
Abstract
Significance:
Healthy skin provides a barrier to contaminants. Breaches in skin integrity are often encountered in the patient health care journey, owing to intrinsic health issues or to various procedures and medical devices used. The time has come to move clinical practice beyond mere awareness of medical adhesive-related skin injury and toward improved care and outcomes.
Recent Advances:
Methods developed in research settings allow quantitative assessments of skin damage based on the measurement of baseline skin properties. These properties become altered by stress and over time. Assessment methods typically used by the cosmetic industry to compare product performance could offer new possibilities to improve clinical practice by providing better information on the status of patient skin. This review summarizes available skin assessment methods as well as specific patient risks for skin damage.
Critical Issues:
Patients in health care settings may be at risk for skin damage owing to predisposing medical conditions, health status, medications taken, and procedures or devices used in their treatment. Skin injuries come as an additional burden to these medical circumstances and could be prevented. Technology should be leveraged to improve care, help maintain patient skin health, and better characterize functional wound closure.
Future Directions:
Skin testing methods developed to evaluate cosmetic products or assess damage caused by occupational exposure can provide detailed, quantitative information on the integrity of skin. Such methods have the potential to guide prevention and treatment efforts to improve the care of patients suffering from skin integrity issues while in the health care system.

SCOPE AND SIGNIFICANCE
This review on skin assessment methods and patient risk factors for skin damage summarizes the literature on these topics. Our goal is to bridge these areas and explore how some research methods could be used to potentially contribute to an improvement in clinical care by helping to prevent medical adhesive-related skin injury (MARSI) in at-risk patients.
TRANSLATIONAL RELEVANCE
Various skin assessment and risk assessment tools initially developed for research purposes may hold promise to improve care and outcomes for patients with fragile skin. The utility of several methods will remain in research and product development and for the comparison of safety profiles of various devices. Some methods however could be considered to quantitatively assess the condition of a patient's skin before choosing an intervention to prevent skin damage. The suggestions made here will need to be validated to establish clinical relevance and determine the cost–benefit of this approach and its impact on clinical outcomes.
CLINICAL RELEVANCE
Healthy skin serves as a barrier to protect the body from outside contaminants and microorganisms. Preserving and protecting skin health is an important component of quality care for patient satisfaction, and it is also better economically than the treatment of lost skin integrity. 1 Unfortunately, there are many circumstances in health care settings where skin is exposed to various medical devices (tapes, dressings, securement devices, drapes) and/or conditions (friction, pressure) that put it at risk for damage. In addition, as patients age, their skin becomes more fragile, slower to heal, and more susceptible to injury from various trauma and exposure to moisture. 2 –4 Once the skin is damaged, it becomes more susceptible to infection because of reduced immunosurveillance. 5
BACKGROUND
Adequate care often involves balancing the need for adhesion versus minimizing skin damage. The strength of adhesion needed depends on the application: a dressing placed to minimize the risk of pressure ulcer development does not require the same adhesion as a device securing a central venous catheter or a tape securing a nasogastric tube. The problem of MARSI has been recognized for several years. 5 –9 MARSI are skin adverse reactions that can occur in anyone requiring a medical adhesive, and they can be avoided with preventive measures. 5 The true incidence is not known because these occurrences are believed to be underreported. However, several studies in specific settings have been published. We have summarized this information to provide a general idea of the situation; studies are not always comparable however because of differences in reporting (Fig. 1). Table 1 provides the various types of skin damage.
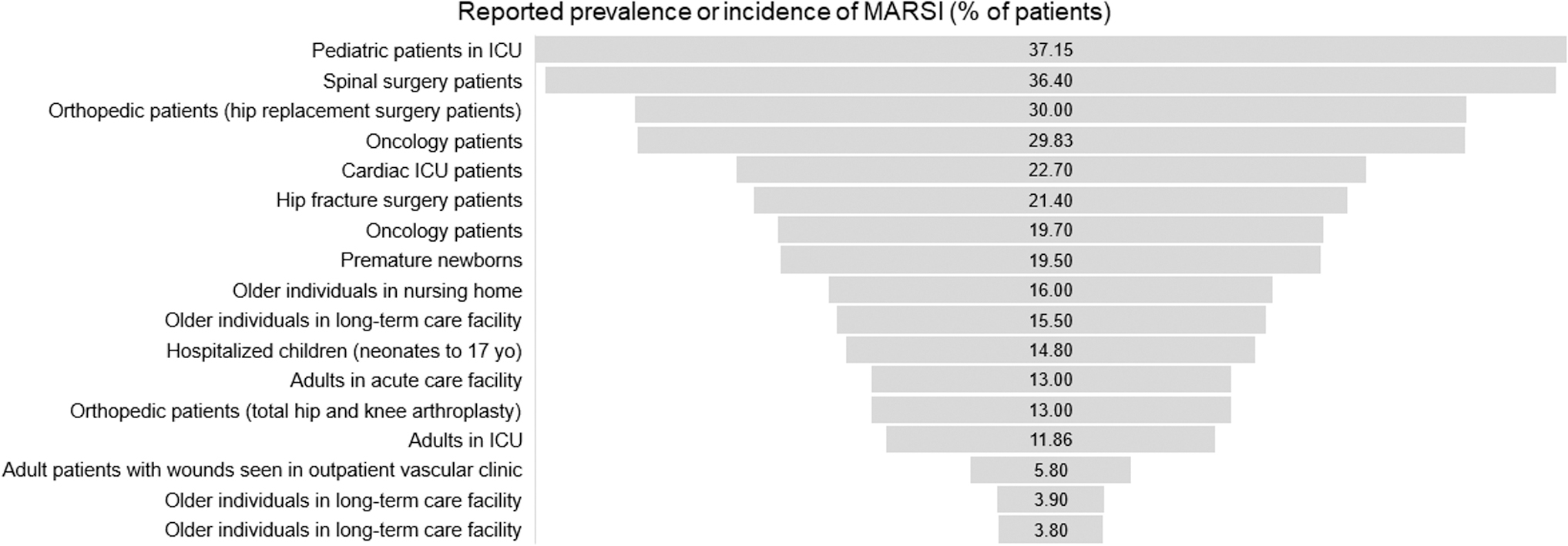
Examples of reported prevalence or incidence of MARSI in the literature, in percent of patients affected. Sources (from top to bottom): Wang et al 10 ; Kim and Shin 11 ; Schwartz Sellaeg et al 12 ; Zhao et al 13 ; Alcantara et al, 14 ; Polatsch et al 15 ; Zhao et al, 16 ; de Oliveira Marcatto et al 17 ; White et al 18 ; Konya et al 19 ; McLane et al 20 ; Farris et al 21 ; Jester et al 22 ; Gao et al 23 ; Ratliff 24 ; Koyano et al 25 ; Sanada et al. 26 MARSI, medical adhesive-related skin injury.
