
Abstract
Introduction:
Federally qualified health centers (FQHCs) provide essential contraceptive services to low-income individuals; yet, access to all method options, notably intrauterine devices (IUDs) and implants, may be limited at non-Title X FQHCs. The South Carolina (SC) Choose Well initiative is a statewide contraceptive access initiative that was launched in 2017 and extends into 2022. Choose Well established a collaborative network between training and clinical partners and is aimed at facilitating implementation of contraceptive care best practices through capacity-building and training of clinical and administrative staff in partner organizations. The initiative provided funding for workforce expansion and contraceptive methods. We examined perceptions of staff from Choose Well-participating FQHCs regarding contraceptive access during the first 2 years of the initiative, including factors that facilitated or posed access challenges as well as sustaining factors. This study informs the process evaluation of Choose Well while providing data critical for uncovering and scaling up contraceptive access initiatives.
Materials and Methods:
Interviews were conducted with FQHC staff (n = 34) in 2018 and 2019 to assess Choose Well implementation and were recorded, transcribed, and double-coded via at least 80% interrater reliability or consensus coding. Data were analyzed according to clinical and administrative factors influencing contraceptive access.
Results:
Increased capacity for contraceptive counseling and provision through training and external funding for IUDs and implants were the most noted clinical factors facilitating access. Streamlining workflow processes was also a facilitator. Buy-in and engagement among staff and leadership emerged as a facilitator at some clinics and as a barrier at others. Policy/structural factors related to costs of devices and insurance coverage were identified as threats to sustainability.
Conclusions:
The Choose Well initiative contributed to the perception of an increase in contraceptive access at participating FQHCs in SC. Statewide contraceptive access initiatives have the potential to support FQHCs in meeting their clients' contraceptive needs. Organizational buy-in, sustainability of funding, and training are key to realizing the full potential of these initiatives.
Introduction
More than 7 million women at risk of unintended pregnancy obtain contraceptive services from publicly funded safety-net clinics nationwide. 1 Key to supporting the reproductive autonomy of these women is contraceptive counseling that honors their needs and preferences and access to the full range of contraceptive methods. 2
However, access to the full range of methods, including intrauterine devices (IUDs) and implants, is restricted by a multitude of barriers such as high upfront cost, 3 required return office visit for placement of the device, 4 and limitations in the number of providers who are trained and/or willing to provide IUDs and implants.5–7
Access to contraceptive methods is complex; the dimensions of health care access provide a framework to assess the interrelated components of availability (supply and demand), accessibility (location), accommodation (organization of resources), acceptability (appropriateness), and affordability (cost).8,9
Due, in part, to funding mechanisms, not all publicly funded safety-net clinics provide equal access to the full range of contraceptive methods. 10 Federally qualified health centers (FQHCs) are an essential component of the nation's health care safety-net, but not all FQHCs provide on-site contraceptive care. While federal law requires FQHCs to provide preventive and primary care, including contraceptive care, FQHCs can offer contraceptive services directly or through agreements with other providers. Also, an FQHC system may offer contraceptive care at some, but not all, of its service delivery sites.
In addition, FQHCs vary in the range of contraceptive services offered, with some offering limited services (e.g., screening and treatment for sexually transmitted infections and one or two contraceptive methods) and others offering more comprehensive care. 10 Center characteristics, the policy environment, and Title X funding influence the range of services offered.
Title X is the sole federal funding mechanism specifically allocated for the provision of contraceptive services, 11 and providers, including health departments, family planning clinics, hospitals, and some FQHCs, 12 rely on Title X funding to provide contraceptive care. 13 In South Carolina (SC), FQHCs do not receive a portion of the ∼$6 million statewide Title X funding, 14 as Title X funding is distributed through the state health department.
