
Abstract

Introduction:
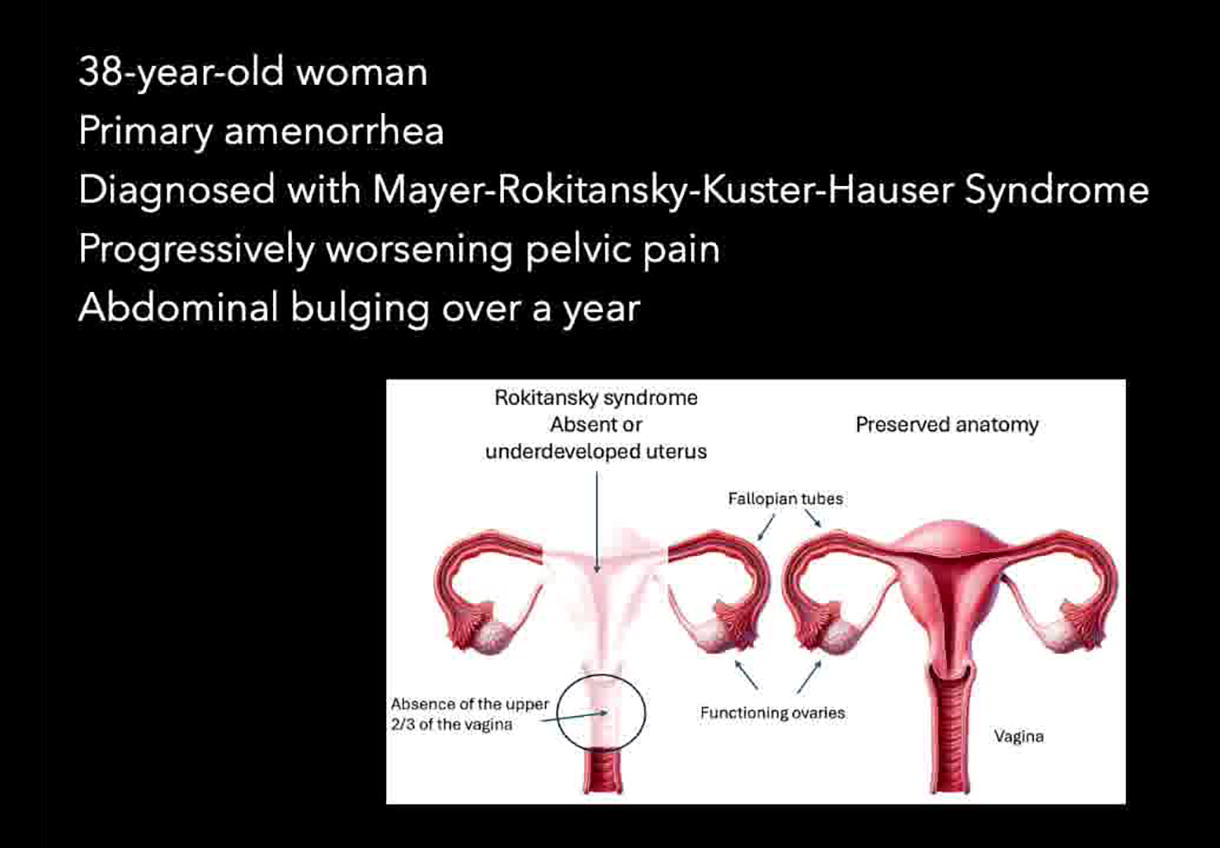
Mayer-Rokitansky-Kuster-Hauser (MRKH) syndrome is a Mullerian congenital disorder. 1 defined as agenesis or aplasia of the uterus and the upper vagina. 2 We present a case of a 38-year-old female patient with primary amenorrhea who was already diagnosed with MRKH syndrome, referring pelvic pain and abdominal bulging for one year. On her abdominal physical exam, she had palpable abdominal tumors 2 cm below the umbilicus. Pelvic magnetic resonance imaging (MRI) showed two rudimentary horns with large nodules (10 cm and 7 cm) compatible with leiomyomas; however, both with hypersignal on T2, suggesting degeneration or atypia. MRI also showed left hematosalpinx, and the CA 125 level was increased (178—reference <35). Due to the atypical imaging and increased tumor marker, we opted for the surgical removal of the rudimentary uterus along with the pelvic masses and bilateral salpingo-oophorectomy. The pathology report confirmed the diagnosis of uterine leiomyomatosis and tubal endometriosis with no malignancy or atypia.
Participants:
A 38-year-old female patient.
Objective:
To show the diagnosis and surgical management of large leiomyomas in a patient with MRKH syndrome via laparoscopic robot-assisted approach.
Materials and Methods:
Interventions Laparoscopic robotic-assisted approach. Cavity inventory: Both uterine horns were identified, and the masses were macroscopically compatible with typical fibroids. There was also hematosalpinx on the left tube. There was no cervix, and horns were attached to a rudimentary uterine midline cord. Adhesion lysis, salpingo-oophorectomy, hysterectomy of the rudimentary uterus along with the myomas. Surgical specimen removal: manual morcellation was performed inside a protection bag.
Results:
The surgery lasted 2 hours, and there was minimal bleeding. An anatomopathological study reported all specimens as benign, typical leiomyomas in both rudimentary uterus and tubal endometriosis.
Conclusion:
Mullerian malformations can be a challenging condition for gynecologists in both diagnosis and surgical treatment, when needed. In those cases, careful diagnostic investigation must be enforced, and the surgical intervention must be meticulously planned.
The author declares that she has no conflict of interest.
IRB approved:
“The patient(s) included in this video gave consent for publication of the video and posting of the video online, including social media, the journal website, scientific literature websites (such as PubMed, ScienceDirect, Scopus) and other applicable sites.”
Runtime of video:
7 mins 26 secs.
Get full access to this article
View all access options for this article.