Types of skin damage
Skin can be damaged in various ways. When directly damaged by an adhesive product (dressings, tapes, stoma devices, tube/catheter securement devices, electrodes, etc.), the damage is termed MARSI. Skin damage from other causes makes the skin more susceptible to MARSI.
MARSI, medical adhesive-related skin injury.
With reported incidences as high as 37% of patients affected, the prevention of avoidable skin damage ought to become a higher priority. To improve care and prevent MARSI, it is equally important to provide a good skin care routine, carefully select adhesive products, and utilize appropriate application and removal techniques. Reducing the risk of contamination also plays an important role.
Treatment strategies should aim to preserve or restore the barrier function, allow healing to occur, and prevent recurrence of the injury. Several categories of products are available to help restore the barrier properties of the skin and protect it from environmental assaults. These products comprise moisturizers and skin barriers. Moisturizers are the most prevalent components of skin care products. The main classes of moisturizers are based on their main ingredient properties including occlusive agents, humectants, and emollients. These have been reviewed by Nolan and Marmur. 27
In brief, occlusives form a hydrophobic layer on the skin and provide a barrier to water loss. Petrolatum and dimethicone are the most common examples, and they both can also act as emollients. Humectants are able to increase the water content of the skin by enhancing water absorption from the dermis into the epidermis. Examples include glycerin, hydroxyl acids, propylene glycol, and urea. To prevent excessive water loss from the dermis, humectants are often combined with an occlusive compound. Emollients such as fatty acids improve the appearance and texture of skin by filling in the crevices between corneocytes.
The application of moisturizers increases moisture levels in the stratum corneum. Desmosomal degradation is an important mechanism in the physiological process of skin exfoliation and is essentially controlled by moisture content in the stratum corneum. It is postulated that moisturizers aid the degradation of desmosomes, which are abnormally retained in xerotic skin conditions. 28 With this effect, moisturizers support an orderly and physiological exfoliation of the top skin layer resulting in less flaky skin surface and better cosmetic appearance. Draelos has provided additional information on the properties of moisturizers found in common skin care products. 29
In a different review article, Draelos discusses the various barrier repair products that exist for professional use and the physical change they induce in the skin, namely an increase in skin hydration as measured by transepidermal water loss (TEWL). This review also discusses additional ingredients such as ceramide, palmitoyl ethanolamide, hyaluronic acid, licorice extract, and paraffin wax. These creams do not actually repair the barrier, but rather create an environment optimal for healing. 30
Once the skin has regained its physiological balance, the selection of suitable adhesive medical devices together with an adapted care technique as part of the daily routine is the best prerequisite to providing the patient with the best possible care. Application technique should always follow the manufacturer's instructions and be performed on clean and dry skin, without tension, stretching, gaps, or wrinkles; removal should be “low and slow” (no fast, vertical pulling) and may be aided by the use of medical adhesive removers. 5,31 Proper care techniques include reducing the risk of cross-contamination from products that have been traditionally carried around and reused, such as medical tapes. 32 Single-patient, single-use products are safer with respect to cross-contamination. This is important because if an injury of the skin barrier happens at the same time as contamination in a hospital setting, there is a higher risk of infection. 19
These considerations become increasingly important when treating older patients. As the skin ages, the dermal–epidermal junction flattens, with the rete peg-related roughness index decreasing by >35%. 33 The interdigitation index, an expression of the shape of the border between the epidermis and the dermis, decreases by ∼20% in older subjects compared with a younger cohort. 34 Skin stiffness also decreases with age. 35 These changes make the skin more prone to trauma and shear injuries such as skin tears. Finally, championing skin integrity using a model of education, auditing, and feedback can increase the uptake of evidence-based practice by staff and significantly decrease the proportion of residents with a wound of any type in residential aged care facilities. 36
Methodologies already exist to quantitatively assess skin aging and skin damage. These methods serve as tools to compare products in controlled research settings and provide a better understanding of interactions between adhesives and skin. In addition to current clinical strategies, some of these methods could potentially be used preventatively in at-risk patients to customize their care. Individualized patient risk assessment is another important factor to help prevent MARSI. In this article, we will review the available skin assessment methods and patient risk assessment tools and propose to use some of these methods to help move clinical practice beyond MARSI awareness toward improved care and outcomes.
The literature on this topic sometimes overlaps with the wound healing literature because severe MARSI can cause wounds that are difficult to heal and can become infected. Moreover, MARSI can also occur on the fragile periwound skin around chronic wounds. A full review of wound healing is however out of scope here.
DISCUSSION
Assessment of skin damage
Several methods have been developed in research settings to quantitatively assess skin damage. These methods are based on the measurement of baseline skin properties that change when skin is stressed. The effective barrier properties of healthy skin depend on protein-rich corneocytes surrounded by the lamellar intercellular lipids. When the barrier function is degraded, such as in dry skin, moisture escapes, breaches develop, and the skin becomes susceptible to irritation and damage from external factors. This is given in Fig. 2 and reviewed in detail by Proksch et al. 37
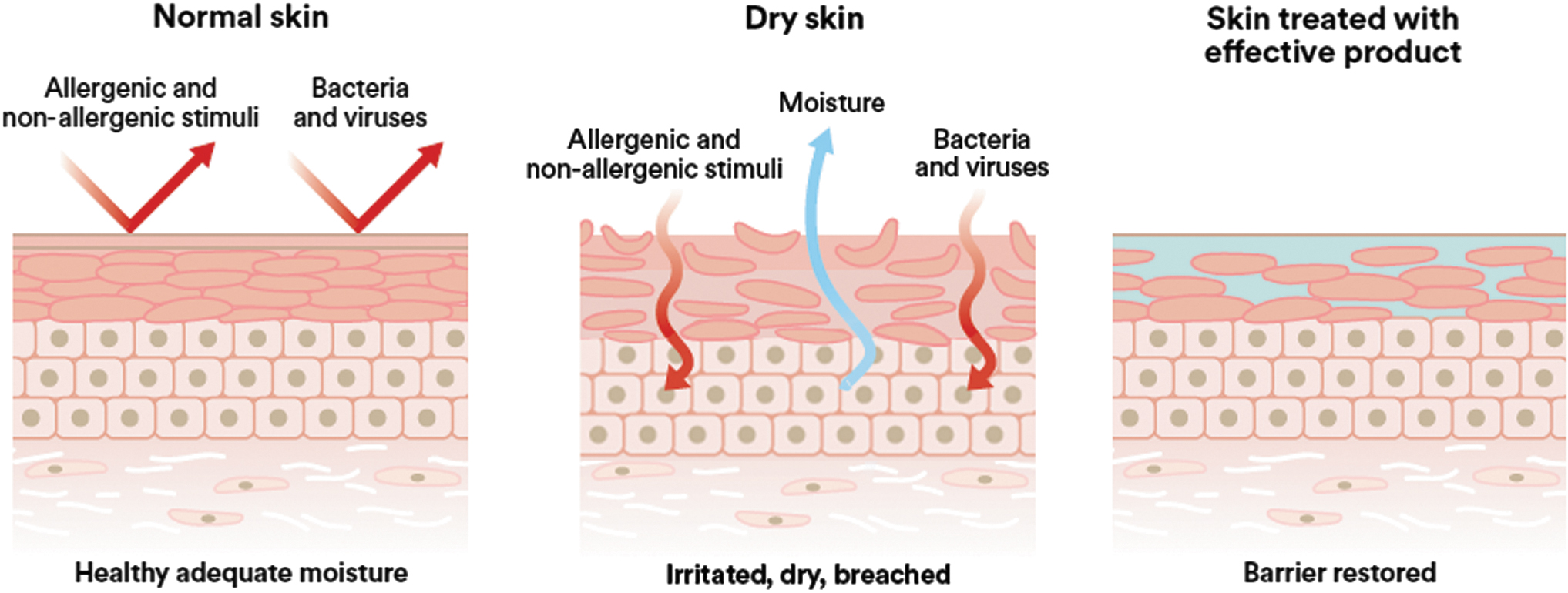
Representation (from left to right) of (a) normal skin; (b) dry skin; and (c) skin treated with effective product.