FQHCs that do not receive Title X funding are less likely to have on-site availability of contraceptive methods, such as stocking IUDs and implant devices,3,15 and are less likely to offer contraceptive services that require additional training, such as IUD and implant placement and removal procedures, than Title X-funded family planning clinics.16–18 Without comprehensive clinical practice guidelines and Title X funding, there is considerable variability in contraceptive service provision among FQHC clinics. 10
Despite funding limitations, the number of contraceptive care patients served by publicly funded clinics that do not receive Title X funding nationwide increased by 29% between 2010 and 2016. 1 As FQHC's role in delivering contraceptive care within the publicly funded safety-net grows, it is increasingly important to support these clinics and to examine perceptions of staff regarding facilitators and barriers to contraceptive access at their clinics.
Nationwide, federal, and state grant funding has facilitated contraceptive provision at FQHC clinics. 19 In addition, contraceptive access initiatives promise to expand access to contraceptive care at partner organizations. In SC, Choose Well is a statewide initiative, which is funded by a private philanthropic foundation, aimed at expanding access to contraception and reducing unintended pregnancy. The 6-year initiative launched in 2017 and extends into 2022. In 2017, a total of 20 FQHC systems in SC offered family planning services at 123 clinic sites across the state, and of these, 8 systems and 33 clinics participated in Choose Well. By 2018, additional FQHC systems and clinics had joined Choose Well bringing the number of participating systems to 16 and the number of participating clinics to 57.
In 2017 and 2018, participating FQHCs received funding and support through Choose Well to bolster contraceptive counseling and service provision. Participating FQHCs received capacity building and provider and administrative trainings (in the areas of contraceptive counseling, IUD and implant placement and removal, billing and coding for contraceptive services, revenue cycle, and inventory management); clinic infrastructure and workforce enhancements, including funding for contraceptive methods and staff positions, and technical assistance opportunities.20,21
As a part of the external evaluation of Choose Well, we assessed progress in implementation of the initiative at participating FQHCs during the initial 2 years with a focus on the availability of IUDs and implants. The availability dimension of access refers to components of supply and demand 22 and explores a specific area of fit between service providers and patients. 8 This construct includes providers who are trained and willing to place and remove IUDs and implants, on-site stocking of devices, administrative support for billing and coding for contraceptive services, and enhanced workflow processes. 9
The study aim was to assess changes in contraceptive access associated with the Choose Well initiative and to identify facilitators and challenges to the provision of IUDs and implants as well as perceptions of sustainability of funding from the perspective of clinical and administrative staff at Choose Well participating FQHCs. This information is important for the process evaluation of Choose Well, and more broadly, to facilitate the translation of evidence-based interventions into practice. Specifically, identifying facilitators and barriers within the availability dimension of access, at the organizational and policy/structural levels, will inform prioritizing areas for improvement within FQHC systems/clinics as well as advocacy efforts for policy change, thereby helping to optimize the impact of statewide initiatives on clinical care among FQHCs. This, in turn, will improve experiences with care and reproductive outcomes for FQHC patients.
Materials and Methods
Data collection
Semistructured key informant interviews were conducted from July 2018 to September 2019 with Choose Well participating FQHC staff at the clinic- and system-levels. FQHCs are large nonprofit organizations composed of multiple delivery sites, 23 with administrative staff working at the system/organizational level and clinic staff working to directly support or provide services at the individual delivery sites. The first round of interviews was conducted in 2018 and assessed staff perceptions of Year 1 (2017) implementation of Choose Well. In 2017, 33 FQHC clinics across 8 FQHC systems participated in Choose Well. In 2018, we invited 38 clinic-level staff (representing 32 of the 33 participating clinics; 1–3 individuals per clinic) and 11 system-level staff (representing all 8 participating systems; 1–3 individuals per system) to interview.
Of those invited, 13 clinic-level staff (34.2%) (representing 13 clinics) and 6 system-level staff (54.5%) (representing 4 systems) completed the first round of interviews.
