers, which are known to strip moisture from the skin 1 by disrupting the acid mantle. 16
Furthermore, it supports the use of a barrier preparation to seal in moisture within the skin to optimize skin integrity 29 to prevent minor (stage II and II) pressure injuries. The study by Clever also utilized a barrier cream, however, did not demonstrate a statistically significant effect. Differences in the findings between the studies may therefore be explained by differences in study methods and other factors. Clever et al. had a much smaller sample size 25 compared with Hunter et al. 27 and only targeted incidence of sacral pressure injury, whereas Hunter et al., 27 included incidence of pressure injuries at the sacrum and heel. It is also unclear what cleansing product was used by participants in the trial by Clever et al., 25 or if this was being controlled for. The other included studies used different topical products with Houwing et al. 28 using a topical cream containing dimethyl sulfoxide, and Shannon et al. using a silicone-based emollient. 26
Other aspects of included studies were notable. The wide CIs around the effect size, indicated high levels of uncertainty (Fig. 4). This supports the need for more adequately powered research into effect for the use of topical moisturizers, emollients, or barrier preparations. The clarity of intervention frequency, skin damage, and grading used for pressure injury staging is an area that could have also been improved in the included studies. This has implications to correctly diagnose the pressure injuries for inclusion in the results. Included studies used a variety of topical products, and no studies indicated the dosage of the application used or the consistency for each participant, which makes comparison to consensus documents difficult. Determining the fidelity of the interventions was also not reported.
While the findings of this study do not demonstrate that the use of moisturizers, emollients, or barrier preparations are effective in preventing pressure injury, the NPUAP guidelines highlight the importance of completing regular skin assessments, which are crucial for early detection of skin damage and potential pressure injury development. 30 Furthermore, as part of risk screening, the NPUAP recommend examining the skin and monitoring it regularly to identify any changes to the skin and if noted, the frequency should be increased. 30
Thus, applying moisturizers, emollients, or barrier preparations allows for closer examination and assessment of the skin on a frequent basis. Topical treatments are also proposed as important because moisturizing the skin allows it to move freely over surfaces, reducing the skin from dragging when moved reducing friction. 31 Therefore, based on the results of this study, clinicians should not change their practice, as there is inadequate good-quality evidence to implement change in this area.
Limitations
While we performed a systematic search of the literature, there may have been omissions that we are unaware of. Our review relates only to inert emollients, creams, or barrier preparations, which meant many studies were excluded which either used oils, gels, or used active ingredients, such as hyperoxygenated fatty acids. These other applications may have use and be effective at preventing pressure injury. However, our review aim was targeted at simple, cost-effective, and available preparations, which aimed to improve skin integrity to reduce incidence of pressure injury and would be easily implementable in hospital or aged care settings. Our criteria relating to what is an emollient, cream, or barrier preparations came from definitions listed in the Prevention and Treatment of Pressure Ulcers/Injuries Clinical Practice Guideline. 2
CONCLUSION
Pressure injuries are common within hospitals and aged care settings, often affecting those over the age of 65 years. It is common practice to apply moisturizers, emollients, or barrier preparations to the skin to prevent pressure injuries in line with guideline recommendations. However, this study demonstrated that based on current available evidence, their use to prevent pressure injury in aged care or hospital settings is not clearly supported. A major caveat to this statement, however, is that due to the limited available data, and the unclear risk of bias and heterogeneity, the results of this study should be considered with caution.
A lack of detail in many of the included studies on the product application protocol, including frequency and volume of product applied, suggests that there is potential that many of the included studies may not adhere to the guidelines for pressure injury prevention. Considering the incidence of the problem, the overall cost of treating pressure injuries, and the effects on quality of life, further well-designed RCTs are justified to determine if this cost-effective option to improve skin integrity can effectively reduce pressure injury.
Studies should consider the number of applications of the emollient, moisturizer, or barrier cream daily, the volume of product applied at each application, the quality of the chosen product, the cost-effectiveness of the chosen product, and the use of the product within a bundle of care focused on improving skin integrity.
TAKE HOME MESSAGES
The use of inert moisturizers, emollients, or barrier preparations does not reduce the incidence of pressure injury in aged care or hospital settings
Combining an inert moisturizer with a pH neutral skin wash is more likely to reduce minor pressure injury (stage I and II)
There is a need for more RCTs to evaluate the use of simple, cost-effective inert skin preparations to prevent pressure injury in aged care and hospital settings
Footnotes
ACKNOWLEDGMENT AND FUNDING SOURCES
The authors thank Nicole Faul-brown, Librarian, University of Newcastle who provided assistance with search strategy. B.M. is a recipient of a National Health and Medical Research Council Investigator grant (GNT2008392).
AUTHORs' CONTRIBUTIONS
H.R.: Methodology, Investigation, Formal Analysis, and Writing—Original draft preparation. P.T.: Methodology, Preparation, Investigation, Formal Analysis, and Writing—Review and Editing. B.M.: Conceptualization, Methodology, Writing—Review and Editing, and Supervision. O.G.: Conceptualization, Writing—Review and Editing, and Supervision. A.H.: Writing—Review and Editing and Supervision.
AUTHOR DISCLOSURE AND GHOSTWRITING
H.R. is a PhD candidate and is receiving an unrestricted scholarship from GAMA health care, who did not have any direct input to this work. H.R. has received honorarium from Molnlycke, 3M, and Smith and Nephew, for education events, however not directly related to this work. P.T. has received a competitive grant from URGO foundation, not related to this current
ABOUT THE AUTHORS
Hayley Ryan, is a registered nurse, current chair of Wounds Australia and a PhD candidate. Dr. Oya Gumuskaya, is a registered nurse and lecturer in the School of Nursing, University of Newcastle. Prof. Brett Mitchell, is a professor in nursing at Avondale University and NHMRC funded investigator (GNT2008382). Dr. Allison Hutton, is a professor in nursing at the University of Newcastle. Dr. Peta Tehan, is a clinical high-risk podiatrist and lecturer in the Master of Wound Care program at Monash University.
Supplementary Material
Supplementary Material S1
Supplementary Appendix SA1
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.