Therefore, measurable parameters such as skin hydration, TEWL, and irritation, among others, will provide information differentiating damaged skin from healthy skin. The values of these parameters will vary depending on the degree of skin damage. Assessment methods are more commonly used in research settings but could be useful in clinical setting to observe trends, intervene to protect the skin from further damage, and assess whether an intervention leads to improvement. Test methods are described hereunder and summarized in Fig. 3 and Table 2.
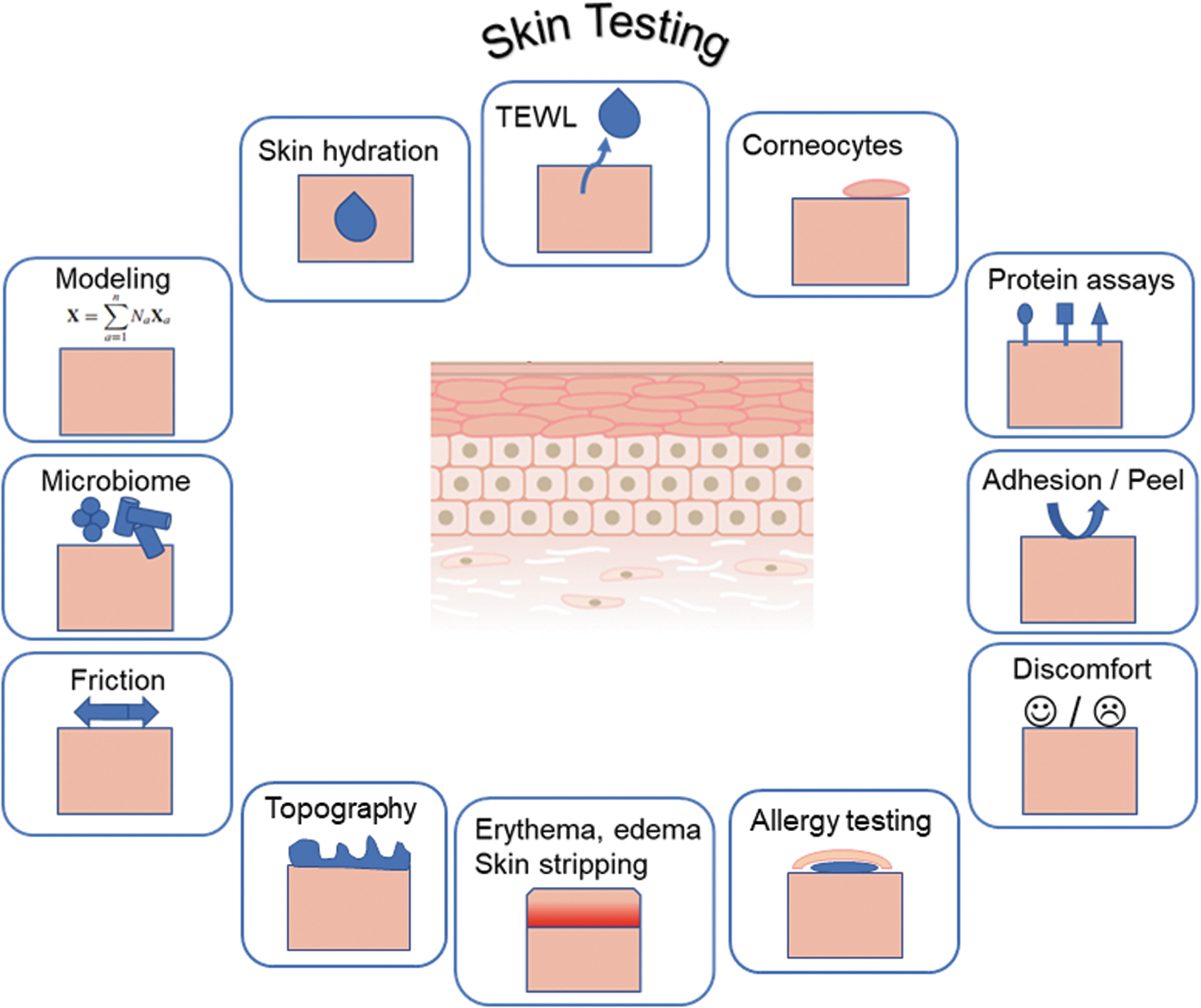
Representation of skin testing methods.
Summary of skin testing methods with examples of references
ELISA, enzyme-linked immunosorbent assay.
Skin hydration
Water is a main component of the skin and plays a key role in the physiological balance of important skin functions, such as barrier effects to external water, chemicals, and allergens. It also affects the biomechanical properties of the skin. The level of skin hydration has been associated with susceptibility to pressure injury and wound chronicity and healing, 38,39 because the condition of the periwound skin is a relevant factor for the progress of wound healing. Dry skin is prevalent in the aged population and is associated with a higher risk of itching, stinging, burning, skin tightness, and skin tears. 40,41 Conversely, excessive hydration, also known as skin maceration, increases the coefficient of friction (CoF) of skin 42 and the risk of skin damage from friction and pressure. 43,44 This, in turn, affects the mechanical properties of the skin. 45 Epidermal hydration can be assessed using electrical, thermal spectroscopic, and microwave methods. 46
Measuring the electrical conductance of the skin provides a measure of hydration. 47 For example, skin maceration (a condition in which corneocytes took up significant amounts of water), is correlated to an increase in the measured electrical conductance. This technique can be used to compare the effectiveness of various barrier creams by measuring the electrical conductance before and after repeated soak cycles. 48 Skin hydration can also be assessed in studies of periwound skin near venous leg ulcers, diabetic ulcers, and pressure-prone areas of the sacrum 49 as predictive information for wound healing potential or pressure injury development; the authors suggested a bimonthly assessment of periwound hydration and erythema to help guide care.