The second round of interviews was conducted in 2019 and assessed staff perceptions of Year 2 (2018) implementation of Choose Well. In 2018, 57 clinics across 16 FQHC systems participated in Choose Well. In 2019, we invited 51 clinic-level staff (representing 39 of the 57 participating clinics; 1–3 individuals per clinic) and 21 system-level staff (representing 12 of the 16 participating systems; 1–3 individuals per system) to interview.
Of those invited, 18 clinic-level staff (35.3%) (representing 14 clinics) and 8 system-level staff (38.1%) (representing 7 systems) completed the second round of interviews. Across both rounds of interviews, 31 clinic-level interviews and 14 system-level interviews were completed. Of the 31 clinic-level interviews, 8 staff were interviewed in both rounds and counted once, generating a final sample of 23 clinic staff. Of the 14 system-level interviews, 3 staff were interviewed in both rounds and counted once, generating a final sample of 11 system staff, and a total of 34 staff at both levels over the study period (see Appendix Table A1 for details).
FQHC staff invited to interview were identified from lists provided by the Choose Well initiative and included staff engaged in or knowledgeable about Choose Well implementation at the system- or clinic-level.
At the clinic-level, we invited the clinic administrator and/or lead family planning provider (e.g., contraceptive counselor, family nurse practitioner, other nursing staff). At the system-level, we invited Executive Directors, Directors of Operations/Finance, and Chief Medical Officer/Chief Nursing Officers.
Study staff iteratively developed semistructured discussion guides, which included open- and closed-ended questions. Interview questions assessed staff perceptions of the initiative's implementation in their clinic or system. All respondents were asked the same interview questions, although wording was adapted for clinic- and system-level staff to assess implementation at the clinic- or system-level, respectively.
Respondents were recruited using a multimodal approach, which included five stages of initial and follow-up e-mails and phone calls. All interviews were conducted over the phone by study staff and audio recorded with permission of the participants. Audio recordings were transcribed by a third-party vendor. Participants received a $50 electronic gift card after completing the interview. This study was approved by the medical Institutional Review Board at East Tennessee State University.
Coding and analysis
