
Abstract
Objective:
Traditional negative pressure wound therapy (tNPWT) systems can be large and cumbersome, limiting patient mobility and adversely affecting quality of life. PICO™, a no canister single-use system, offers a lightweight, portable alternative to tNPWT, with improved clinical performance. The aim of this study was to determine the potential mechanism(s) of action of single-use NPWT (sNPWT) versus tNPWT.
Approach:
sNPWT and tNPWT were applied to an in vivo porcine excisional wound model, following product use guidelines. Macroscopic, histological, and biochemical analyses were performed at defined healing time points to assess multiple aspects of the healing response.
Results:
Wounds treated with single-use negative pressure displayed greater wound closure and increased reepithelialization versus those treated with traditional negative pressure. The resulting granulation tissue was more advanced with fewer neutrophils, reduced inflammatory markers, more mature collagen, and no wound filler-associated foreign body reactions. Of note, single-use negative pressure therapy failed to induce wound edge epithelial hyperproliferation, while traditional negative pressure therapy compromised periwound skin, which remained inflamed with high transepidermal water loss; features not observed following single-use treatment.
Innovation:
Single-use negative pressure was identified to improve multiple aspects of healing versus traditional negative pressure treatment.
Conclusion:
This study provides important new insight into the differing mode of action of single-use versus traditional negative pressure and may go some way to explaining the improved clinical outcomes observed with single-use negative pressure therapy.

Introduction
Our skin has evolved an innate ability to rapidly and efficiently repair injury and damage. This wound healing response is both complex and dynamic, requiring initial inflammation followed by granulation tissue formation, angiogenesis, reepithelialization and dermal remodelling. 1 In the elderly and diabetic these normal reparative processes are substantially impaired, increasing the risk of developing non-healing, “chronic” skin wounds. 2 Chronic wounds are a significant socioeconomic and clinical burden, estimated to cost the United Kingdom's National Health Service more than £5 billion per year. 3 The development and clinical implementation of therapies designed to address this everincreasing and largely underappreciated area of clinical need remain a challenge. 4,5
Negative pressure wound therapy (NPWT) is one of the most effective and widely used interventions for problematic wounds. 6 In traditional application, foam or gauze is used to fill the wound to allow negative pressure transmission through to the wound bed. A drape is then applied to form a sealed system. NPWT devices generate negative pressure between −50 and −175 mmHg, 7 removing excess wound exudate through a drainage tube and preventing bacterial contamination. 8,9 Early studies demonstrated that traditional NPWT (tNPWT) promotes granulation tissue formation in pigs 10 and in the clinical setting. 11,12 Additional healing promoting effects of NPWT also include pulling wound margins together to accelerate contraction, stimulating cellular proliferation by microdeformation, 13,14 and increasing tissue perfusion. 15 Thus, NPWT is indicated for a plethora of wound types, including acute surgical, chronic, trauma, burns, and skin grafts. 7
Despite its versatility, tNPWT is not without limitations. 16 For example, tNPWT devices can be seen as cumbersome, requiring large canisters, power supplies, and drainage tubes. The utilization of wound fillers (e.g., foam) adds complexity of use, creates longer application times, and can cause discomfort and pain upon dressing changes. Indeed, it has been noted that there is potential for filler fragments to remain in the wound bed. 17 Recently, lightweight negative pressure modalities have been developed to overcome some of these challenges inherent to larger tNPWT devices. One such example is a single-use NPWT (sNPWT) system (PICO™; Smith and Nephew Wound Management, Hull, United Kingdom), which is canister free, portable, and disposable.
In this study, we present a direct comparison of sNPWT to tNPWT in an in vivo porcine injury model, with a focus on elucidating the effects of sNPWT on specific aspects of the wound repair response.
Clinical Problem Addressed
tNPWT has been shown to influence multiple aspects of the wound repair process, but comes with clinical limitations. sNPWT has been developed to overcome these limitations, but the mode of action remains poorly understood. In this study, a standardized and reproducible in vivo porcine wound model is used to explore the effects of sNPWT on specific aspects of the healing response, with direct comparison to tNPWT. This porcine study, in a close model of human wound repair, provides a significant new insight into the effects of sNPWT on healing and should inform future treatment innovations.
Materials and Methods
Animal experimentation
Young (12–14 weeks) female Landrace × Large White × Duroc farm pigs (n = 12, ∼40 kg) were prepared for surgery by intramuscular injection of Azaperone (2 mg/kg) and Midazolam (0.3 mg/kg) and anesthetized with isoflurane and oxygen. Prophylactic amoxicillin (15 mg/kg) was administered subcutaneously on the day of wounding, and buprenorphine (0.01 mg/kg) was given intramuscularly postoperatively and subsequently according to clinical need. Back and flank skin were clipped, wet shaved, and disinfected with 5% chlorhexidine, and the skin wound site swabbed with 70% ethanol immediately before the creation of full-thickness, 3-cm-diameter excisional wounds (two wounds per flank on each pig). Digital photographs were then taken for macroscopic wound analysis.
Contralateral wounds were treated with sNPWT (PICO system with no filler; Smith and Nephew Wound Management, Hull, United Kingdom; −80 mmHg) or tNPWT (V.A.C Via™ system with Granufoam™ wound filler; KCI Medical Ltd., West Sussex, United Kingdom; −125 mmHg continuous mode). The PICO sNPWT system consists of a silicone wound interface dressing to transmit even pressure across the wound bed, while negative pressure in the traditional device was transmitted from the wound filler. sNPWT was changed every 6 days, while tNPWT was changed every 3 days, as per the “Instructions for Use” provided with each device (Supplementary Fig. S1A). A purpose made swine jacket with pockets (Lomir Biomedical, Inc., Quebec, Canada) was used to support the NPWT device pumps on the animals.
