
Abstract
Background:
Psychological symptoms and sleep disturbance are common during pregnancy. Observational data suggest that being physically active during pregnancy is related to better mood and sleep, but whether sedentary behavior reduction interventions provide similar benefits is untested. We aimed to determine whether reducing sedentary behavior across pregnancy improved psychological and sleep parameters.
Methods:
Pregnant participants (n = 51) were allocated 2:1 to a sedentary behavior reduction intervention or control in their first trimester. Depressive symptoms, perceived stress, mood disturbance, nausea/vomiting quality of life, and sleep parameters were assessed with validated questionnaires in each trimester. Linear mixed effects regression examined differences between groups across pregnancy. Spearman correlations tested whether changes in sedentary time and physical activity were associated with changes in psychological and sleep outcomes without regard to group.
Results:
Despite significant reductions in sedentary behavior (−0.84 hour/day), the intervention had no effect on psychological health outcomes. Further, intervention participants demonstrated significant worsening of sleep efficiency factor scores compared with control (p = 0.038). Small but significant correlations were found between changes in sedentary time and nausea/vomiting quality of life, and between changes in physical activity and nausea/vomiting quality of life, sleep duration, and sleep efficiency.
Conclusions:
Reducing sedentary behavior during pregnancy did not improve psychological symptoms and may worsen sleep efficiency. Recommendations for future sedentary behavior reduction research in pregnancy include a larger sample with poorer psychological health and sleep at baseline, targeting reductions in mentally passive sedentary behavior, and including device-based sleep assessments.
Introduction
Pregnancy is a dynamic period, during which many individuals experience worsening of psychological and sleep outcomes. Between 10% and 20% of pregnant individuals develop depression during pregnancy, which can continue postpartum. 1 Also, many pregnant individuals report being mildly to moderately stressed during pregnancy,2,3 and mood instability tends to be higher in pregnant individuals compared with their nonpregnant counterparts. 4 Additionally, sleep duration and quality are often poor during pregnancy. 5 Exploring strategies to improve mood and sleep during pregnancy is a priority, as suboptimal mood and sleep are associated with an increased incidence of adverse pregnancy outcomes such as preeclampsia.1,6–8 Further, if these issues persist postpartum, there is an increased risk of poor maternal outcomes, such as suicide, and behavioral, cognitive, and health problems in the child.1,2,4
Physical activity has been shown to improve many psychological9,10 and sleep 11 outcomes during pregnancy, with the American College of Obstetrics and Gynecology recommending at least 150 minutes of moderate-intensity physical activity per week. 12 However, fewer than 40% of pregnant people in the United States are estimated to meet this recommendation. 13 This may be a consequence of barriers pregnant individuals face to being physically active, such as increased fatigue, pregnancy-related discomforts, and lack of time. 14 The limited number of pregnant individuals meeting physical activity recommendations, coupled with the increased barriers to physical activity, suggests that exploring new strategies to improve psychological and sleep outcomes during pregnancy is necessary.
Sedentary behavior, defined as time spent seated or lying down with low energy expenditure, is distinct from physical activity. This can be understood by the fact that it is possible to be both highly active and highly sedentary, for example, by exercising daily after sitting all day at work. Furthermore, sedentary behavior appears to confer risk for poor psychological and pregnancy outcomes that is independent of physical inactivity.15–17 Research in nonpregnant populations suggests that higher levels of sedentary behavior are associated with a higher depression risk.18,19 Regarding sleep, sedentary behavior is associated with several poor sleep parameters.20–23 Fewer data on the potential risks of excessive sedentary behavior are available in pregnant populations, especially for sleep outcomes, but a recent systematic review suggests that longer sedentary time is associated with a higher risk of postpartum depression. 24
Sedentary behavior reduction may be a promising, approachable behavioral strategy to improve psychological and sleep outcomes in pregnant populations who may struggle to add more intense physical activity as recommended. However, the current evidence base is largely observational. Therefore, the experimental evidence testing the effects of reducing sedentary behavior during pregnancy on changes in psychological and sleep outcomes should be explored.
