
Abstract

Introduction:
Patients who undergo abdominal wall reconstruction (AWR) with mesh remain at risk for subsequent abdominal surgeries. 1,2 The presence of mesh complicates the surgical approach in these patients when attempting to preserve the integrity of the mesh. Laparoscopic approaches can be tailored to patients with large pieces of planar mesh after AWR to reduce hernia recurrence, which may occur when the previously placed mesh is violated. This video case report illustrates the preoperative planning and operative approach to treat a small bowel obstruction (SBO) after AWR.
Materials and Methods:
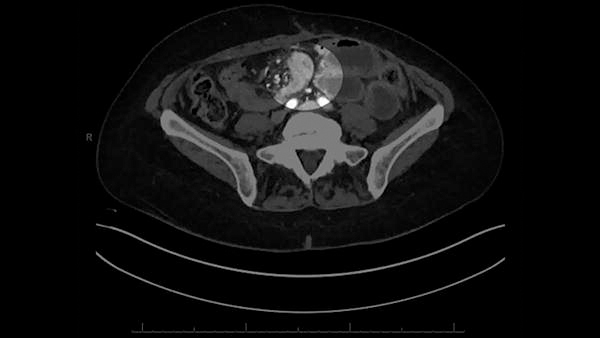
A patient who underwent prior AWR with the placement of a large piece of permanent synthetic mesh in the retromuscular space developed a small bowel obstruction (SBO). The review of prior operative reports and preoperative imaging revealed a 30 cm by 30 cm piece of retromuscular mesh spanning the right rectus muscle to the left hemiabdomen. A second piece of mesh measuring 13 cm by 11 cm was described as bridging a defect in the left rectus muscle. Laparoscopic ports were placed lateral to the right semilunar line to avoid the right side of the mesh. Two additional ports were successfully placed lateral to the right semilunar line under direct visualization. The previously placed mesh was easily visualized laparoscopically, with no evidence of hernia recurrence. A complete lysis of adhesions was performed, and the patient recovered postoperatively and was discharged home. A few months later, the patient presented with a recurrence of SBO and was taken back to the operating room for further exploration. Utilizing the same port configuration, laparoscopic access was obtained without violating the previously placed mesh. The previously placed mesh was intact, with no evidence of hernia recurrence. A complete lysis of adhesions was performed again, and the patient recovered uneventfully.
Results:
Although the patient developed a recurrent SBO, laparoscopic lysis of adhesions was successfully completed on both occasions without compromising the previously placed permanent synthetic mesh.
Conclusion:
We emphasize the importance of reviewing preoperative imaging and prior operative reports to gain a comprehensive understanding of a patient’s anatomy and the location of any synthetic implants prior to operative intervention. We demonstrate that it is sometimes possible to perform laparoscopic surgery and avoid port placement through previously placed retromuscular permanent synthetic mesh, which may reduce future hernia recurrence.
Runtime of video:
7 mins 00 secs.
Get full access to this article
View all access options for this article.