Wound planimetry analysis
Wounds were digitally photographed on day 0 (n = 12 pigs/24 wounds per treatment group), day 6 (n = 12 pigs/24 wounds per treatment group), and day 12 (n = 8 pigs/16 wounds per treatment group). Macroscopic wound closure analysis was performed using Image Pro Plus v.4.1.0 (Media Cybernetics, MD). The wound area remaining open, and the contribution of reepithelialization and contraction to overall wound closure were measured as described below (Fig. 1A):
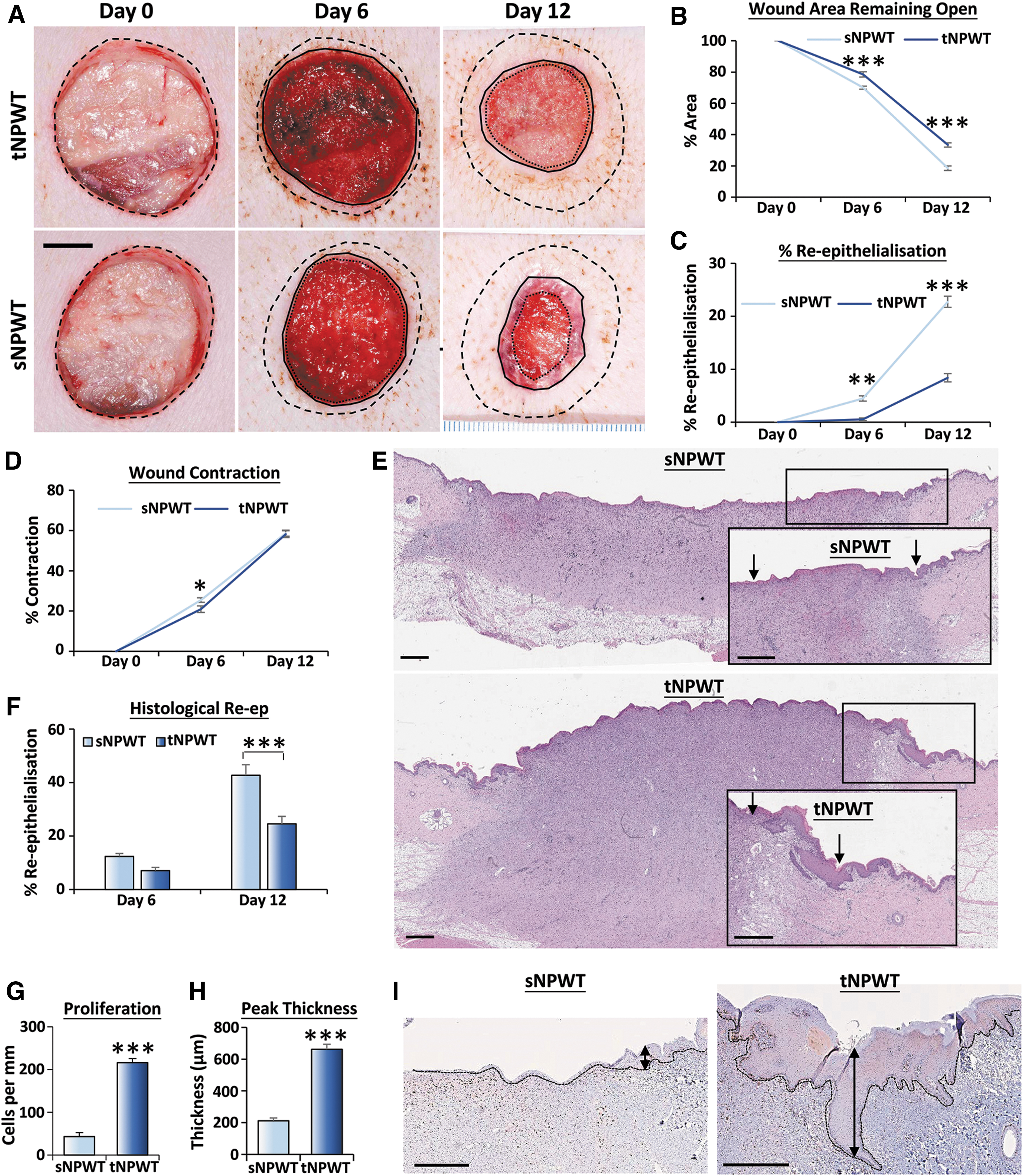
sNPWT accelerates porcine wound closure. sNPWT or tNPWT was applied to 3-cm-diameter full-thickness excisional wounds. Representative macroscopic images showing the impact of treatment over time [
Skin and wound assessment
Surface wound damage was determined at each dressing change, where 0 = no bleeding, 0.5 = removal of surface tissue without bleeding, 1 = minimal bleeding, 2 = moderate bleeding, and 3 = substantial bleeding. Skin color measurements were taken using a spectrophotometer (X-Rite Sp68 Sphere, Manchester, United Kingdom) and expressed using the CIELAB color notation system. A Tewameter® TM 300 was used to measure transepidermal water loss (TEWL) and skin hydration, and a Mexameter® MX 18 probe (both Courage and Khazaka, Germany) was used to measure erythema (using a redness index). These measurements were made, after sNPWT dressing or tNPWT drape removal, in two regions around the wound: (i) the periwound (∼0.5–1 cm away from wound edge) and (ii) the extended zone (2.5–3 cm away from wound edge). For TEWL, an average of the first 30 readings was taken following skin acclimatization after dressing removal. For skin hydration (skin surface moisture), a reading was taken immediately following dressing removal with no acclimatization (at the extended zone site only). Wound depth was assessed in three defined wound regions using a depth gauge. These measurements were taken on n = 12 pigs (24 wounds) on day 6 and n = 8 pigs (16 wounds) on day 12.