The Sedentary Behavior Reduction in Pregnancy Intervention (SPRING) was a randomized multi-component pilot and feasibility intervention trial (n = 51) in the second and third trimesters of pregnancy that sought to reduce sedentary behavior while increasing standing and steps.25,26 The behavioral intervention included individualized coaching, a sit-stand desk, a wearable activity device, and a social media group, while the control group received a handout with physical activity recommendations. The intervention successfully reduced sedentary behavior by 0.84 hour/day and increased standing by 0.77 hour/day, with no significant changes in the control group. Psychological and sleep data were collected as exploratory outcomes and are the focus of this report. Here, we use data from the SPRING randomized clinical trial to:
Investigate the effect of the SPRING intervention on psychological and sleep outcomes across pregnancy compared with controls, and Assess the relationship between changes in sedentary behavior and physical activity with changes in psychological and sleep outcomes during pregnancy, without regard to a randomized group.
Methods
Participants
Participants were enrolled in their first trimester of pregnancy and were at risk of both high sedentary behavior (to enable meaningful reductions with intervention) and adverse pregnancy outcomes (to intervene upon individuals at higher risk for these exploratory outcomes), as described previously.25,26 Eligible participants reported high sedentary behavior at screening, for example, a job that was primarily sitting or fewer than 6000 steps per day from a wearable activity monitor. In addition, participants had at least one risk factor for an adverse pregnancy outcome, including nulliparity, a body mass index (BMI) of at least 30 kg/m2, a history of an adverse outcome in a prior pregnancy, and/or being 35 years of age or older. Ethical approval was provided by the local review board, and all participants provided written informed consent.
Assessments
Assessments were conducted in each trimester. Baseline assessments took place between 100 and 126 weeks of gestation, and second and third trimester follow-up assessments occurred between 200−226 and 320−346 weeks, respectively. Participants completed validated questionnaires to assess mood, quality of life, and sleep parameters.
Depressive symptoms were assessed using the Center for Epidemiological Studies—Depression scale (CES-D), 27 in which scores ranged from 0 to 30 and a score ≥15 was indicative of elevated depressive symptoms. Perceived stress was ascertained from the Perceived Stress Scale (PSS), 28 with scores ranging from 0 to 40. Higher PSS scores suggest greater perceived stress. Pregnancy quality of life was assessed using the Health-Related Quality of Life for Nausea and Vomiting during Pregnancy scale (NVPQoL), 29 with higher scores suggesting worse quality of life. Overall mood was assessed using the 40-item profile of mood states.4,30 Total mood disturbance (TMD) was calculated by summing item scores for the tension, anger, fatigue, depression, esteem-related affect, and confusion subscales, then subtracting the summed item scores for the vigor subscale. A higher score indicates worse mood disturbance.
Sleep parameters were self-reported using the Pittsburgh Sleep Quality Index 31 (PSQI). The instrument includes subscales for duration, sleep disturbances, sleep latency, daytime dysfunction, sleep efficiency, sleep quality, and medication use. The global PSQI score is calculated by summing each subscale; a score greater than 5 indicates poor sleep quality. In addition, factor scores were calculated for quality (the sum of the sleep quality, sleep latency, and medication use subscales), daily disturbances (the sum of the sleep disturbances and daytime dysfunction subscales), and efficiency (the sum of the sleep duration and sleep efficiency subscales). 32 Finally, continuous values of sleep duration (hours) and sleep efficiency (percentage) were analyzed.