Proksch et al 37 reported that skin hydration can be inversely correlated with TEWL based on experiments involving cleansing the skin with soaps and detergents and on examples of diseased skin. Caberlotto et al 50 also concluded that the higher the skin hydration, the lower the TEWL in an experiment on volunteers treated with model hydrating products containing various concentrations of glycerol as a hydrating ingredient.
The measurement of electrical conductance can be performed easily and quickly with a small portable instrument and could be integrated in a clinical routine for a quantitative assessment of skin hydration.
Transepidermal water loss
The stratum corneum is the main barrier for water evaporating through the epidermis to the external environment. This passive transport is driven by the water vapor pressure gradient inside versus outside the skin and is used to quantify the skin barrier function. This so-called “insensible perspiration,” measured as TEWL, should be differentiated from the “sensible perspiration,” the active water evaporation through sweat gland activity. 51,52
The measurement of TEWL is used to quantify the loss of water and is accepted as a reliable marker for the skin barrier status. TEWL has been determined to range from 120 to 240 g/m2/day. 53 If the skin barrier is damaged, TEWL becomes elevated. International guidelines have been developed for measuring TEWL and skin hydration in nonclinical settings to assess workplace exposure to physical and chemical stressors. 54 Various methodologies have been reviewed. 46,53,55
The technique, also referred to as evaporimetry, requires that specific care be taken to control factors that may influence the real TEWL. This includes reducing sweat gland activity by defining controlled conditions, with temperature under the thermal sweating threshold and after acclimatizing the subjects. In addition, no topical skin care products should be applied for 12 h before the experiment, and the same instrument, contact pressure, and defined anatomical area should be used consistently. Nevertheless, TEWL remains sensitive to confounding factors. 52 Commercially available instruments use either an open chamber method or a closed-chamber method (in which measurements are not influenced by external air convection and turbulence). This is described in detail in du Plessis et al. 54
The TEWL measurement has been used in research settings for multiple applications. It can be used to examine the effect of the repetitive application and removal of various medical tapes and adhesive devices on skin integrity for the purpose of comparing adhesive product gentleness. 56,57 It can also be used to observe the effect of barrier films on skin integrity (a clinical study on premature infants used this method to choose the best skin barrier product) 58 to measure excess water in overhydrated skin (such as macerated skin), 59 or to evaluate the clinical severity of disease in patients affected by atopic dermatitis or psoriasis in comparison with healthy skin. 60,61
Research using animal models has shown that chronic wounds infected with biofilms may later heal and visually appear to be closed, but the skin barrier function may be compromised as demonstrated with TEWL measurements. 62 This could explain further complications and provide an example where functional measures of skin barrier function may provide useful information. Further animal studies using weak electric fields to combat wound biofilm infection showed that the acceleration of wound closure occurred by restoring skin barrier function. 63
It is now understood that wound closure without a restored barrier function is not sufficient because it leaves the site prone to wound recurrence. As a consequence, the concept of functional wound closure has emerged, 64 and the measurement of barrier function restoration is important to characterize complete wound closure. The measurement of TEWL can be performed easily and quickly with a small portable instrument and could be integrated in a clinical routine for a quantitative assessment of the skin barrier function.
Corneocytes
The stratum corneum is the main anatomical structure to maintain a barrier between the organism and the external environment. Accordingly, it must withstand enormous mechanical forces and yet display the elastic properties important for its general biological function. Corneocytes are vital elements of the stratum corneum architecture. They are differentiated apoptotic keratinocytes, composed of a cornified envelope filled with keratin proteins. They are connected to each other by desmosomes to withstand various types of mechanical stresses. Desquamation of corneocytes is a well-controlled complex mechanism that allows continuous renewal of the outmost barrier.
Given their position at the outermost layer of the skin, corneocytes are the first layer to lift off from adhesive device removal, and their measurement can be used to assess how much skin is stripped by tapes or other adhesive devices. The technique involves applying tape to the skin, removing it, and staining the cells present on the tape to quantify them. The term “tape stripping” is often used to describe this form of controlled “skin stripping” (a clinical term used to describe skin damage from adhesive device removal).
A study by Tokumura et al 56 showed that as pressure-sensitive adhesive tapes were applied repetitively, the dermal peeling force gradually increased, the amount of stripped corneocytes decreased, and the skin irritation worsened. The method allowed differentiation of tapes by strength of adhesion and showed seasonal variability. Of interest, the area ratio of stripped corneocytes was highly correlated with TEWL, which directly reflected the degree of skin irritation. The method can then be used to test various formulations of adhesives and to develop tapes with improved performance. 56 Several studies have also included an assessment of pain/discomfort upon removal of tapes or adhesive dressings 65 –69 with a general association between discomfort and the product's adhesion or peel force. With newer silicone adhesives, however, good adhesion can be obtained without causing much skin damage upon removal. 70
In a different variation on the method, Waring et al 71 applied a stain to the skin before repeated application and removal of different adhesives and measured the intensity of the stain left after each application using a chromameter. They compared this method with TEWL and found the staining methodology as effective in detecting and comparing adhesive damage, and possibly able to detect barrier disruption earlier than the TEWL method. The consistency of the method used and the importance of defining the experimental conditions are critical to establish valid comparisons between adhesive products. Breternitz et al 72 have shown that the degree of skin barrier disruption depends on the total duration of applied pressure, the anatomical site, and the condition of the skin before stripping (occlusion versus non occlusion).
This type of measurement involves stripping the skin and is appropriate for research studies in healthy volunteers. We do not consider this method to be appropriate for patients with fragile skin.
Total protein assays
This test targets the same information as the corneocytes test (evaluation of the extent of skin stripping caused by the removal of an adhesive device) but measures the amount of protein in the stratum corneum removed. The first step is the same as above (applying tape to the skin and removing it); the second step can use different methods to analyze the protein collected on the tape. Various assays are available to estimate total protein, including both soluble and insoluble proteins or only the soluble protein. Other analytical techniques can also be used to specifically look at inflammatory markers, lipids, and so on. These methods have been described by Clausen et al. 60
This approach is useful not only to compare damage from different adhesive products but also to look at differences in stratum corneum between healthy skin and skin affected by pathological conditions such as atopic dermatitis. Gentler sampling methods have also been described. Portugal-Cohen and Kohen 73 described a skin surface wash with an extraction buffer in a well adhered to the skin, followed by enzyme-linked immunosorbent assays for cytokine quantification. This method allowed them to demonstrate distinct patterns of cytokine secretion related to psoriasis and atopic dermatitis. The approach of measuring inflammatory cytokines could also be used to gauge the level of irritation caused by various devices after their removal from skin.