Interview transcripts containing responses about contraceptive provision, training opportunities, and perceptions of sustainability of funding were independently coded using an iterative coding process between two coders. A codebook based on the interview guide was developed after initial review of transcripts 24 and then refined after each round of coding through consensus coding. Emergent themes were clearly defined in the codebook. 25 A minimum of 80% interrater reliability was applied for all coding. 26
This dataset contains an aggregate of 2 consecutive years of interview data. In counting responses within emergent themes, responses from each individual were counted as one total, regardless of whether an individual answered in 1 year or in both years. Themes were analyzed without regard to clinic- or system-level responses, but quotes from each level were highlighted, respectively, in data tables. The coding was conducted with NVivo 12.0 software (released in March 2018).
The availability dimension of health care access, 22 operationalized in terms of three main constructs (Availability: Clinical Factors; Availability: Administrative Factors; Sustainability of Funding) offered a framework for analysis (Fig. 1). Emergent themes influencing availability of IUDs and implants, as identified during the analysis, were mapped to these three constructs. 9
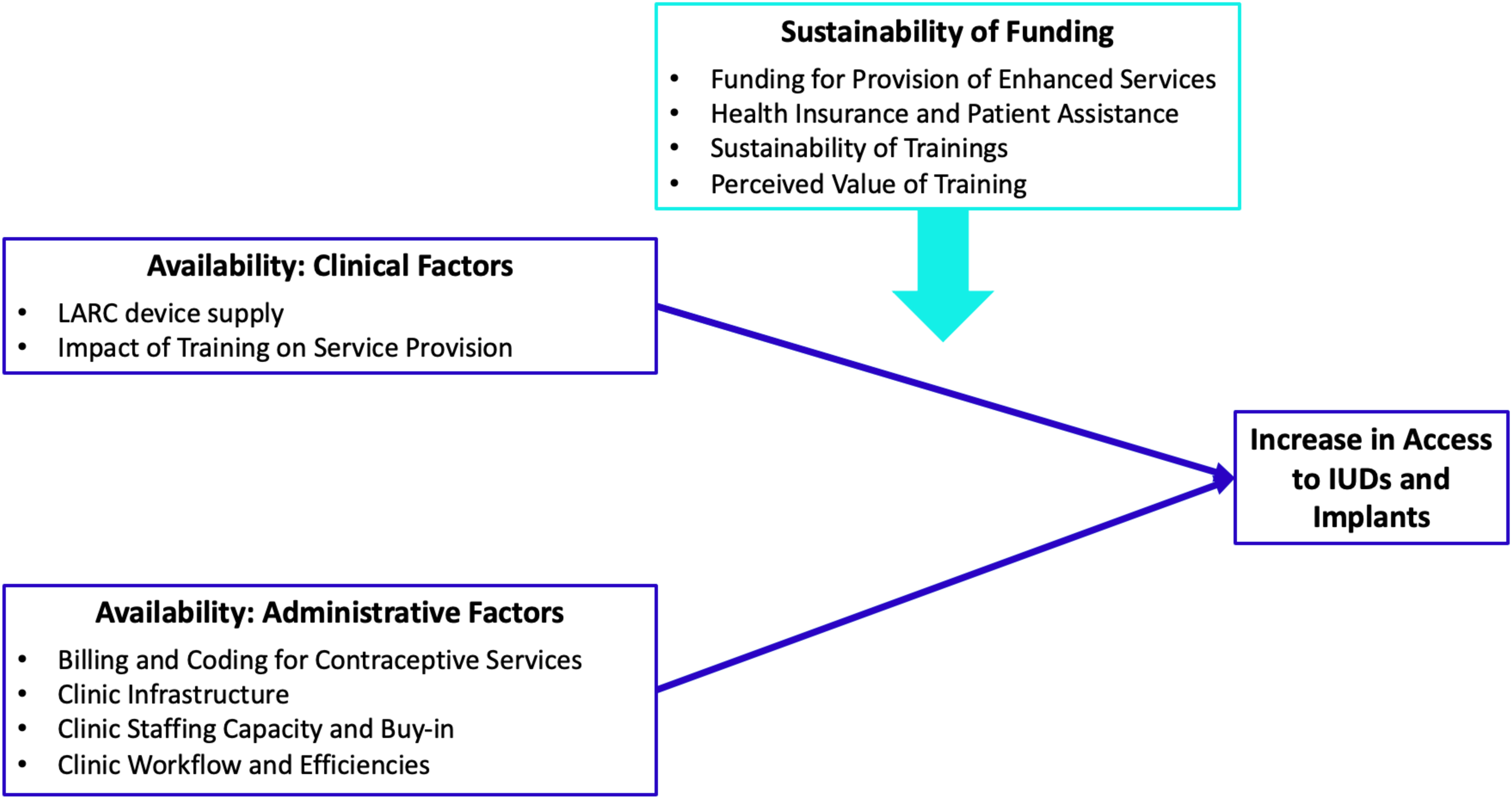
The theoretical model utilized to guide qualitative data analysis was based on the availability component of the health care access framework. Within the context of FQHC clinics and the Choose Well Evaluation, three key constructs (Availability: Clinical Factors; Availability: Administrative Factors; Sustainability of Funding) were hypothesized to influence contraceptive access. Through an inductive exploration of the interview data, emergent factors/themes impacting access were identified and then mapped to each of these three constructs. In addition, through an inductive analysis of the data, the relationships among the three constructs relative to contraceptive access were identified. Specifically, two of the three constructs (Clinical Factors and Administrative Factors) were found to directly contribute to an increase in access to implants and IUDs, whereas one construct (Sustainability of Funding) appeared to influence the identified clinical and administrative factors that impacted access. The conceptual constructs, emergent themes within constructs, and relationships relative to contraceptive access are illustrated in Figure 1. FQHC, federally qualified health center; IUDs, intrauterine devices.