To assess sedentary behavior and physical activity, participants wore a thigh-mounted activPAL3 micro accelerometer (PAL Technologies, Glasgow, Scotland) continuously for one week in each trimester, removing it only for swimming activities, and completed a concurrent wear diary. After processing using PALTechnologies software, event files and daily summaries were downloaded, and a diary-informed cleaning approach was used to determine waking wear time. For those with at least 5 valid days of wear, sedentary behavior was analyzed both as total daily duration and percentage of total wear time. Time spent in moderate-to-vigorous physical activity (MVPA) was estimated as minutes per day during which the participant achieved at least 100 steps per minute from the daily summaries from valid days. Given that the intervention targeted sedentary behavior, we chose to only analyze device-based data because prior literature has shown that self-report measures such as the Pregnancy Physical Activity Questionnaire have low validity for sedentary behavior. 33
Randomization and intervention
The randomization and intervention protocol has been described in detail previously.25,26 In brief, participants were randomly allocated 2:1 to either a sedentary behavior reduction intervention or a no-contact control group following the baseline assessment. Intervention participants received a multi-level intervention that included biweekly individual behavioral coaching, inclusion in a study-administered social media group, a height-adjustable workstation, and a wearable fitness tracker. Behavioral sessions focused on decreasing sitting time by increasing standing and stepping behaviors. No-contact control participants were urged to maintain their usual activity patterns.
Statistical analyses
Mixed-effect linear regression models using an interaction term between intervention group and trimester were used to examine whether the sedentary behavior reduction intervention yielded any changes in sleep, depressive symptoms, perceived stress, health-related quality of life, or mood parameters over the intervention period compared with controls. In addition, Spearman rank correlations between changes in behaviors (sedentary behavior, steps per day, and MVPA) with changes in mood, sleep, and quality of life outcomes from the baseline visit to the follow-up visits were examined in the full sample, without regard to the intervention group. Analyses were conducted using Stata version 18 (StataCorp, College Station, TX), and significance was accepted at p < 0.05.
Results
Participants in the SPRING Study (N = 51) were on average (standard deviation [SD]) 32.0 (4.3) years old with a pre-pregnancy BMI of 28.0 (8.8) kg/m2. As shown in Table 1, no significant differences were found between the intervention (n = 34) and control (n = 17) groups for demographic or pregnancy characteristics, and the groups had similar baseline values for all mood, quality of life, and sleep parameters.