Tissue collection
Histological samples were collected from n = 4 pigs harvested on day 6 (n = 8 wounds per treatment group) and n = 4 pigs harvested on day 12 (n = 8 wounds per treatment group), preselected during study planning. Strips (1 cm wide) of wound tissue and marginal skin (craniocaudal orientation) were harvested and placed in 10% buffered formal saline for histological analysis. Wound tissue (n = 4, one wound per pig per time point) was placed in RNAlater™ (Thermo Fisher Scientific, Paisley, United Kingdom) and frozen at −80°C for PCR Array profiling. Normal skin, periwound skin (immediately adjacent to the wound), and extended zone skin (under the sNPWT dressing island, or tNPWT drape) were also collected for comparison.
Histology
Paraffin-embedded sections (6 μm thick) were dewaxed and rehydrated before staining. Hematoxylin and eosin (H&E) was used to visualize trapped filler material and to quantify granulation tissue depth and reepithelialization through Aperio ImageScope image analysis software (Leica Biosystems, Milton Keynes, United Kingdom). Picrosirius Red (PSR) color analysis allowed histological assessment of matrix maturity, where immature (green birefringence) and mature (red birefringence) fibers were visualized by polarizing light and quantified (as in 18 ). For 5-bromo-2′-deoxyuridine (BrdU) analysis, proliferating cells were labeled 1 h before culling by intraperitoneal injection of 1 mg BrdU (B5002; Sigma-Aldrich) in 100 mL physiological saline. BrdU was traced using an anti-BrdU antibody (GE Life Sciences, Buckinghamshire, United Kingdom). Neutrophils were stained using an anti-neutrophil gelatinase-associated lipocalin (NGAL) antibody (Enzo Life Sciences, Inc., New York). Bound antibodies were detected by ABComplex and 3,3′-diaminobenzidine (Vector Laboratories Ltd., Peterborough, United Kingdom). The number of BrdU+ve and NGAL+ve cells was determined using Image Pro Plus.
Transcriptional profiling
Porcine skin and wound tissue were homogenized (T10 basic; IKA, Oxford, United Kingdom) in TRIzol® reagent (Thermo Fisher Scientific). Chloroform was added for phase separation and RNA removed and purified using a PureLink RNA Mini Kit (Thermo Fisher Scientific) following manufacturer's instructions. RNA concentration was determined using a SimpliNano nanodrop (Biochrom, Cambridge, United Kingdom) and adjusted to 1 μg/μL. Reverse transcription was performed with random primers (Promega, Southampton, United Kingdom) and BioScript reverse transcriptase (Bioline, London, United Kingdom). cDNA was diluted in nuclease-free water and each sample plated in RT 2 Profiler™ PCR array plates (Pig Wound Healing; Qiagen, Manchester, United Kingdom) with 2 × Takyon SYBR MasterMix (Eurogentec, Hampshire, United Kingdom). Quantitative real-time polymerase chain reaction (qRT-PCR) was performed and data were analyzed in CFX Manager software on a CFX connect thermocycler (Biorad Laboratories Ltd., Hertfordshire, United Kingdom).
Statistical analyses
All data are presented as mean ± standard error of the mean. Pairwise t tests were performed on data sets comparing sNPWT and tNPWT at one time point. One-way analysis of variance (ANOVA) was performed on qRT-PCR data comparing normal skin and day 12 treatments. Two-way ANOVA was performed on all other data sets with appropriate post-hoc analysis (Tukey or Sidak). Statistical analysis was performed in GraphPad Prism v.7.0 (GraphPad Software, CA). Data were considered significant at the p < 0.05 level.
Results
sNPWT leads to greater wound closure than tNPWT
Planimetric analysis was performed on scaled macroscopic wound images taken on day 0, 6, and 12 (Fig. 1A). The area of the wound remaining open, determined as a percentage of day 0 wound area, was significantly smaller following sNPWT than tNPWT on both day 6 (70.06% vs. 78.55%; p < 0.001) and day 12 (18.56% vs. 33.36%; p < 0.001) postinjury (Fig. 1B). Similarly, macroscopic quantification demonstrated significantly greater reepithelialization with sNPWT compared to tNPWT on days 6 (4.46% vs. 0.55%; p < 0.01) and 12 (22.73% vs. 8.4%; p < 0.001; Fig. 1C). Wound contraction was greater on day 6 for sNPWT-treated wounds (p < 0.05; Fig. 1D) versus tNPWT, and was found to be similar between treatments on day 12. Accelerated reepithelialization following sNPWT treatment was confirmed by histological analysis of H&E-stained tissue sections on day 12 (p < 0.001; Fig. 1E, F). Interestingly, the neoepidermis of wounds under tNPWT was extremely hyperproliferative on day 12, as demonstrated by increased numbers of proliferative (BrdU+ve) cells (p < 0.001; Fig. 1G, I) and increased peak epidermal thickness (Fig. 1H, I). Collectively, these data demonstrate that sNPWT accelerates wound closure compared to tNPWT, with increased epithelial migration and reduced wound edge hyperproliferation.
Reduced wound bed inflammation following sNPWT treatment
Immunohistochemistry for neutrophils was performed to assess the level of early inflammatory cells in porcine NPWT-treated wounds. Quantification showed significantly higher neutrophil numbers in tNPWT-treated wounds compared to sNPWT on day 12 postwounding (Fig. 2A; p < 0.001). Transcriptional profiling revealed statistically significant upregulation of a number of proinflammatory cytokines, including CXCL11 (day 6), CSF2, IL-1α, and IL-1β (day 12) in tNPWT-treated wounds (Fig. 2B–H). Collectively, these findings support higher wound bed inflammation in tNPWT- versus sNPWT-treated wounds.