The themes within clinical or administrative factors were subsequently aggregated into broader themes through a team-based data consolidation approach. 24 Representative quotations for each theme were selected to highlight perspectives of clinic- and system-level respondents.
Results
This study examined perceptions of FQHC staff regarding organizational factors, including clinical and administrative factors, which influenced access to IUDs and implants at FQHC clinics in SC during the initial 2 years of the Choose Well initiative. We also examined perceptions of sustainability, including foreseen facilitators and challenges.
Respondents
Respondents at the clinic-level held a variety of roles, including Certified Medical Assistant, Clinical Support Supervisor, Case Manager, Family Nurse Practitioner, Practice Manager, and Reproductive Health Manager. Respondents at the system-level included Chief Executive Officer, Chief Quality Officer, Clinic Operations Director, Director of Patient Services, and Project Manager.
Clinical factors
Two themes emerged related to clinical factors influencing contraceptive access at participating FQHCs during the Choose Well initiative: IUD and implant device supply; and impact of training on service provision (Table 1).
Availability—Clinical Factors
IUDs, intrauterine devices.
Discussing device supply, the majority of respondents indicated that an increase in access to IUDs and implants was facilitated by external funding, ability to provide same-day IUD and implant placement procedures, and on-site stockpiling of devices. For example, “Having that funding to be able to have the devices in-house is the biggest thing for us.”
Training opportunities provided through the initiative were noted to have enhanced and increased capacity for contraceptive counseling, increased overall clinical capacity to provide contraceptive care, and specifically increased provider capacity for IUD and implant provision. One respondent noted, “We have more providers now that can offer [IUDS and implants], can do insertions and removals of [IUDs and implants].”
In addition, half of the respondents highlighted the benefits of training for patient education and community outreach as a component of contraceptive counseling. Respondents also emphasized the benefits of an expanded perspective on reproductive health, such as “gaining viewpoints,” “becoming more open,” and “creating dialog” about contraceptive methods, sexuality, unintended pregnancy, and contraceptive counseling. Improved quality of contraceptive care services was also noted, “[Training] enhances the quality of care that the patients have been receiving… ”
However, provider factors (beliefs and comfort level) emerged as a barrier among a few respondents, for instance, the perception that some providers were “not comfortable with doing an IUD” or “have strong beliefs that's always going to be a barrier.”
Administrative factors
Four themes emerged related to administrative factors influencing contraceptive access, including the provision of IUDs and implants, during the Choose Well initiative: billing and coding for contraceptive services; clinic infrastructure; clinic staffing capacity and buy-in; and clinic workflow and efficiencies. Facilitators were identified across all themes, and barriers were identified in three domains (Table 2).
Availability—Administrative Factors
Related to billing and coding, respondents noted the importance of maximizing reimbursement and increasing revenue potential for contraceptive services. As one respondent noted, “From a revenue generation perspective, the services pay for themselves.…” While some respondents indicated that improvements in billing and coding practice at their clinic(s) had facilitated IUD and implant provision, others indicated that lack of knowledge about billing and coding was a challenge.
Regarding clinic infrastructure, robust improvement to electronic medical record or electronic health record systems was noted as a facilitator by some respondents, such as adding templates and conducting upgrades.
In discussing staff capacity and buy-in, several respondents noted that buy-in and engagement among both staff and leadership and expanded clinic workforce had facilitated access to IUDs and implants at their clinics. For example, “Our CEO is very supportive. I would think she wants to see [the program] continue and succeed.” Yet, several other respondents noted lack of buy-in to organizational change and workforce turnover as administrative barriers to increased access. Regarding a lack of buy-in: “There's some barriers still where [some providers] think that [implants] are okay, but for an adolescent, an IUD, they're not on board with. We're still working on changing some mindsets.”
Enhanced clinic workflow processes, institutionalizing changes into the current system, and tracking and utilizing clinic data were indicated as facilitators of service provision. One respondent highlighted “[reproductive health services are] part of our daily delivery now.” A few respondents, however, noted challenges to updating clinic infrastructure along with difficulties in tracking supplies and methods.