Descriptive Characteristics and Baseline Scores for Psychological and Sleep Parameters by Randomized Group
Data presented as mean (SD) or frequency (%). APO, adverse pregnancy outcome; BMI, body mass index; PSQI, Pittsburgh Sleep Quality Index.
Effect of the intervention
Raw scores for outcome variables by trimester and group can be found in Supplementary Table S1. Results of linear mixed effects models found no significant interactions between intervention status and trimester for depressive symptoms, perceived stress, total mood disturbance, or NVPQoL (Fig. 1). No main effect of intervention status was found for any mood or quality of life outcome. The main effect of trimester was only significant for NVPQoL, in which nausea and vomiting quality of life symptoms improved in the second and third trimesters compared with the first (p = 0.001).
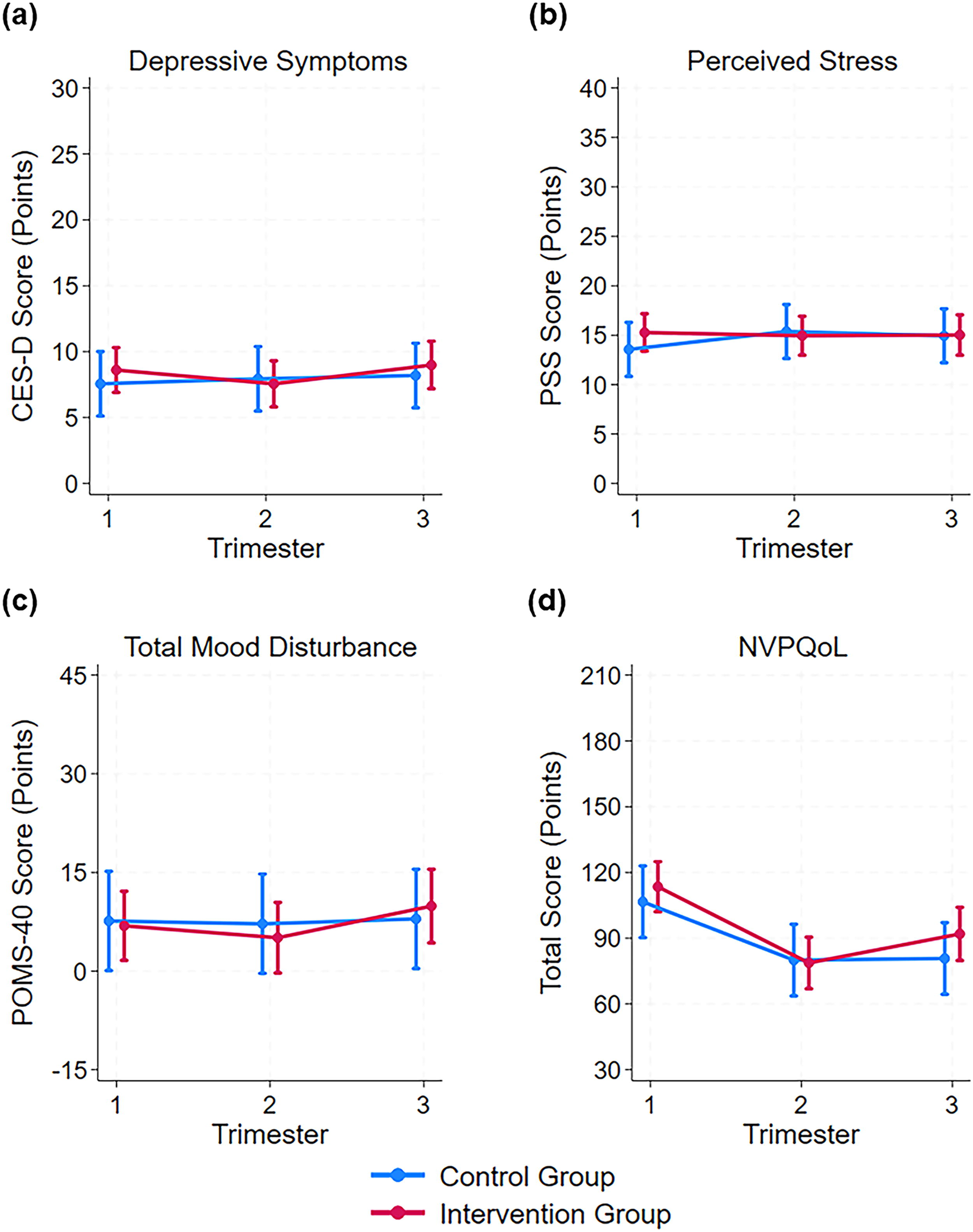
Psychological well-being and quality of life marginal mean scores (95% CI) at each trimester by intervention condition for
Results of linear mixed effects models for the sleep parameters are shown in Figure 2. A significant interaction effect of the intervention group by trimester was found only for the efficiency factor score (Fig. 2d), in which those in the intervention group had worsening efficiency factor scores as pregnancy progressed while there was no change across pregnancy in the control group (p = 0.038). No significant main effects of either intervention status or trimester were found for any sleep parameters.

Sleep characteristic marginal means (95% CI) at each trimester by intervention condition for
Correlations with sedentary time and MVPA
As shown in Table 2, changes in sedentary time, steps per day, and MVPA from the first to second or the first to third trimesters were not correlated with changes in depressive symptoms, perceived stress, or total mood disturbance over the same time periods. Small-to-moderate significant correlations, ranging from |0.32| to |0.45|, were seen between changes in sedentary time, steps per day, and MVPA and changes in NVPQoL symptoms. Less sedentary time, more steps per day, and greater MVPA were each correlated with decreased NVPQoL symptoms, and these correlations were stronger when comparing the change from the first to the third trimesters versus the change from the first to the second trimesters.
Spearman Rank Correlations Between Changes in Mood/Quality of Life Parameters and Changes in Movement Behaviors from the First to Second and First to Third Trimesters
A positive change means the later trimester value is higher than the first trimester value.
Indicates p < 0.05.
CES-D, Center for Epidemiological Studies—Depression scale; MVPA, moderate-to-vigorous physical activity; NVPQoL, Health-Related Quality of Life for Nausea and Vomiting during Pregnancy scale; PSS, Perceived Stress Scale; Sed, sedentary; TMD, total mood disturbance.