Skin blotting using a nitrocellulose membrane to attract and absorb skin proteins is another method to analyze soluble factors secreted and distributed in the dermis and epidermis. 74 The method has been used to measure levels of type IV collagen, matrix metalloprotease 2 (MMP-2), and tumor necrosis factor alpha (TNF-α) in patients with skin tears compared with those without them. 25 This approach (using a noninvasive skin surface wash) could possibly predict a patient's risk of experiencing skin tears, but requires more elaborate laboratory equipment not practical in a clinical setting.
Adhesion, peel force, and discomfort
Adhesion to skin is an important property, as it affects the performance and wear time of medical devices. As mentioned earlier, adequate care often involves balancing the need for adhesion versus minimizing skin damage from device removal. Adhesion to skin can be quite variable because many factors affect it, such as variability between subjects, anatomical location, hair density, age, health status, sebum production, ambient temperature, and humidity. For this reason, methods have been developed in an attempt to find a more reproducible substrate (artificial skin, various plastics, steel). Additional parameters that can be standardized include exact sample size, dwell time, peel angle, and peel speed.
Standardization improves reproducibility and allows generation of comparative data on adhesion strength of various products tested in terms of peel force needed to remove a sample (reflecting adhesion performance). However, testing on human subjects is the only way to truly assess clinical performance including the interindividual variability of adhesion and to gather information on the perception of pain and discomfort (through subjective assessment) and possible allergic reactions to the material tested.
Standard methods (utilizing standardized substrates such as steel) exist to test adhesion of pressure-sensitive tapes from the American Society for Testing and Materials (ASTM), 75 the International Standards Organization (ISO), 76 and the Pressure Sensitive Tape Council (PSTC). 77,78 In addition, several publications (using standard methods or variations thereof) are available reporting human volunteer studies in which various medical devices were adhered to skin and peel force was measured along with assessments of skin damage and self-reported discomfort. 56,65,68,79 Some studies also compared peel force results between human skin and substrates intended to mimic it better than steel to develop a more consistent assay. 69,80
Peel force methods are typically used to compare the adhesion strength of various products. They can easily be combined with corneocyte or total protein assays on the same samples to provide additional information (see previous paragraphs describing those methods). 57,81 They can also be used to compare the adhesion under different moisture conditions. 82 Another use for these methods may be to see the effect on adhesion of other products often used simultaneously with adhesive devices, such as skin cleansers, antibacterial skin preps, barrier films, and skin protectants. 83,84 It is important to know if these products affect the performance of tapes, dressings, or other adhesive medical devices such as securement devices, incise drapes, and so on. For example, petrolatum-based products reduce the adherence of wound dressings but most film-forming polymers do not. 85
Finally, a specific application in which adhesion is critically important is for transdermal drug delivery patches, where adhesion characteristics must be designed to provide complete and consistent adhesion over the entire application period to ensure proper drug delivery. 86
This method belongs in research settings, as it could cause skin damage to patients with fragile skin.
Erythema, edema, denudation, and skin stripping
These clinical observations are typically recorded using semiquantitative scales and can also be documented using photography. They can all have in common a color change of the affected skin. The change can be transient if the redness is owing to a physiological response rather than damage (vascular reflex with increased capillary flow); therefore, a protocol specifying the time point(s) of observation after device removal is helpful. Erythema owing to device removal is considered MARSI if the redness persists 30 min or more after the removal of the adhesive. 7
This type of observation is not always as quantitative as the other assays described but it provides a pragmatic, real-life clinical assessment. It can be used to document clinical observations related to various skin conditions, or to document additional diagnostic data from experiments using tape stripping to compare the gentleness of various adhesive products, as described previously in the section Corneocytes. Grove et al 57 have proposed detailed severity scales for erythema/edema and denudation/skin stripping visual assessments in a study comparing tapes for their gentleness. Studies evaluating postoperative scar cosmesis have also proposed semiquantitative scales to grade skin redness. 87 It is important to note that variations in skin tones from different ethnicities greatly influence any assessments relying on colors and color intensity, limiting the reproducibility and reliability of this assessment.
Additional quantitative evaluations of redness have been proposed using various instruments: the DiaStron erythema meter, 88 the Chromameter CR 300, 89 or the ScarletRed®Vision digital skin imaging mobile application. 90 The latter method introduces the Standardized Erythema Value and overcomes the usual pitfall of spectrophotometric skin analysis by enabling objective quantification and providing a linear scale from bright to very dark skin tones. 91 It can therefore be used independently of skin type, taking into account the basic or even changing skin color of a subject. It is the first objective erythema parameter, providing a linear scale from light to very dark skin tones. 90
The presence of visible redness (assessed qualitatively or quantitatively) should be interpreted as an indication that the skin is fragile and at risk for MARSI. For example, Demarre et al 92 showed that hospitalized patients with nonblanchable erythema were at an increased risk for developing pressure ulcers despite preventive measures.
Skin surface topography
The surface of the skin contains furrows of different depths on its surface, creating a topography that changes with the degree of hydration, the age of the skin, the presence of various skin injuries or diseases, and the application of skin care products. Examining this topography can be carried out in a noninvasive way by active image triangulation 93 and provides useful information on the health and condition of the skin and the effects of various treatments. This technique has been used to observe the effects of tape stripping on the skin surface; repetitive tape stripping was found to destroy skin surface topography by deepening skin furrows, which directly reflected the degree of skin irritation experienced. 56
Other noncontact optical methods have been described as well: the surface evaluation of living skin (using the Visioscan® device) and the phaseshift rapid in vivo measurement of skin (PRIMOS device) were compared, and both were found adequate to demonstrate differences between subjects and treatments. 94,95
The cosmetic industry is particularly interested in this type of measurement to substantiate claims for products intended to correct wrinkles and pigmentation. 96 Several commercially available systems that measure biomechanical parameters such as skin softness, stiffness, firmness, elasticity are described in detail in a recent publication from the European Group on Efficacy Measurement and Evaluation of Cosmetics and Other Products (EEMCO Group). 97 More recently, topological data analysis using skin images has been successfully used in combination with machine learning to quantify the regularity of skin surfaces and predict TEWL, a method that is much faster than directly measuring TEWL. 98
Skin thickness can be measured using an ultrasound scanner. 99,100 This technique has proved useful to study chronological (intrinsic) aging and photoaging (extrinsic aging) of the skin. Dermal and epidermal thicknesses decrease with increasing age in the extremities.