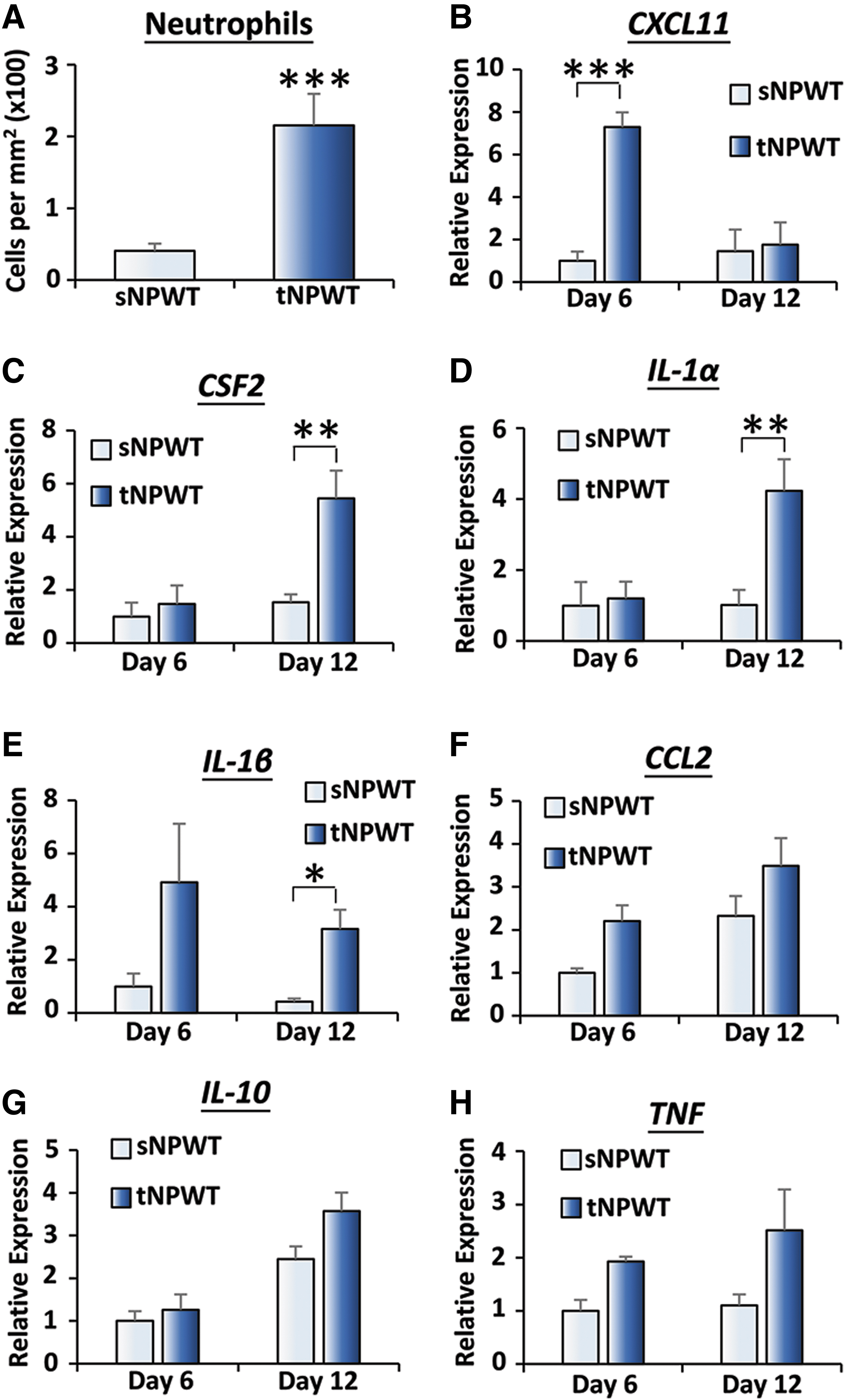
Single-use negative pressure dampens inflammation in porcine wounds. Wounds treated with tNPWT showed increased neutrophil infiltration on day 12
sNPWT promotes granulation tissue maturation and causes less damage to the wound bed than tNPWT
Similar wound filling was observed between sNPWT and tNPWT on day 6. However, by day 12, tNPWT led to significantly reduced macroscopic wound depth (p < 0.001; Fig. 3A) and increased wound granulation tissue deposition (measured by histology; p < 0.001; Fig. 3B) compared to sNPWT. While wounds filled faster under tNPWT, the quality and maturity of granulation tissue formed in these wounds were inferior to that following sNPWT application. PSR staining determined granulation tissue extracellular matrix maturity in discrete upper wound regions (Fig. 3C–F). Here, sNPWT led to significantly increased total collagen deposition (bright field; p < 0.05; Fig. 3E). Polarizing light microscopy revealed that sNPWT treatment increased both immature (green birefringence) and mature (red birefringence) collagen fiber deposition compared to tNPWT (p < 0.001; Fig. 3D, F).