Correlations of changes in sedentary time, steps per day, and MVPA with changes in sleep parameters are shown in Table 3. When looking at the changes from the first to the second trimester, small but significant positive correlations were found between increases in sedentary time and unfavorable increases in the global PSQI score, increases in steps per day with favorable increases in sleep duration and sleep efficiency, and increases in MVPA with favorable increases in sleep duration. A small, significant negative correlation was found between increases in MVPA and favorable decreases in the efficiency factor score. When looking at changes from the first to the third trimesters, only a small significant negative correlation was found between increases in MVPA and favorable decreases in the quality factor score.
Spearman Rank Correlations Between Changes in Sleep Parameters and Changes in Movement Behaviors from the First to Second and First to Third Trimesters
A positive change means the later trimester value is higher than the first trimester value.
Indicates p < 0.05.
MVPA, moderate-to-vigorous physical activity; PSQI, Pittsburgh Sleep Quality Index; Sed, sedentary.
Discussion
Our study found that the SPRING intervention had no effect on measures of psychological factors during pregnancy; however, surprisingly, intervention participants demonstrated a significant worsening of the sleep efficiency factor score over pregnancy compared with control participants. Yet, more consistent with our expectations, we found several small significant correlations between increases in physical activity and decreases in sedentary behavior with beneficial changes in nausea/vomiting quality of life scores and several sleep parameters. These findings suggest a possible relationship between changes in physical activity and sedentary behavior with changes in nausea/vomiting quality of life and sleep health which could be bidirectional or in the reverse direction—where beneficial changes in the outcomes as pregnancy progresses lead to less sedentary behavior and more physical activity.
Our findings that the intervention did not improve psychological outcomes across pregnancy align with other studies, including interventions, in nonpregnant adults that found no association between sedentary behavior reduction and psychological factors. 34 Changes in mentally active rather than mentally passive sedentary behavior may explain why there were no differences in psychological factors between groups in the SPRING intervention. 35 A meta-analysis found that mentally passive sedentary behavior, such as television watching, is associated with increased depression risk, while mentally active sedentary behavior, which includes working on a computer, is not. 36 Since the SPRING intervention participants were provided with a sit-stand desk, it is likely that they mainly decreased their mentally active sedentary behavior. If more leisure or mentally passive sedentary behaviors were decreased, there may have been a significant intervention effect on depressive symptoms and possibly other psychological factors. Furthermore, average depressive symptoms, perceived stress, and mood disturbances were low across pregnancy in both groups, which could have resulted in a floor effect. We may have observed an intervention benefit in a sample with a poorer psychological profile at baseline.
It is unclear why the intervention group experienced significantly worsening sleep efficiency factor scores compared with the control group. Observational evidence in pregnant women suggests that those with low sleep efficiency may engage in less sedentary behavior, and those with longer sleep duration also accumulate more sedentary time,37,38 and our findings indicate that reducing sedentary behavior may cause lower sleep efficiency and duration. Baseline demographics, pregnancy characteristics, psychological factors, and sleep parameters were similar across groups, so it is unlikely issues such as parity were confounding factors. Additionally, the main findings of SPRING reported that 54% of intervention participants reported being more comfortable, 42% reported less pain, and 42% reported less swelling after completing the intervention. 25 Therefore, it is unlikely that worsening sleep efficiency and duration were due to increased musculoskeletal pain from the intervention effect of increased standing. Future research is needed to understand the mechanisms that could explain this unexpected finding. Of note, the mean global PSQI score ranged between 6.3 and 8.9 across trimesters for both groups at all three time points (see Supplementary Table S1). This finding aligns with previous studies that have found that sleep is generally poor during pregnancy.5,39
When we examined correlations between changes in movement behaviors and changes in psychological and sleep outcomes without regard to the intervention group, we found that decreases in sedentary behavior and increases in physical activity between trimesters were only correlated with beneficial changes in the nausea/vomiting quality of life scores and sleep parameters. In line with these findings, a recent study of pregnant women found that moderate-intensity physical activity was associated with better quality of life. 40 Given that we did not find a significant effect of the intervention, one plausible explanation is that those with declining symptoms of nausea or vomiting were able to participate in a more active, less sedentary lifestyle (rather than more activity causing an easing of symptoms). This is consistent with reported facilitators of sedentary behavior and barriers to physical activity in pregnancy that include pregnancy-related symptoms of nausea and fatigue.14,41 Regarding sleep parameters, we found a general trend that more physical activity was associated with better sleep efficiency, duration, and quality; sedentary time was not correlated with sleep parameters in this sample. These findings are in line with previous literature in pregnant and nonpregnant adults. A longitudinal study of over 2000 pregnant women found that physical activity was positively associated with healthy sleep parameters, 42 and a systematic review and meta-analysis in nonpregnant adults found that prolonged sedentary behavior was associated with less healthy sleep parameters such as increased risk of insomnia, more sleep disturbances, and poorer sleep quality. 20 Another study aligning with our findings was a pregnancy cohort study comparing sedentary behavior and sleep duration in individuals who were pregnant prior to versus during the COVID pandemic. 38 This study found that the pre-COVID participants had less sedentary behavior and shorter sleep during the third trimester than the pandemic-era participants.
