
Abstract
Introduction:
Situs inversus totalis is a rare condition characterized by mirror image transposition of organs. 1 The literature reports its occurrence as 1:10,000 with a slightly more frequent occurrence in men, 1.5:1. 1 Patients with this condition can pose a clinical challenge as it is rarely encountered and the anatomy is located in unfamiliar locations. 2 In addition, most minimally invasive procedures may require surgeons to use their nondominant hand for dissection. One study documents only 31 patients with situs inversus undergoing cholecystectomies in the nearly 15 years since the first documented patient underwent this procedure. 3 They noted a general longer operating time, as well as increased probability for biliary and vascular anatomy anomalies. 4 Even with these considerations, the rates of morbidity or mortality compared with the general population were not higher. 4
Case Presentation:
A 40-year-old woman was referred to general surgery clinic for a history of biliary cholic. She reports years of episodic pain with associated nausea vomiting. Her medical history was significant for situs inversus totalis. Preoperative imaging included computed tomography and ultrasound images that confirmed situs inversus as well as cholelithiasis without evidence of cholecystitis.
Materials and Methods:
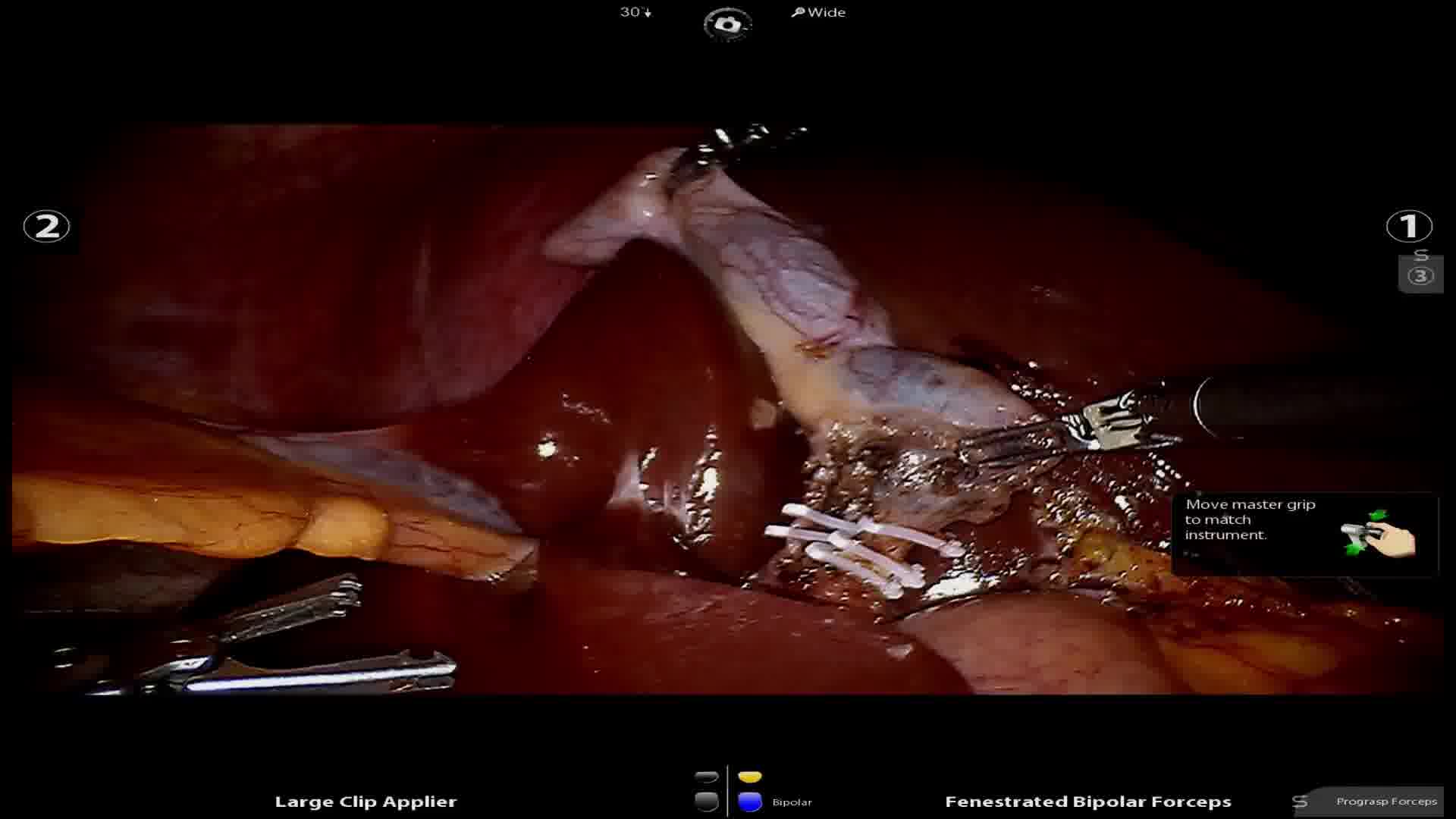
The patient underwent general anesthesia and both arms were tucked. The abdomen was entered using a Veress needle and 12 mm Optiview trocar. Once the abdomen was insufflated, three more ports were placed each 8–10 cm apart in a semicircular manner along the left lower abdomen. The gallbladder was visualized and retracted cephalad using robotic grasper. Next, using a combination of hook cautery and a grasper, the cystic duct and artery were skeletonized. Indocyanine green fluorescent imaging was used to confirm biliary anatomy. The hepatocystic triangle was cleared of fat and the lower third of the gallbladder was separated from the liver. Once the critical view was achieved, a robotic clip applier was used to apply three clips to the cystic duct and artery, respectively. The duct and artery were then cut, and the gallbladder was dissected from the liver bed using electrocautery.
Results:
Total operative time was 221 minutes with an estimated blood loss of 5 mL. There were no complications, and the patient was discharged the same day of surgery. During the patient's follow-up visit 2 weeks later, she was tolerating diet, with excellent pain control and no complaints.
Conclusion:
Situs inversus totalis can pose unique clinical challenges to surgeons. The robotic platform can help mitigate some of the challenges this condition presents. Given its rarity, when clinicians encounter patients with this condition, extensive preoperative planning is recommended to adequately prepare for the procedure. To our knowledge, this is the only case report using the robotic platform for cholecystectomy in a patient with situs inversus. Previous case series have demonstrated advantages using the robotic platform in this patient population because of augmented observation, and the ability to use bimanual dexterity. 5 The robotic platform has been reported for the use of oncologic resections in patients with situs inversus with gastric cancer, rectal cancer, and those with large hiatal hernias. 5 Finally, patients with situs inversus did not have higher rates of morbidity or mortality than the general public. 4
Acknowledgment:
The authors thank Christina Monaco DO for her contributions to this project.
Patient Consent Statement:
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
No competing financial interests exist.
Runtime of video: 8 mins 25 secs

Get full access to this article
View all access options for this article.