This method requires elaborate instrumentation and we do not foresee a clinical application in the near future.
Coefficient of friction
The CoF measures the amount of resistance that a surface exerts on materials moving over it, for example, a patient's skin against bed linen. It is known that moist skin has a higher CoF than dry skin, 42,101 making it more susceptible to friction blisters. 102 Skin hydration therefore influences the CoF. The literature on pressure ulcer prevention describes well the role of shear and friction in the development of those wounds. 103 Instruments used to measure friction involve a sled moving over a horizontal platform at a constant speed. The CoF is generally defined as a constant μ in the equation F = μW, where F is the frictional force and W is the load applied to the materials. 104 For example, CoF can be measured between two fabrics, between a fabric and a dressing or between skin and any other material of choice.
The static CoF is calculated with the friction force required to initiate the movement between the surfaces at a certain normal load, whereas the dynamic CoF is calculated with the friction force needed to retain the movement once initiated. Both are strongly correlated. 105 Such studies can help indicate which fabrics have lower friction for improved performance and are therefore better suited to preventing pressure sores. 106,107
This method is intended to compare materials and does not apply in clinical settings.
Skin microbiome
Up to 100 trillion microorganisms settle on and in our bodies. Called the microbiome, they form a unique and complex cosmos in the various regions of the body. The skin microbiome includes a specific composition of bacteria, fungi, viruses, protozoa, and mites. 108 The high number of bacteria makes colonization by other potentially pathogenic microorganisms difficult. The microbiome is therefore also a fundamental part of our immune system that is continuously stimulated and trained by our own skin flora and can thus ward off external attacks more efficiently. These microorganisms can be classified as transient versus resident, beneficial versus pathogenic, and collaborators versus adversaries.
Resident microbes are not harmful and may provide benefits; however, after perturbation or injury, they can proliferate and become opportunistic pathogens. Chronic wounds are an example where normal skin organisms can become pathogenic after breaching the skin barrier. 109 The skin microbiome varies between body sites (sebaceous, moist, dry) and between individuals, as it is influenced by ethnicity, environment, and diet. 110,111 In normal conditions, skin microbes contribute to the skin's innate defense by producing antimicrobial peptides. 109
The molecular methods now available, based on the sequencing of the bacterial 16S rRNA gene, have revealed that the healthy skin flora is more diverse than previously recognized using culture methods. 112 The methodology includes the sampling method chosen (swab, biopsy, surface scrape, cup scrub, or tape strip, with the premoistened swab as the most established collection method), the use of controls, sample handling and storage, sample processing, and analysis methods. The research standards and important factors to consider are presented in detail by Kong et al. 111
It is important to realize that although molecular methods allow for the detection of organisms that could otherwise go undetected because they are difficult to grow in culture, the methodology does not distinguish between viable and dead organisms. Culture of viable organisms is still necessary for purposes of antibiotic susceptibility and virulence testing. In a study comparing molecular and culture methods using two different collection techniques (swabbing and tape stripping), the collection techniques showed comparable results for microbiome analysis, and the tape-stripping method collected more viable bacteria than the swabbing method, in numbers of colonies and in number of species detected. 113 This could be explained by the tape-stripping method reaching bacteria deeper inside the stratum corneum compared with a surface swab.
The study of wound microbiomes has also been conducted with conventional cultures and molecular methods. 114,115 The determination of the microbial profile of chronic wounds using molecular methods (DNA sequencing) is currently available to clinicians to guide treatment. 116 Given the expertise and equipment required for this, the use of an outside laboratory is likely to remain a necessity. Studies have shown that molecular pathogen diagnostics that allow for a comprehensive evaluation of the chronic wound microbial bioburden can lead to a targeted therapeutic approach and improve healing rates. 117,118 Biofilm-based wound care has also been shown to lower costs. 119
Biomechanical modeling using finite element analysis
Finite element models allow the development of mathematical solutions to the complex and nonhomogeneous tissue deformation (strains) and stress distributions caused by external loading. The method consists in breaking down large and complex problems into smaller parts termed finite elements. The elements are represented by equations used to solve for unknown values in the model. Tape removal models using finite element analysis have been developed to better understand how medical tape removal affects skin using FEBio, an open-source framework, or Abaqus. 120 The results showed that a silicone adhesive surgical tape had a higher peel force than acrylate adhesive tapes and yet the silicone tape applied a lower skin strain. 121 As such, the use of adhesive products that impart lower stresses and strains upon removal may be an important option for reducing skin injury.
Modeling methods are useful for product development and are not anticipated to provide direct help in clinical settings.
Allergy testing
Adverse skin reactions can occasionally be owing to an allergy. Substances like fragrances, 122 lanolin 122 (used in some moisturizers), latex, 123 wound dressings, 124 acrylates 125,126 (used in several medical adhesives), chlorhexidine gluconate 127 (used for skin prep), and pharmacologic agents 128 are known allergens that can trigger a skin reaction in some patients. Repeated exposure (occupational, or through the long-term use of some products) can cause sensitization leading to the development of an allergy. The way to differentiate between irritant contact dermatitis (nonimmunologic skin damage) and allergic contact dermatitis (a cell-mediated immunologic skin response) is by doing patch testing, a method consisting in exposing the skin of the patient to a small amount of suspected allergen(s) under an occlusive patch and observing the skin reaction at different time points. 129
A complicating factor is that medical device manufacturers are currently not required to disclose a complete list of ingredients for each device, which makes the screening of allowable devices for patients with known allergies very difficult and impedes patient care. Advocacy work is currently underway to change this. 130
This type of testing should be considered in patients with a history of skin reaction to various products to avoid using materials that are allergenic to them.
The literature reviewed emphasizes that a single parameter is not entirely sufficient to describe the skin barrier and therefore a variety of methods should be used. 46 This is also supported by a recent publication aimed to identify a set of robust parameters sensitive to mechanical and chemical challenges to skin integrity: Jayabal et al 137 attempted to use quantitative skin assessment methods to aid the early detection of skin damage for potential clinical application. They found that thresholds derived from single biophysical parameters were limited in detecting skin changes following insults. An evaluation using combined parameters may provide a more sensitive assessment.
In their study, TEWL showed less variability in skin response between subjects than subepidermal moisture, laser Doppler imaging, and erythema. The authors concluded that further research is needed to identify robust biophysical parameters to facilitate early detection of skin damage in clinical settings. The literature also highlights some similarities and overlap between methods; for example, the assessment of corneocytes removed can be performed by looking at the substrate used to remove them or by the resulting appearance of the skin surface, and this assessment will also correlate with the TEWL because it is directly affected by the integrity of the stratum corneum.