Although our study uncovered the effects of the SPRING intervention on psychological and sleep parameters along with correlations between specific behavior and outcome changes, it has limitations. Being a pilot study, the sample size of SPRING was small. Also, the randomization of SPRING was 2:1 in favor of the intervention group, which further limited our power to detect between-group differences. Finally, device-based sleep data were not obtained; self-reported and device-based data are only mildly correlated with each other and often provide complementary insights about separate sleep domains. 43 Considering these limitations, the results of this study should be verified in a larger sample and include a multi-modal assessment of sleep.
Despite these limitations, this study had several strengths. First, SPRING employed a randomized controlled trial study design, a rigorous approach to investigating the causal relationships between the intervention (which successfully reduced sedentary behavior) and outcomes. Next, SPRING tracked participants during each pregnancy trimester, providing a better understanding of behavior and outcome changes across pregnancy. SPRING also used a best practice, device-based sedentary behavior measurement via thigh-worn accelerometry, which uniquely measures posture and intensity and has been validated for pregnant populations. 33
Conclusion
Contrary to our hypothesis, the SPRING intervention did not improve depressive symptoms, stress, pregnancy quality of life, and overall mood but had a negative effect on self-reported sleep efficiency factor scores during the third trimester of pregnancy. Increases in physical activity were more often positively correlated with quality of life as related to nausea and vomiting and sleep parameters than sedentary behavior. Therefore, although decreasing sedentary behavior may be a more feasible or approachable behavior change during pregnancy than increasing physical activity, it may be less effective for improving psychological and sleep health. Future research should verify our findings with a larger sample size, and interventions aiming to decrease sedentary behavior in pregnant women may also target decreases in mentally passive sedentary behavior (e.g., leisure screen time) instead of mentally active sedentary behavior.
Footnotes
Acknowledgments
The authors gratefully acknowledge the SPRING Study participants, along with the contributions of students and study staff: Meghan Savidge, Alexis Thrower, Shannon McAdoo, Alyona Osadcha, PrimaDouris Ngumah, Joshua Paley, and Sabera Rahman.
Authors’ Contributions
A.C.K.: Conceptualization; data curation; methodology; analysis; writing—original draft; visualization. K.L.W.: Conceptualization; data curation; analysis; writing—original draft. C.E.K.: Methodology; writing—review and editing. K.K.D.: Methodology; writing—review and editing. A.H.: Methodology; writing—review and editing. J.M.C.: Methodology; supervision; writing—review and editing. B.B.G.: Funding acquisition; conceptualization; supervision; data curation; methodology; analysis; writing—review and editing.
Author Disclosure Statement
All authors report no conflicts of interest.
Funding Information
The SPRING Study was funded by the American Heart Association (20TPA354909) and recruitment was supported by the University of Pittsburgh’s Clinical and Translational Sciences Institute (UL1TR001857). A.C.K. is supported by the National Heart, Lung, and Blood Institute (T32HL083825).
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.