Sustainability of funding
Sustainability of funding was examined given its importance in maintaining changes associated with Choose Well implementation. This construct included four domains: funding for provision of enhanced services; health insurance and patient assistance; sustainability of trainings; and perceived value of training (Table 3).
Sustainability of Funding
FQHC, federally qualified health center.
Regarding funding, the availability of the 340B drug pricing program was noted as a facilitator of sustainability. The pricing program was noted “to provide contraceptives to clients whose insurance does not cover it.” Similarly, respondents emphasized continuing to seek other sources of external funding to provide same-visit IUD and implant provision and to order and stock devices on-site.
In addition, increasing the number of patients enrolled in Medicaid, enrolling patients in patient assistance programs, and offering a sliding scale fee for uninsured patients were all highlighted as sustaining factors to increased access. One individual at the system level noted: “You're going to get the reimbursement from the insurance companies and from Medicaid. We're trying to get everybody that will qualify on Medicaid, at least for family planning if they don't qualify for the full Medicaid.”
Plans to continue to provide staff training and to facilitate transfer of knowledge from trained staff within the FQHC system were also highlighted as sustaining factors. “For example, our providers will already be trained and as we get more providers in, those providers that have already been here and have already been trained, can be preceptors for those new providers.”
Respondents noted that expanded training opportunities are critical to increased access. One respondent emphasized, “…without the trainings we couldn't be where we are today.” Other perceptions of sustaining factors included: the applicability of training content to practice and enhanced networking among clinics.
Barriers to sustainability discussed were the high cost of devices, high rate of uninsured patients, and restrictive health care policies, such as FQHC clinics not being Title X recipients in SC, and limited insurance coverage for contraception.
Discussion
In this study, we examined perceptions of FQHC clinic- and system-level staff participating in the SC Choose Well initiative regarding organizational factors that facilitated or posed challenges to access to IUDs and implants during the first 2 years of the initiative's implementation. Staff perceptions of the early impact of the Choose Well initiative on contraceptive access at their clinics were highly positive. Staff noted how the initiative had influenced multiple clinical and administrative policies/practices related to contraceptive access. This suggests that statewide contraceptive access initiatives that remove cost barriers to care, while building the capacity of safety-net clinics to provide contraceptive services, have the potential for advancing equitable access to care.
Challenges remain, particularly related to sustaining efforts beyond the initiative's funding period and ensuring patient-centered care. On-going evaluation of Choose Well will examine the impact of the initiative at the clinic, population, and policy levels.
Findings contribute novel and relevant nuance about access to IUDs and implants among non-Title X funded safety-net clinics in SC. Notably, components of access extend beyond clinical factors, such as on-site stocking of IUDs and implants and availability of trained and willing providers, into administrative factors, such as organizational buy-in, enhanced workflow processes, electronic infrastructure enhancement, and billing and coding support.
Respondents emphasized the benefits of external funding for IUDs and implants to reduce the cost barrier to patients, consistent with previous studies. 27 In addition, themes suggest that an increase in funding for IUDs and implants contributed to clinics' ability to stock devices and provide same-visit placements, which contributed to expanded access, as noted previously.4,28–31 There are varying opinions among clinicians regarding the importance of same-visit IUD and implant placement, 32 but respondents in our study emphasized that having the financial means to stock devices and provide same-visit placement procedures positively impacted access to IUDs and implants.
In addition, increased capacity for and enhanced contraceptive counseling was noted as a primary facilitator of access to IUDs and implants, as it increased patient education and expanded perspectives, such as gaining new viewpoints, examining personal prejudices, and increasing comfort level with discussing contraceptives, among reproductive health providers.