Assessment of individual patient risk
The clinical implementation of skin testing methodology should be performed thoughtfully to test when appropriate and ensure that the benefits outweigh the risks and costs. The first element to consider is the individual patient's potential risk to develop skin damage. There is a general awareness that patients who are at the extremes of age, bedridden, or malnourished are at higher risk of skin injury owing to their frail condition. The adverse effects of age-related and disease-related pathologies on skin integrity have been described in the literature. 138 Incidence studies have also been performed to identify risk factors.
Skin tears, for example, have been the topic of a large number of publications and were found to be most prevalent in the elderly people, followed by patients with impaired mobility, patients experiencing falls and accidental injuries, and those with a history of previous skin tears, cognitive impairment/dementia, and dependence in transfers. 3 Incontinence, 139 the presence of an ostomy 140 or a tracheostomy, 141 obesity, 142 malnutrition, 143,144 and various drug reactions 128 are other circumstances that affect the skin barrier and may increase a patient's risk to develop skin injuries. Finally, a history of contact dermatitis and longer time to ambulation after surgery are also factors affecting the risk for MARSI. 11
Several clinical tools have been developed to predict risk of skin injury; two examples are described. The Braden scale was developed and validated to help early identification of patients at risk for the development of pressure ulcers and reflects sensory perception, skin moisture, activity, mobility, friction and shear, and nutritional status. It has been translated in a variety of languages and is recognized internationally. 145,146 The Cubbin–Jackson scale 147 has a similar purpose and was developed specifically for critical care patients. Both scales are considered suboptimal owing to poor specificity and predictive value. 148 This type of risk assessment is used to decide which level of nursing interventions should be implemented to prevent pressure ulcers.
These scales incorporate several factors defining the skin's environment and the overall health of the patient, but no specific instrumental and reproducible skin measurements are included. They are susceptible to assessor bias and may lead to variable scoring results, dependent on the level of clinical expertise and knowledge of the caregiver. Figure 4 provides the types of factors included in clinical assessments. For this reason, measuring skin integrity using quantitative methods such as skin hydration and TEWL, and including allergy testing in patients with a history of dermatitis, could potentially provide more objective information on actual risk and help develop effective care protocols to restore the skin's barrier function to prevent further skin injuries.
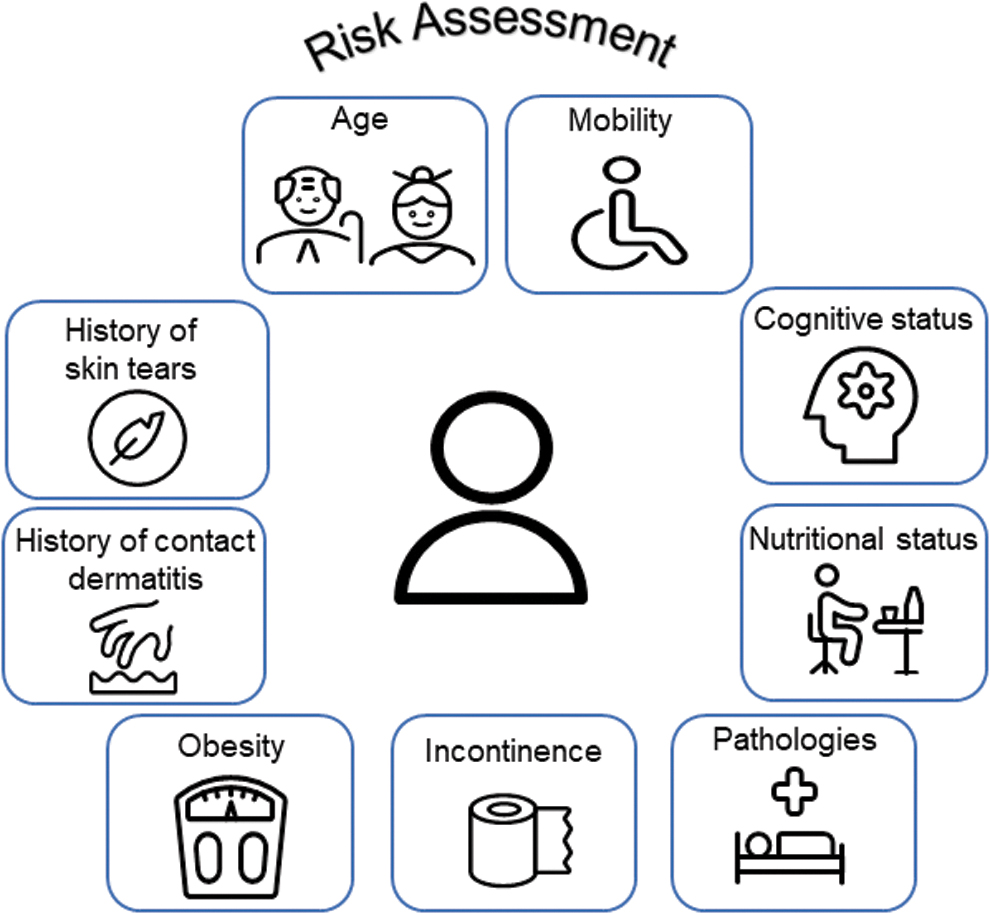
Clinical risk factors assessed to predict skin injury.
Improving care
The body of literature now available describing various quantitative skin assessment methods suggests that some objective skin diagnostic measures developed for research purposes may also be used in clinical practice. These methods are already in use for purposes of cosmetic product testing and evaluation of occupational exposure. Others have already proposed using quantitative assessment tools to predict the risk of skin injury. For example, a Japanese incidence study on skin tears, which also found preexisting skin tears to be a risk factor, additionally looked at the Braden score for the same patients and found that a decrease of 6 points in the Braden score was significantly associated with the development of skin tears. 26
It makes sense that a tool designed to assess overall skin fragility could provide useful information on risk for various types of mechanically related injuries. The same group (Koyano et al) published other studies 25,149 using quantitative skin assessment methods to correlate skin properties and their relationship to skin tears. Their results showed that the dermal thickness (measured using an ultrasound scanner) could identify patients at high risk for skin tears, with a cutoff point of 0.80 mm, 149 and that the expression levels of some skin proteins were significantly different in patients with skin tears, 25 that is, lower levels of type IV collagen and MMP-2, and higher level of TNF-α.
These studies provide specific examples of noninvasive, quantitative, objective skin measurements that may serve as an early predictor of increased risk of skin injury for individually optimized treatment in clinical settings.
Our focus in this article is to consider applications related to patients in health care settings. Based on our experience developing technologies to improve and repair the barrier function of the skin, we recommend the skin hydration (electrical conductance) and TEWL as being the most relevant and easiest to implement clinically for the assessment of skin integrity in patients with risk factors for MARSI. We propose a decision chart (Fig. 5) to incorporate these tests (and potentially a few others as suggested by the literature review mentioned previously) in the clinical setting.