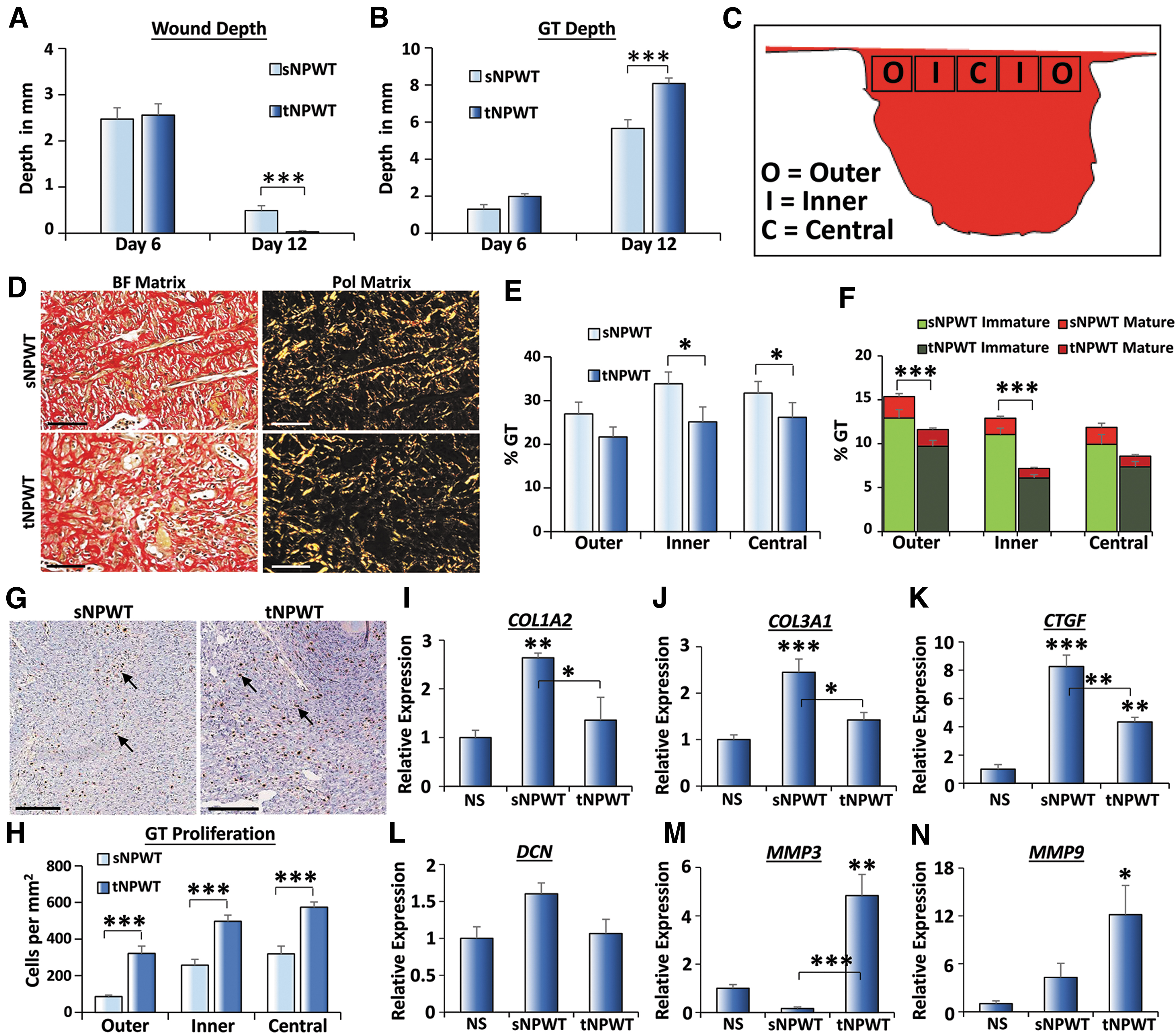
Porcine wound maturation is accelerated with sNPWT compared to traditional application. Increased wound depth
Wound maturation was evaluated by measuring the level of granulation tissue cellular proliferation. In this study, sNPWT-treated upper wound tissue contained fewer BrdU+ve cells versus tNPWT (p < 0.001; Fig. 3G, H). qRT-PCR array analysis further substantiated increased maturity of sNPWT wounds, with higher expression of wound matrix components, COL1A2 (p < 0.01; Fig. 3I) and COL3A1 (p < 0.001; Fig. 3J), granulation-promoting factors, CTGF (p < 0.001; Fig. 3K), and proteoglycans, DCN (Fig. 3L), in sNPWT wounds. By contrast, tNPWT-treated wounds displayed substantially elevated levels of the tissue remodeling matrix metalloproteinases (MMPs), MMP3 (p < 0.01; Fig. 3M) and MMP9 (p < 0.05; Fig. 3N), but not MMP2 (Supplementary Fig. S2A).
Evaluation of H&E-stained sections revealed trapped filler material/foreign body reactions in 50% of tNPWT-treated wounds (representative images in Fig. 4A). By contrast, no trapped filler material or foreign body reactions were detected in any sNPWT-treated wounds. In addition, tNPWT dressing removal resulted in significantly more wound surface damage with noticeable bleeding compared to removal of sNPWT dressing on day 6 (p < 0.001) and day 12 (p < 0.001; Fig. 4B). Overall, these data reveal that sNPWT increased granulation tissue maturation, without the trapped filler and damage observed following tNPWT.
