
Abstract
Introduction:
Intrathoracic leak rates associated with Ivor Lewis esophagectomies range from 3% to 12%. 1 These anastomotic leaks have been treated with multiple techniques, including both surgical and endoscopic methods. 2 Surgical methods include percutaneous or operative drainage, as well as primary surgical repair. 3 Endoscopic methods include stenting, clips such as Ovesco, which is an over the endoscope metal clip used for approximating soft tissue, and suturing systems. 4,5 Some endoscopic techniques may be challenging in areas that are not amenable to the equipment that must be used, such as larger or abnormally shaped defects as is evident in this case.
Materials and Methods:
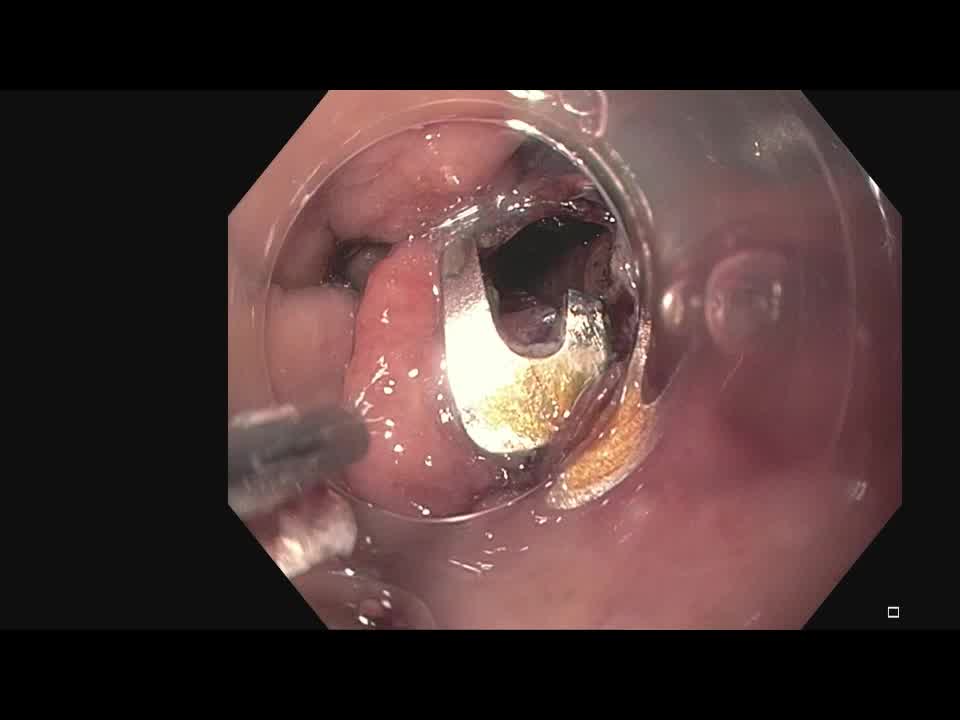
This is a 72-year-old man with a past medical history significant for esophageal adenocarcinoma status post-Ivor-Lewis esophagectomy. He presented 2 months postoperative with increasing nausea, vomiting, cough with increased sputum production, and weight loss. A swallow study was completed, which showed contrast opacification of right lower lobe segmental and subsegmental airways that was suggestive of a gastrobronchial fistula. He was taken to the Operating Room for endoscopic management later that month, which revealed breakdown of the staple line. The fistula was initially treated with a 12/6 GC Ovesco clip and subsequent carbon dioxide insufflation was read at 40 mm Hg, thus suggesting that the defect was closed. There were no immediate operative or postoperative complications. However, 1 month postoperatively, the patient had a follow-up swallow study completed that showed a persistent gastrobronchial fistula. The patient underwent a repeat Esophagogastroduodenoscopy with removal of the Ovesco clip and utilization of the X-tack system, which is a through the endoscope, helical tacking system. Because of increased maneuverability, two separate four bite X-tack systems were used to run the suture line along the area of the previously identified fistula. Each tack was placed independently in a “Z” pattern before the 3-0 polypropylene suture was pulled tight to approximate the soft tissue surrounding the defect. 6 Both X-tack systems were observed for proper placement and closure of the defect.
Results:
The patient had two subsequent swallow studies completed, 2 months apart, which showed effective closure of the gastrobronchial fistula. He was doing well at his follow-up appointment 2 months postoperatively, with only mild dysphagia.
Conclusion:
X-tack has proven to be a safe, feasible, and effective modality for closing a gastrobronchial fistula. This case demonstrates the importance of a staged endoscopic intervention in the case that one device fails, as was evident with the Ovesco clip failure and subsequent X-tack utilization. Finally, this case highlights the benefits of multidisciplinary care that saved this patient from a more morbid surgical intervention. To date, the X-tack system has been utilized in 14 patients in our surgical endoscopy group with varying degrees of long-term success.
T.E., A.H., and M.D.T. have no financial disclosures. E.M.P: Speaking/teaching: Bard Davol, Medtronic, Ovesco; Consultant: Boston Scientific Corp., Actuated Biomedical Inc., Baxter, Cook Biotech, Neptune Medical, Surgimatrix, CMR surgical, Boehringer Laboratories, Allergan; Royalties: UpToDate Inc., Springer; Financial Interests: IHC, Inc., Contamination Source Identification, SIG Biomedical.
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
The source of the study is the Penn State Milton S. Hershey Medical Center: surgical endoscopy group.
Runtime of video: 5 mins 54 secs
This video was presented as a video presentation at the 2022 Society of Gastrointestinal and Endoscopic Surgery on March 17, 2022.


Get full access to this article
View all access options for this article.