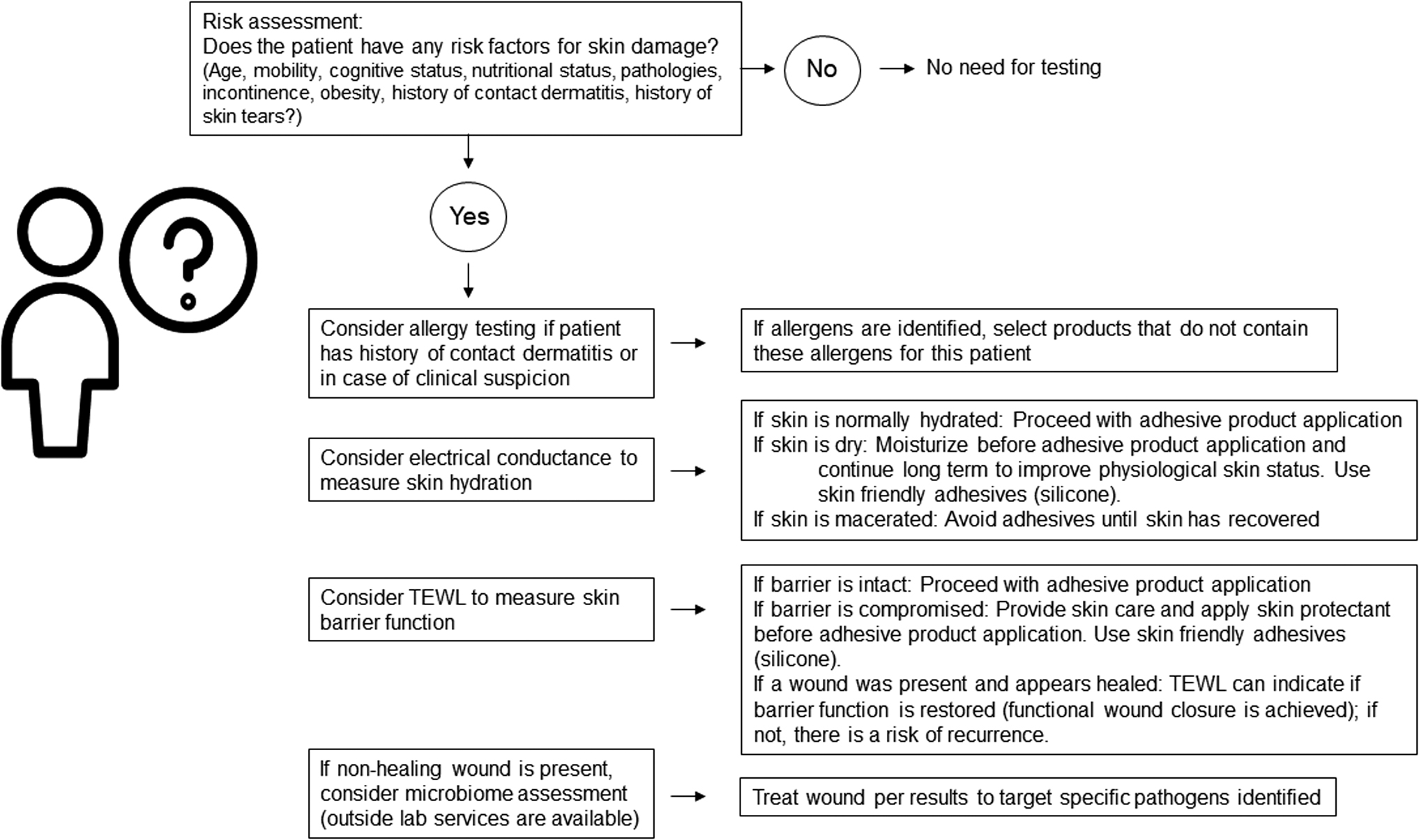
Proposed clinical evaluation algorithm incorporating quantitative test methods as appropriate.
Further studies are necessary to examine the benefits of these assessments to clinical practice. Such methods are likely to highlight larger differences between susceptible patients than between healthy individuals typically tested in research settings. Noting that variability between test methods and between subjects in the response to various insults is significant, it is likely that clinical measurements should focus on relative values instead of absolute, one-time measurements. Monitoring over time will likely be the best way to assess the evolution of a condition and the effectiveness of an intervention.
Another condition increasing risk for skin injury is the presence of a chronic wound. In a way, the skin is already injured because a wound is present, but the health of the periwound skin is important to promote healing and avoid further enlargement of the wound. From that perspective, periwound skin is at risk for further injury and for MARSI because it is exposed to chronic wound fluid and adhesive products from dressings used on the wound. A best practice recommendation for the prevention and management of periwound skin complications was recently published. 150 The evaluation of the wound microbiome should also be considered, as discussed previously.
SUMMARY
A multitude of skin testing methods are available and widely used in research settings to evaluate skin for its degree of hydration, its physiological integrity and topography, its barrier properties, its inflammatory status, its microbiome composition, and its interactions with various materials (adhesion, friction, stress distribution). These methods offer the potential to provide information that may also be useful in clinical settings to help prevent or mitigate skin injury in patients at risk. Current clinical tools for risk assessment focus on the skin's environment and the overall health of the patient, but typically, no specific, reproducible skin measurements are included.
Quantitative measurements could potentially guide clinical practice by providing more objective information on actual risk, documenting the effectiveness of preventive interventions, and helping to develop effective care protocols. In addition, such methods could also be used for better characterization of wound healing, confirming functional wound closure with restoration of skin barrier function. As mentioned previously, the suggestions made here will need to be validated to establish clinical relevance and determine the cost–benefit of this approach and its impact on clinical outcomes.
In addition to addressing skin health, optimal product selection and the use of proper care techniques for product application and removal are paramount to provide the best care for patients.
TAKE-HOME MESSAGES
The time has come to move clinical practice beyond mere awareness of MARSI and toward improved care and outcomes.
Skin assessment methods typically used in research to compare products may offer new possibilities to improve clinical practice by providing better information on the status of patient skin.
Risk assessment tools developed to choose the level of nursing interventions to prevent pressure ulcers could be complemented by quantitative skin measurements, holding promise to improve care and outcomes for patients with fragile skin.
Validation will be needed to establish clinical relevance and determine the cost–benefit of this approach and its impact on clinical outcomes
Footnotes
ACKNOWLEDGMENT AND FUNDING SOURCES
The authors thank Judith Alexander, Technical Information Specialist from 3M Knowledge Discovery and Analytics, for conducting the literature search. The preparation of this publication was funded by 3M.
AUTHOR DISCLOSURE AND GHOSTWRITING
S.F.B. and J.B. are employees of 3M. Both authors contributed to writing this article and no ghostwriters were used to write this article.
ABOUT THE AUTHORS