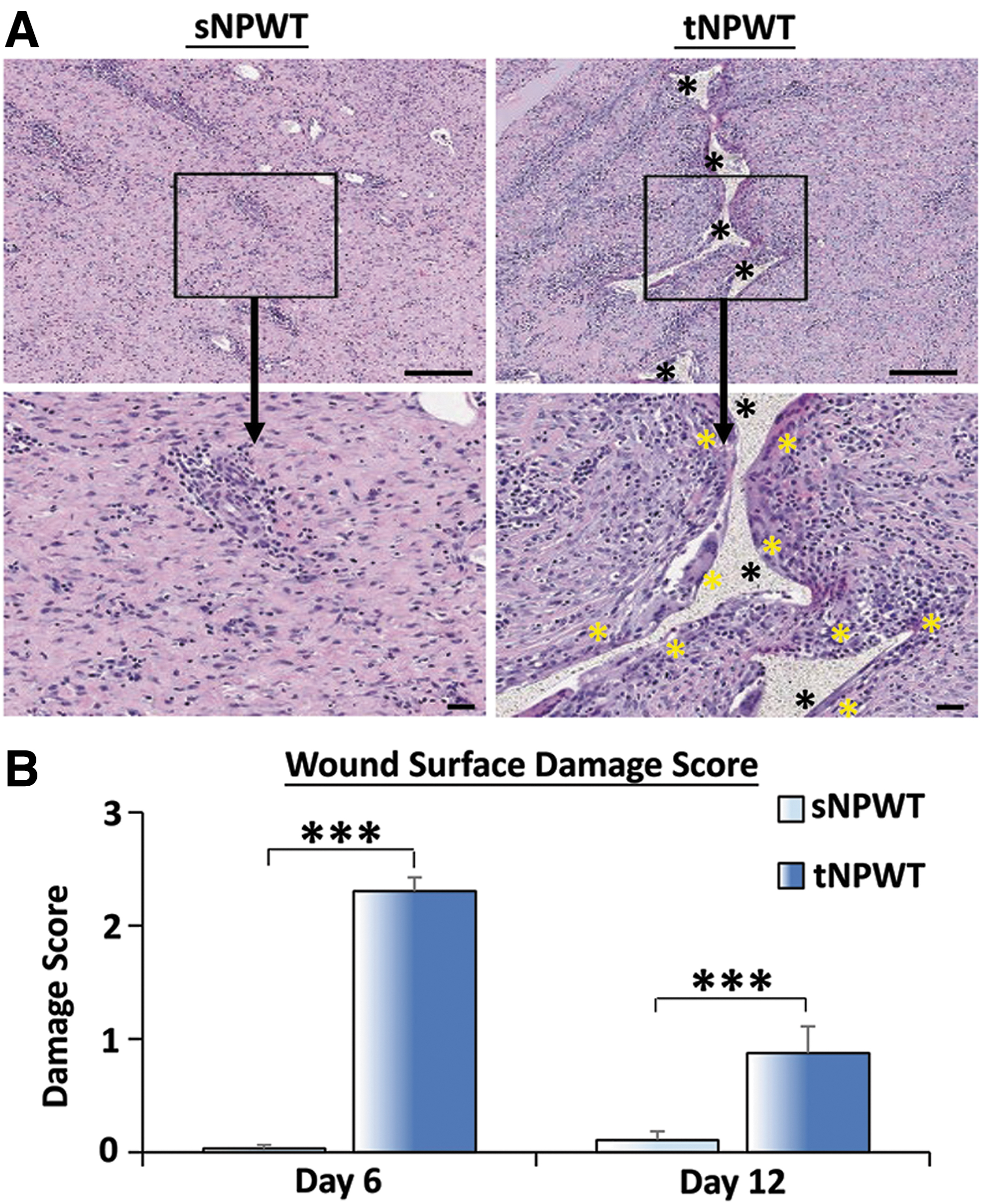
Filler foam in tNPWT causes wound damage. tNPWT left foam in wounds [
Reduced surrounding skin disruption with sNPWT versus tNPWT
Skin barrier function and erythema were assessed in the periwound skin and the extended zone (schematic, Supplementary Fig. S1B) to determine whether NPWT application affected the function of skin surrounding the wound. Extended zone skin hydration, measured immediately after dressing or drape removal, revealed significantly higher moisture content in skin under tNPWT compared to skin under sNPWT (p < 0.001 on days 6 and 12; Fig. 5A). In addition, TEWL, a direct measure of skin barrier, was significantly elevated in periwound skin under the tNPWT drape compared to that under the sNPWT dressings (p < 0.001; Fig. 5B). The redness (erythema) of tNPWT-treated periwound skin was significantly greater than sNPWT-treated skin (p < 0.001; Fig. 5C), with a nonsignificant trend toward an increased erythema index (Fig. 5D). Collectively, these in vivo data suggest that sNPWT causes far less disruption to the skin surrounding a wound.
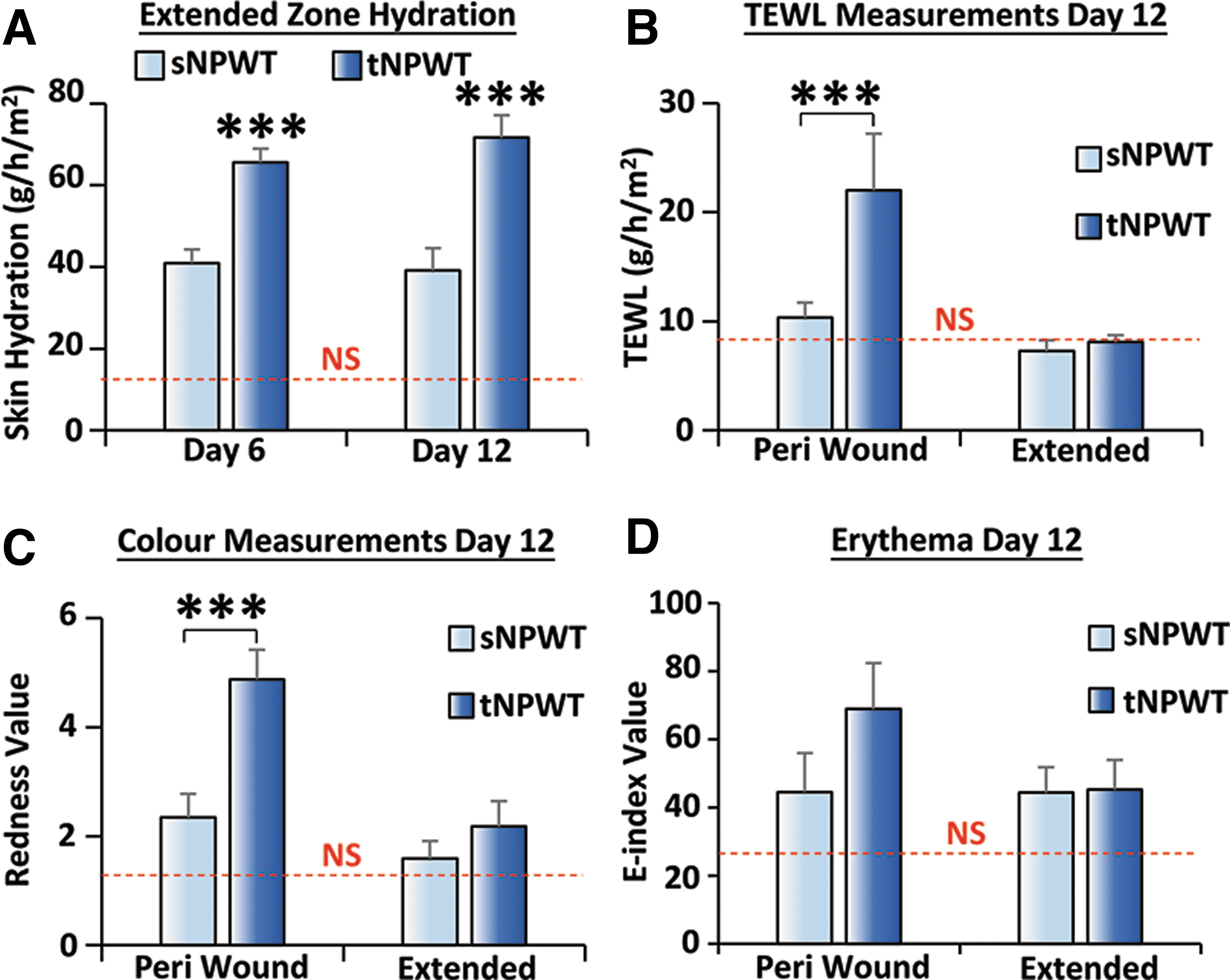
tNPWT increases erythema and TEWL in periwound skin. tNPWT increased hydration in the extended zone region
tNPWT, but not sNPWT, causes heightened proliferation and inflammation in periwound skin
