
Abstract
Introduction:
Benign esophageal tumors are relatively uncommon, with a prevalence rate of 0.5%. 1 More than two-thirds account for leiomyomas, which are submucosal located and originate from smooth muscular fibers. Small esophageal leiomyomas under surveillance usually have a benign natural history, with most cases being asymptomatic. 2 Surgical resection is warranted for larger masses (>5 cm) and symptomatic cases. 1,2 Enucleation is the treatment of choice, preferably through minimally invasive approaches. Although thoracoscopy is generally performed to treat upper-middle third esophageal leiomyomas, laparoscopic transhiatal enucleation can be an alternative for tumors in the distal third or near the gastroesophageal junction. 2 This video presents an effective laparoscopic transhiatal resection of a large esophageal leiomyoma of the lower esophagus with intraoperative endoscopy.
Materials and Methods:
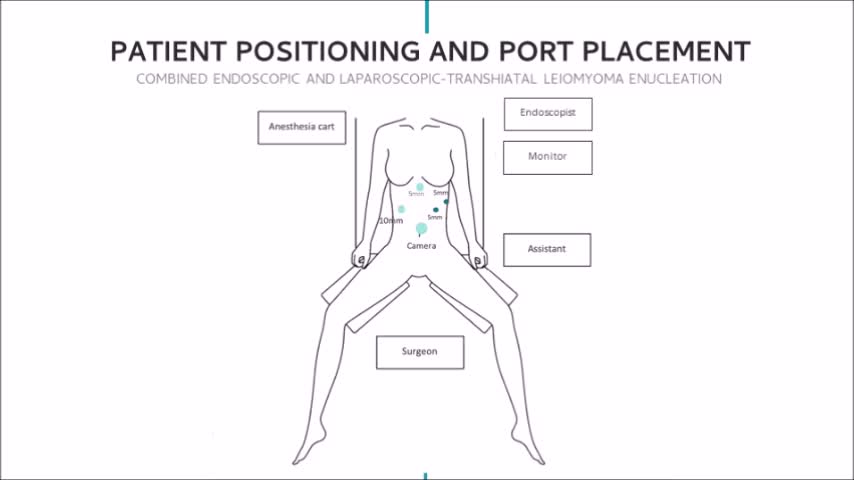
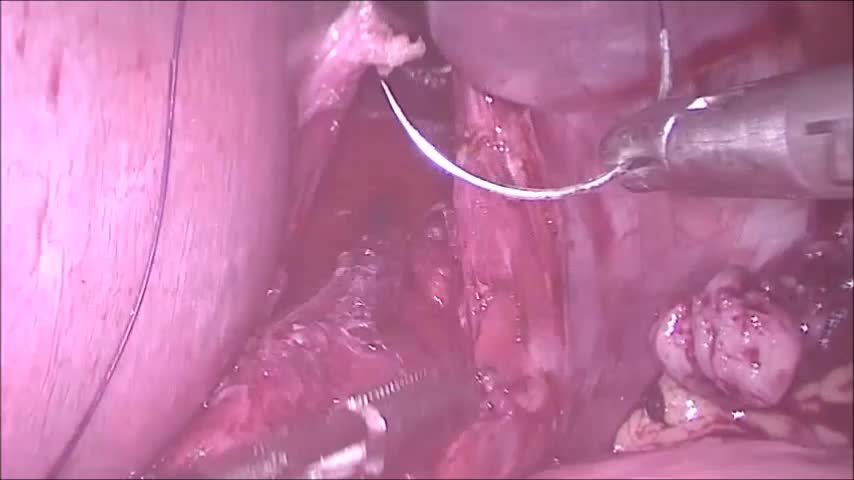
A 17-year-old female patient with a history of quiescent celiac disease presented with persistent dyspeptic symptoms. Esophagogastroduodenoscopy revealed a protruding submucosal smooth mass in the lower third of the esophagus located 6 mm from the cardia. CT scan confirmed the diagnosis of a circumscribed soft tissue opacity with homogeneous density measuring 3.2 × 6.3 × 3.2 cm, suggestive of esophageal leiomyoma. In view of the patient's symptoms and tumor location, enucleation by a combined endoscopic and laparoscopic transhiatal approach with gastric fundoplication was planned. After dissection and mobilization of the proximal stomach and lower esophagus, transillumination under intraoperative endoscopy guided the identification of the tumor. The esophageal muscular layer was longitudinally incised along the whole length of the tumor to enable its enucleation. Mucosal integrity was confirmed with air inflation under intraoperative endoscopy. The myotomy was closed using continuous slowly absorbable sutures and a 90° anterior fundoplication was performed. The patient was allowed liquids on day 1. She was discharged on the 5th postoperative day after an uneventful recovery. She has been followed up for 1 year with complete symptom resolution. Histopathology examination was consistent with benign leiomyoma and no atypia was detected.
Results and Conclusion:
Esophageal leiomyomas are typically located within the lower two-thirds of the esophageal wall. 1 The laparoscopic transhiatal enucleation for tumors located up to 5 cm from the hiatus provides better exposure and access to the tumor and has the advantage of allowing concomitant antireflux repair by crural repair and fundoplication. 3,4 A hybrid approach with intraoperative endoscopy further increases safety as it facilitates identification of the dissecting plane thus limiting myotomy, and also provides control for mucosal integrity. 3 Muscle layer approximation after the myotomy is recommended to prevent loss of peristalsis, mucosal bulging, and pseudodiverticulum formation, which could lead to dysphagia. 1,5 In the described case, the suture line was also protected by the gastric flap of the 90° anterior fundoplication, which combined with the hiatal closure contributed to reducing the patient's gastroesophageal reflux symptoms. The literature reports excellent long-term results with minimally invasive approaches, and surgical recurrence is rare. 2,5 Postoperative follow-up usually consists of clinical assessment of symptom resolution, though some authors advocate objective functional analysis by esophageal manometry and pH monitoring. 1 In conclusion, this report describes an effective resection of a leiomyoma of the lower esophagus by a combined method of laparoscopic transhiatal and intraoperative endoscopy, which represents a safe and effective approach for esophageal benign masses.
Dr. Leandro Totti Cavazzola is a proctor for Intuitive Surgical, Inc. The other authors do not have conflicts of interest to disclose.
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Runtime of video: 5 mins 45 secs

Get full access to this article
View all access options for this article.