Overall, enhanced training opportunities were perceived to have increased capacity for contraceptive service provision, consistent with previous findings among FQHC clinics. 3 Although training for IUD and implant provision is recommended for a breadth of providers, including midwives, advanced practice nurses, family medicine providers, 33 and adolescent and pediatric providers, 34 it is not always included in programs outside of Obstetrics and Gynecology specialties. 33 One sustainability strategy emerging from our interviews is the continuous provision of staff training through implementing preceptorship programs with already trained providers.
In terms of administrative factors, buy-in and engagement among staff and leadership was the most noted facilitator to increased access to IUDs and implants. Enhanced workflow processes and infrastructure support and improvements in billing and coding were similarly noted to facilitate access to IUDs and implants in our study. Enhanced interclinic networking was also emphasized.
Respondents noted challenges to increasing access to contraception in their clinics, which related primarily to lack of buy-in to organizational change among staff. The systems changes required to implement medical innovations, such as integration of contraceptive care, require administrative support and buy-in from multiple levels within the organization. 35 Optimizing the impact of statewide initiatives on clinical care among FQHCs necessitates attention to securing buy-in through on-going engagement with leadership, staff, and partnerships with other organizations to support internal influence. 35 A few respondents also noted challenges related to provider factors (comfort, beliefs).
Providers averse to offering IUDs and implants due to their beliefs and perceptions may hinder patients' access to the full range of method options, 29 suggesting the importance of on-going education and support for providers. A few respondents also mentioned workforce turnover and on-going issues with billing and coding. Incorrect billing and coding for medical services may lead to denied claims, which threaten the financial capacity for the clinic to maintain a stock of devices. 19 Coverage and reimbursement policies across insurance plans complicate billing and coding, and on-going technical assistance for clinics in this area is needed.
Considering the lack of Title X funding for FQHC clinics in SC, sustaining factors must be considered. Structural factors related to cost of contraceptive services/devices and insurance coverage emerged as prevalent challenges to sustainability. 340B drug pricing was noted as one solution. Previous research indicates variation among FQHC clinics in utilizing 340B drug pricing, with clinics that have on-site pharmacies or receive Title X funding more likely to engage with 340B drug pricing, 19 indicating opportunities for increasing clinic participation in this program.
Another suggested strategy for sustainability is facilitating patient enrollment in Medicaid. Nationwide, health centers serve about 16% of Medicaid beneficiaries, and Medicaid payments constitute nearly 40% of the revenue of FQHC clinics. 10 Beyond these approaches, our findings reinforce the need for expanded insurance coverage, particularly in states such as SC that did not expand Medicaid under the Patient Protection and Affordable Care Act (ACA), as well as for supportive reimbursement policies to increase access to the full range of contraceptive methods. 20 In addition, an important consideration for contraceptive access initiatives is ensuring patient-centered care, including best practices in contraceptive counseling that prioritize patients' needs and preferences and respect patients' reproductive autonomy.36–41
This study is not without limitation. While this study included a large number of respondents (N = 34), some members of the participant pool declined to participate, which might have contributed to potential response bias skewed toward participants eager to participate or with positive opinions about IUD and implant access. Due to the nature of qualitative research, researcher bias was a potential limitation of this study. To account for such bias, the study team was composed of a diverse group of people, and a team-based analysis approach was used. Data were double coded using an 80% or greater threshold for interrater reliability, and all differences were consensus coded.
Furthermore, as this study focused on FQHC clinics participating in the Choose Well initiative in SC, these findings may not be generalizable to other FQHCs, but rather may inform future efforts to expand contraceptive access at non-Title X clinics. The study was limited to assessing perceptions/opinions of clinic staff and did not measure clinic practices or other dimensions of access to care quantitatively or directly. On-going clinic surveys and analysis of population-level data will expand and further inform the evaluation.
Conclusion
Strengthening the family planning safety-net clinic network remains a priority at the state and national levels. Given the volatility of federal funding sources, 42 other funding mechanisms are crucial to bolster contraceptive availability among safety-net clinics that do not receive Title X funding. Statewide contraceptive access initiatives that combine funding for contraceptives with training and capacity building have the potential to support contraceptive policies and practices at FQHC clinics. By increasing access to a full range of contraceptive options and prioritizing patient-centered counseling, these initiatives could help ensure contraceptive choice and reproductive autonomy, improve health outcomes, and reduce inequities.