Next, the cellular correlates to the observed reduced redness and TEWL in sNPWT-treated periwound skin were assessed histologically. Reduced epidermal BrdU+ve (proliferating) cells were observed in the sNPWT-treated periwound tissue on day 6 (p < 0.05) and day 12 (p < 0.05; Fig. 6A, B), commensurate with reduced tissue damage. Transcriptional analysis revealed elevated inflammation in tNPWT-treated periwound skin with upregulation of the inflammatory markers CSF2 (p < 0.05; Fig. 6C), IL-1α (Fig. 6D), and IL-1β (p < 0.05; Fig. 6E). In addition, MMP2 was specifically upregulated on day 6 (p < 0.05; Fig. 6F and Supplementary Fig. S2). Taken together, these data suggest that tNPWT treatment adversely influences the periwound skin region, while sNPWT supports a prohealing wound edge environment.
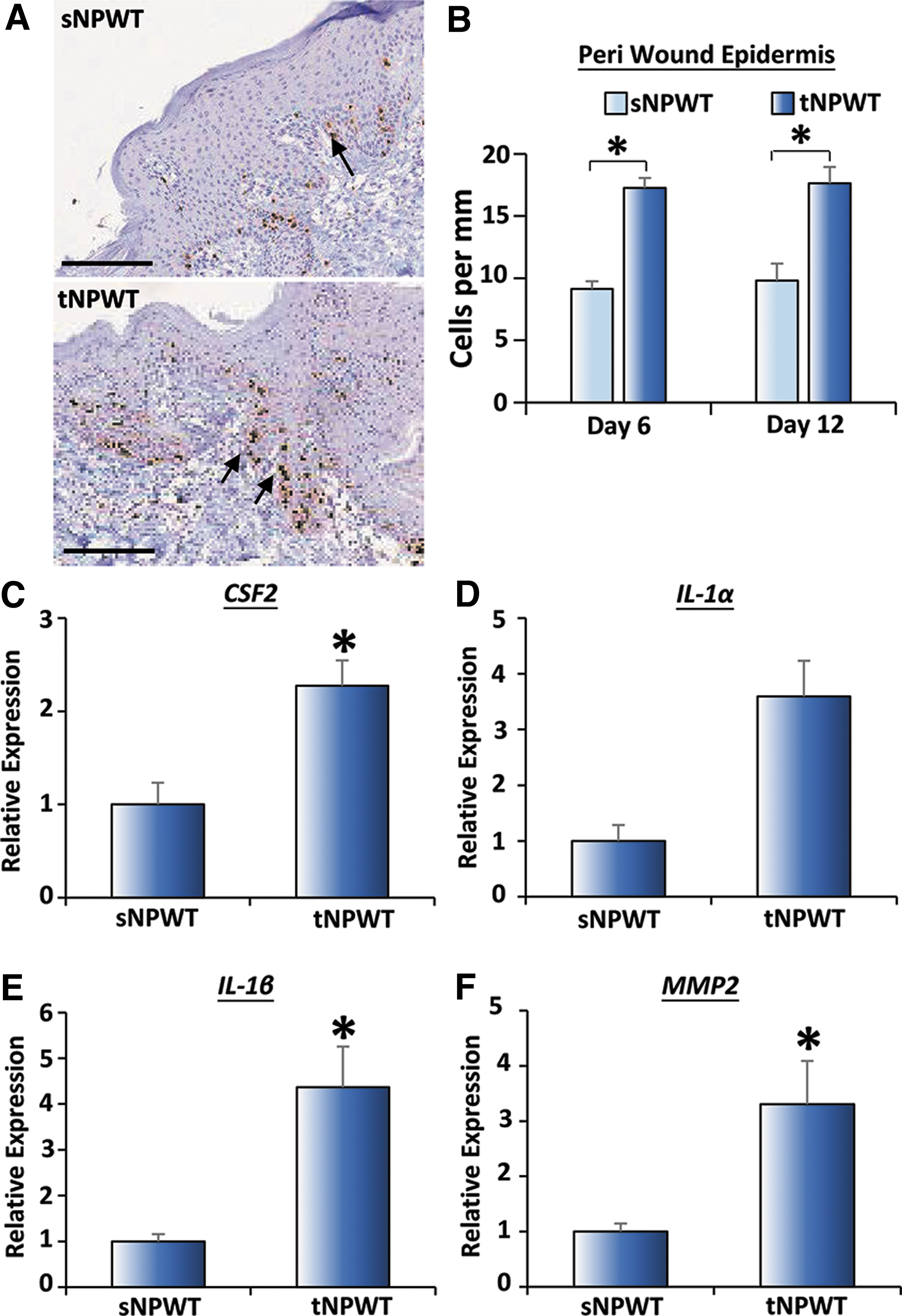
tNPWT causes inflammatory damage to periwound skin. tNPWT increased periwound epidermal proliferation on day 6 and 12 [
Discussion
tNPWT devices were successfully implemented in wound treatment over 20 years ago. 11,19 In these applications, a wound filler (foam or gauze) is required to deliver negative pressure to the wound bed and to serve as a fluid conduit. As previously mentioned, the PICO sNPWT system uses a very different technology, a silicone wound interface dressing with an incompressible airlock layer that transmits pressure evenly across the wound bed, periwound, and wider skin region. 20 Interestingly, a recent randomized control trial demonstrated that sNPWT achieved greater wound closure (45%) compared to tNPWT (22%) with fewer adverse events, such as wound maceration. 21 Concurrent cost-based analysis revealed that sNPWT was more cost-effective than tNPWT, 22 suggesting benefits that extend beyond the patient.
