
Abstract


Introduction:
Isolated tracheoesophageal fistula (H-type TEF) is a rare congenital anomaly characterized by a direct connection between the esophagus and trachea without esophageal atresia (EA), representing only 4–5% of congenital EA/TEF cases. Prompt treatment of a TEF is important for preventing aspiration. Children affected by EA/TEF frequently present with other anomalies in the VACTERL spectrum, introducing additional management challenges. We present a novel case of an infant with H-type TEF, tetralogy of Fallot (ToF), and a vascular ring.
Materials and Methods:
An 8-day-old male born at term, small for gestational age (3rd percentile, 2.5 kg) with prenatally diagnosed ToF presented with desaturation episodes after feeding, raising concern for aspiration. Maternal history was notable for hypothyroidism treated with levothyroxine and hepatitis C antibody positivity with an undetectable viral load. The infant had peripheral acrocyanosis and oxygen desaturation at birth and was placed on nasal continuous positive airway pressure. He was weaned to room air on the same day.
Results:
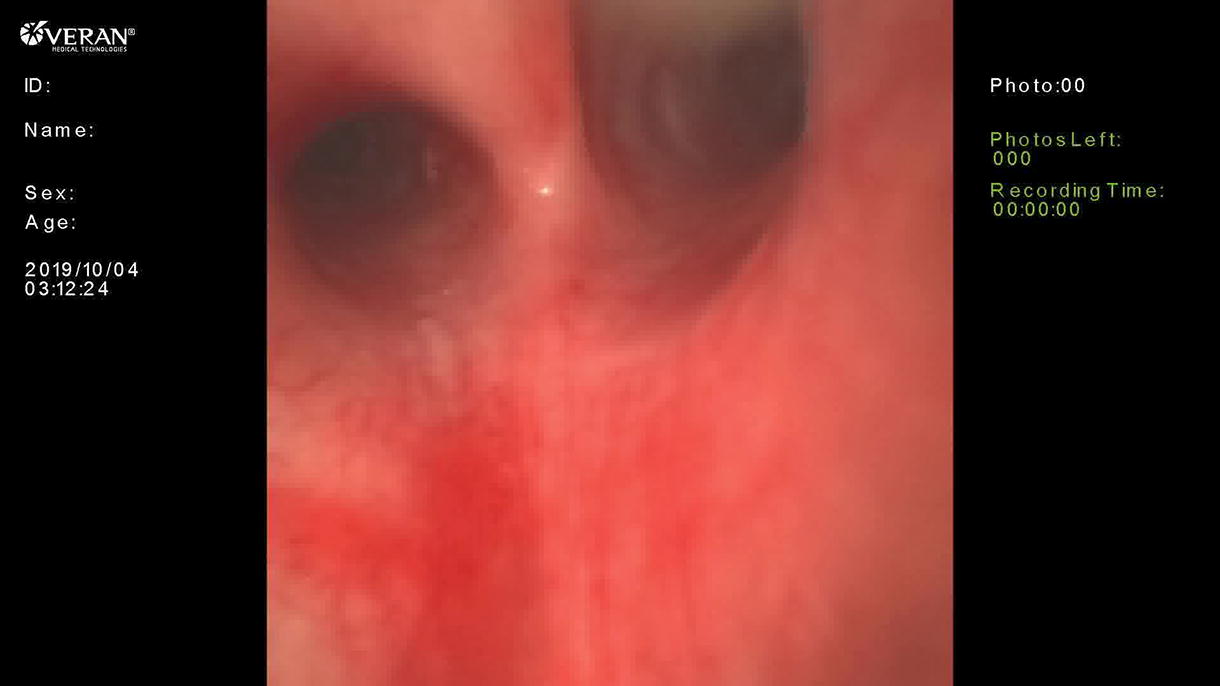
Modified barium swallow suggested an H-type TEF, and an echocardiogram demonstrated ToF with a large anterior malalignment conoventricular septal defect, right ventricular hypertrophy, and a small left-sided patent ductus arteriosus (PDA) with bidirectional flow. Pulmonary hypertension was detected through PDA and pulmonary artery spectral Doppler profiles. Preoperative imaging also revealed a vascular ring consisting of a right aortic arch with an aberrant left subclavian artery and ductal ligament. Diagnostic laryngoscopy identified a type I laryngeal cleft. Rigid tracheobronchoscopy confirmed a mid-tracheal TEF and no tracheomalacia. Flexible upper endoscopy showed the TEF with an otherwise normal esophagus. The patient underwent an uncomplicated combined repair of the TEF and vascular ring through a left posterior muscle-sparing thoracotomy. The ductal ligament was divided. The aberrant left subclavian artery was divided and reimplanted onto the left common carotid artery. The H-type TEF was divided and repaired with a transverse tracheoplasty and a Heineke–Mikulicz esophageal repair. The esophageal repair had minimal tension and good tissue quality. Indocyanine green perfusion assessment revealed excellent tissue perfusion. Leak test showed no air leakage from the tracheal repair nor the esophageal repair. There was good preservation of the esophageal lumen on flexible endoscopy. A descending aortopexy, posterior tracheopexy, and rotational esophagoplasty were performed to offset suture lines and minimize the risk of recurrent fistulization. The recurrent laryngeal nerve was monitored during the operation with dual-channel electrodes adhered to the endotracheal tube. Nerve signals were intact at the end of the operation. The child recovered well and awaits repair of his ToF.
Conclusions:
This is the first case reported of the surgical treatment of a type H tracheoesophageal fistula and vascular ring in an infant with tetralogy of Fallot, highlighting the complexities in the management of patients with TEF. The successful surgical management outlined in this report emphasizes the benefits of a multidisciplinary approach, thorough preoperative imaging and endoscopic evaluation, and concomitant repair of coexisting intrathoracic pathology.
Patient consent statement:
Consent was obtained for the publication of this case report. Author(s) have received and archived patient consent for video recording/publication in advance of video recording of the procedure.
Source of work:
Clinical practice.
Disclosures:
The authors of this article have no conflicts of interest to disclose.
Runtime of video:
7 mins 29 secs
Get full access to this article
View all access options for this article.