Based on the interview findings, the Choose Well initiative was perceived by clinic staff to have contributed to increased provision and access to contraception at participating FQHC clinics in SC through changes to clinic-level policies and practices and enhanced counseling. Staff also highlighted on-going challenges and perceived barriers to sustainability over time.
Optimizing the impact of Choose Well, and potentially of other contraceptive initiatives, requires coupling organizational change at the clinic/health system level with broader structural and policy changes to reinforce benefits of training and clinic enhancements. For example, state-level contraceptive access initiatives could advocate to strengthen health care delivery systems (through protecting contraceptive access under the ACA and restoring contraceptive access through expanded Medicaid programs) and support innovative policymaking and implementation of new delivery channels such as pharmacist prescribing.
Footnotes
Authors' Contributions
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded by a private philanthropic foundation. Grant number: 17-069.
Abbreviations Used
Appendix
Sampling Approach and Sample Sizes for South Carolina FQHC Staff Interviews by Year and Level
| FQHC systems | N | FQHC clinics | N |
|---|---|---|---|
| FQHC systems in SC that offered family planning services (2017) | 20 | FQHC clinics in SC that offered family planning services (2017) | 123 |
| FQHC systems participating in Choose Well in 2017 | 8 | FQHC clinics participating in Choose Well in 2017 | 33 |
| Of participating systems, FQHC systems invited to interview in 2018 | 8 | Of participating clinics, FQHC clinics invited to interview in 2018 | 32 |
| Of participating systems, FQHC system-level staff invited to interview in 2018 (N = 1–3 individuals per system) | 11 | Of participating clinics, FQHC clinic-level staff invited to interview in 2018 (N = 1–3 individuals per clinic) | 38 |
| Of those invited, FQHC systems interviewed in 2018 | 4 | Of those invited, FQHC clinics interviewed in 2018 | 13 |
| Of those invited, FQHC system-level staff interviewed in 2018 |
|
Of those invited, FQHC clinic-level staff interviewed in 2018 |
|
| FQHC systems | N | FQHC clinics | N |
| FQHC systems in SC that offered family planning services (2018) | 21 | FQHC clinics in SC that offered family planning services (2018) | 126 |
| FQHC systems participating in Choose Well in 2018 | 16 | FQHC clinics participating in Choose Well in 2018 | 57 |
| Of participating systems, FQHC systems invited to interview in 2019 | 12 | Of participating clinics, FQHC clinics invited to interview in 2019 | 39 |
| Of participating systems, FQHC system-level staff invited to interview in 2019 (N = 1–3 individuals per system) | 21 | Of participating clinics, FQHC clinic-level staff invited to interview in 2019 (N = 1–3 individuals per clinic) | 51 |
| Of those invited, FQHC systems interviewed in 2019 | 7 | Of those invited, FQHC clinics interviewed in 2019 | 14 |
| Of those invited, FQHC system-level staff interviewed in 2019 a |
|
Of those invited, FQHC clinic-level staff interviewed in 2019 b |
|
| Total system-level interviews in 2018 and 2019 |
|
Total clinic-level interviews in 2018 and 2019 |
|
| Final system-level staff interviews in sample a |
|
Final clinic-level staff interviews in sample b |
|
| Final no. of system-level and clinic-level staff interviews in sample 34 | |||
The bold values show 1. the number of unique individuals that were interviewed in each year of the study; 2. the total number of interviews for both years; and 3. the total number of unique interviews across both years (as some people were interviewed in both years).
N = 3 were also interviewed in 2018 and counted once in final sample.
N = 8 were also interviewed in 2018 and counted once in final sample.
SC, South Carolina.
FQHC, federally qualified health center.