This study was specifically designed to explore the mode of action of sNPWT compared to tNPWT using an in vivo porcine wound repair model. Note, previous studies (e.g., 23 ) have performed direct porcine side-by-side comparison of tNPWT devices demonstrating relative equivalence. In this study, we report, for the first time, detailed macroscopic and histological comparison of sNPWT and tNPWT in vivo. We show that sNPWT accelerated wound closure, promoted wound reepithelialization, and increased granulation tissue maturity when compared with tNPWT. In fact, tNPWT actively prevented reepithelialization, inducing substantial wound edge epidermal hyperproliferation. tNPWT-treated wounds also displayed extensive filler material trapped in the granulation tissue (observed in earlier studies; in pigs 24,25 and in patients 26 –28 ), which may contribute to heightened local tissue inflammation. 29
NPWT-associated healing has previously been linked to dampened proinflammatory cytokines, TNFα and IL-1β, compared to non-NPWT treatment. 30,31 In our study, tNPWT-treated wound granulation tissue displayed increased inflammation and upregulation of the proinflammatory the cytokines, CSF2, CXCL11, IL-1α, and IL-1β, compared to sNPWT treatment. The heightened damage response following tNPWT extended to the periwound skin region, which also contained increased proinflammatory marker expression and increased redness, indicative of erythema. 32 This local damage likely results from both the differential forces experienced by tNPWT- and sNPWT-treated wounds, and the differences in frequency of dressing change. Interestingly, Karabacak et al. 33 report that compressional injury from tNPWT drape drainage tubes can cause spontaneous wound formation in compromised skin surrounding a wound.
Higher TEWL and excessive hydration were observed in the skin surrounding tNPWT-treated wounds. TEWL is a direct measure of skin barrier integrity, where higher TEWL is associated with a compromised barrier. 34,35 High TEWL is a potential indicator of skin maceration risk, an observation noted by Kirsner et al. 21 in their randomized control trial, following tNPWT use. Loss of barrier integrity also increases the risk of infection, 36 a common problem when negative pressure application fails and wound exudate is not effectively managed. 26 Indeed, in this study, sNPWT delivered active therapy 97% of the time requiring only 14 device-related interventions, versus 24 interventions to correct leaks and blockages under tNPWT.
In addition to neoepidermal hyperproliferation, tNPWT caused excessive cellular proliferation in the periwound region and in the wound granulation tissue. High levels of epidermal proliferation are a hallmark of wound pathology, and have previously been observed following tape stripping, 37 suggesting that tNPWT dressing removal may cause similar damage. By contrast, mature wound granulation tissue is typically characterized as relatively acellular. 38 In this study, granulation tissue of tNPWT-treated wounds was highly proliferative, with fewer mature collagen fibers and increased wound MMPs, indicating reduced maturation compared to sNPWT. Overall, these data suggest that sNPWT independently promotes granulation tissue maturation and reepithelialization. Indeed, these two aspects could be closely linked, with a mature wound bed important to permit active reepithelialization.
Data now show a direct link between compromised skin barrier and subsequent wound recurrence, 39 a significant consideration for chronic wound management. Although several clinical studies have demonstrated enhanced wound closure and faster granulation with tNPWT, 40,41 few studies have performed follow-up assessments to determine rates of wound recurrence. 42 A future preclinical in vivo investigation would provide a unique opportunity to explore recurrence, an important and often overlooked aspect of wound healing studies.
Innovation
The results of this preclinical in vivo study clearly demonstrate that sNPWT, which delivers negative pressure using a unique multilayered interface technology, promotes faster healing than tNPWT. While tNPWT treatment led to wound damage and inflammation, sNPWT stimulated faster reepithelialization and promoted granulation tissue maturation. This study therefore provides new mechanistic insight that informs the enhanced wound healing outcomes of sNPWT observed in the clinical setting.
KEY FINDINGS
sNPWT promotes a faster rate of wound closure than tNPWT in an in vivo porcine model.
sNPWT improves multiple aspects of healing, promoting reepithelialization, dampening inflammation, and increasing granulation tissue maturity.
sNPWT avoids the detrimental effects of tNPWT on the periwound epithelium.
sNPWT appears to circumvent the foam-trapping and foreign body reactions that are frequently observed with tNPWT.
Footnotes
Acknowledgments and Funding Sources
We would like to thank Benjamin Gardner for assistance with sNPWT device pump analysis. This study was funded by TJ Smith and Nephew Ltd. in collaboration with the University of Hull and Cica Biomedical Ltd.
Author Disclosure and Ghostwriting
The content of this study was exclusively contributed and written by the authors listed. V.R.B., E.H., and I.W. are employees of TJ Smith and Nephew Ltd. The authors declare no other conflicts of interest. No ghost writers were involved in the completion of this article.
About the Authors
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.