
Abstract
Introduction:
Laparoscopic repair for incisional hernias was described initially in the early 1990s. 1 The procedure involves an intraperitoneal mesh placement to achieve a tension-free repair of the hernia. However, in recent years, there has been great concern about long-term complications related to the intraperitoneal mesh placement. Many case reports and case series have found evidence of mesh adhesion, bowel fistulae, shrinking, and migration resulting in various minor and major acute abdominal complications. 2 After these concerns, in the past years, many new techniques have been developed, alongside the most traditional ones, such as Rives Stoppa. 3,4 These new procedures such as the MILOS, the ELAR, the TESAR, and the REPA 5 –8 aim to treat incisional hernias in an extraperitoneal way. Our group has recently published a new and innovative technique, the THT (named from our regional surgical group, the Trentino Hernia Team), which aims to reconstruct the abdominal wall midline endoscopically with a linear stapler through a single umbilical access. 9 The advantages of this procedure consist mainly in its simplicity of execution and speed (1 hour), its high reproducibility, the extraperitoneal approach (with the only exception of a 5 mm trocar), and the sublay mesh positioning with a significant decrease in costs compared with the traditional Intraperitoneal Onlay Mesh approach. 10
Patient Selection and Work-Up:
The patient depicted in the video was urgently admitted to our department for strangulation of a voluminous recurrent incisional umbilical hernia. The patient was 53 years old, with a body mass index of 33. He had undergone previous laparoscopic cholecystectomy in 2016 for cholelithiasis and a direct suture of an umbilical trocar site incisional hernia in 2017. At admission, a CT scan revealed a defect of 6 × 8 cm (M3 L6 W2 according to European Hernia Society classification) 11,12 with a synchronous epigastric hernia of 2 cm and a diastasis of 8 cm width and 18 cm of longitudinal extension. Informed consent was obtained and he was furthermore informed about the THT procedure and the possibility of a transversus abdominis release (TAR) procedure in case of excessive tension along the median suture.
Preoperative Preparation:
The surgery was conducted under general anesthesia. A single dose of a short-term antibiotic (cefazolin 2 g i.v.) 13 was administered before the operation.
Equipment Preference Card:
The patient was positioned on the operating table with the right arm open, the left one closed, and split legs. The first operator stood between his legs, the second operator on the patient's left side, and the nurse between the surgeons. Two monitors were used, one positioned behind the right shoulder of the patient, the second one behind his right leg.
Methods:
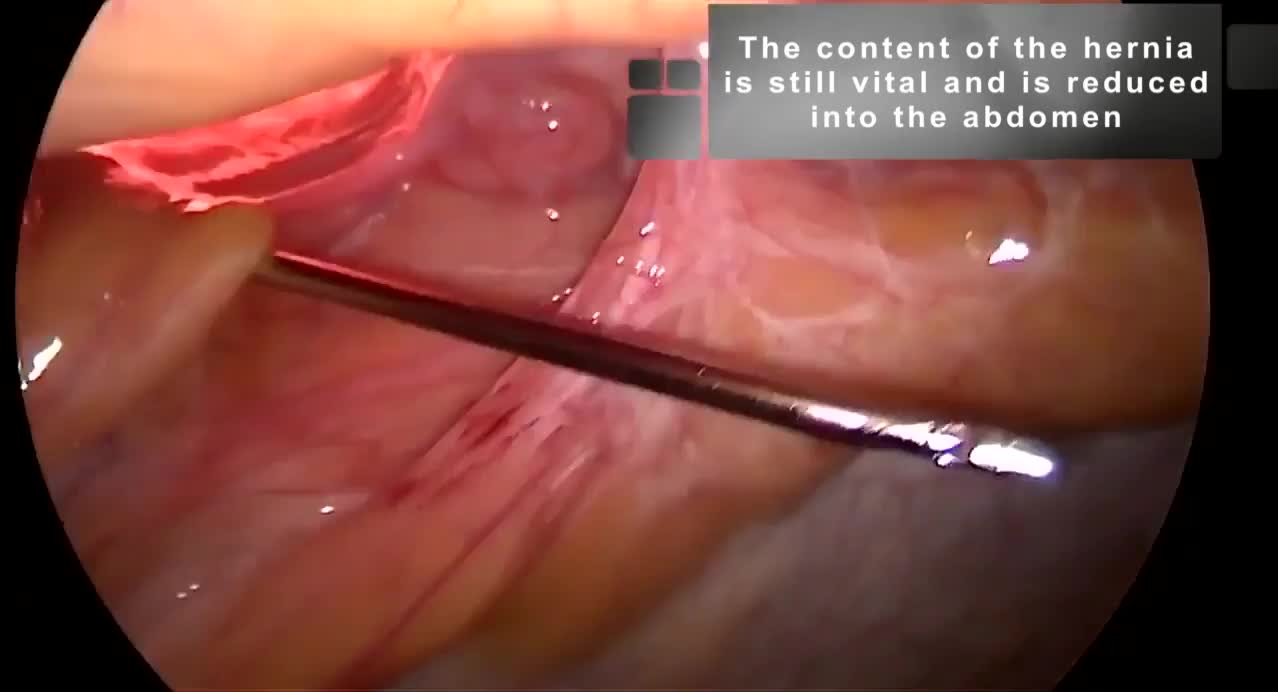
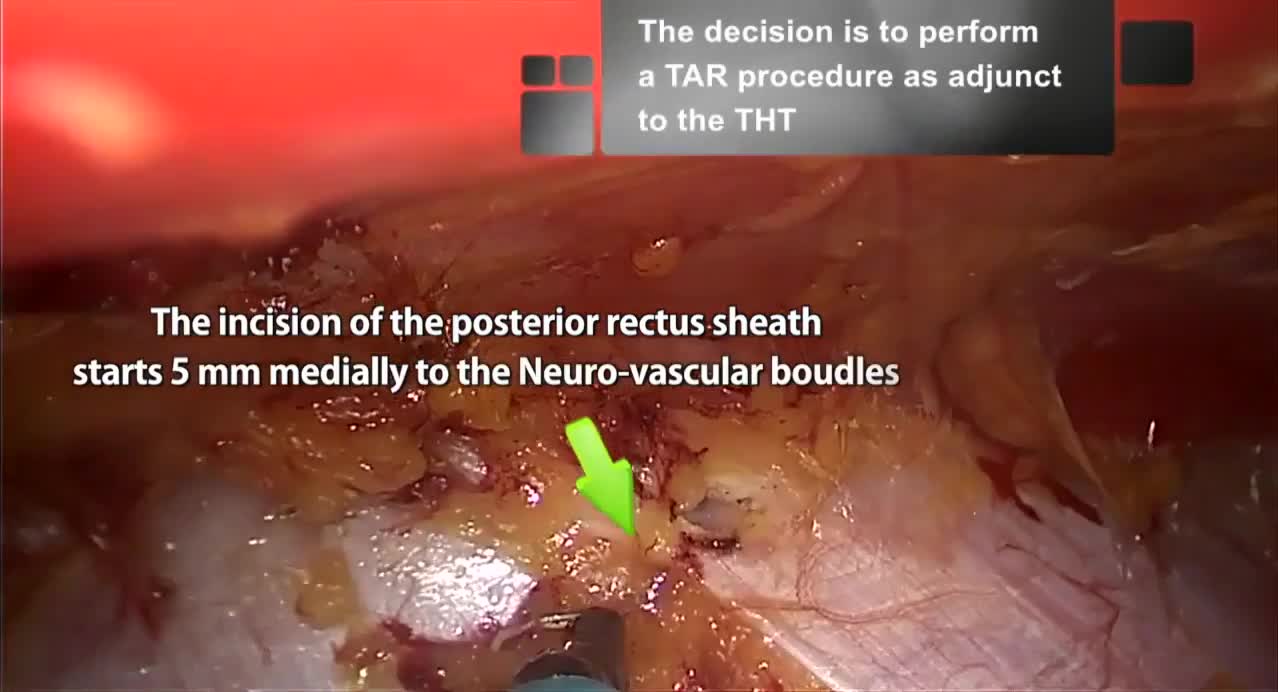
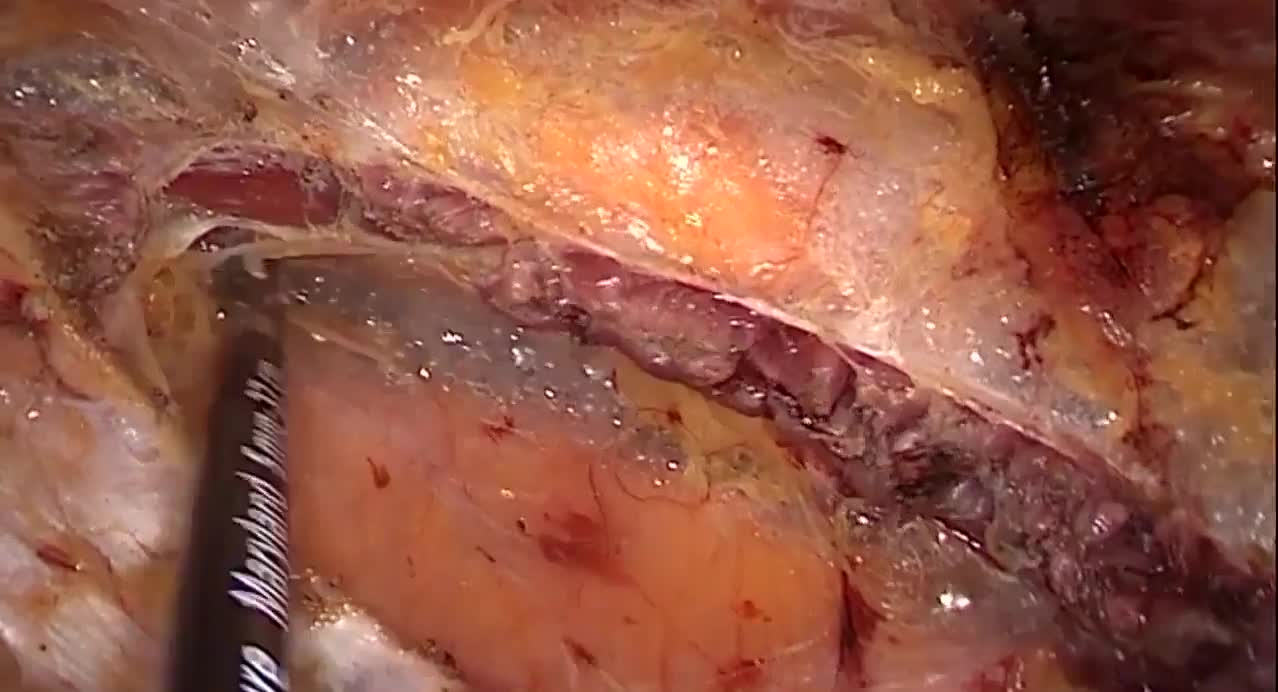
First, through a 4 cm periumbilical incision, the umbilicus was disconnected from the fascial plane. The voluminous hernia sac was dissected and opened to verify its content. A portion of necrotic strangulated omentum was resected with Ligasure™ (Medtronic). No ischemic intestinal portions were found inside the hernia. The hernia sac was subsequently resected and the peritoneum closed with an interrupted suture. A Veress needle was positioned through the suture to inflate a pneumoperitoneum of 12 mm Hg. One 10 mm trocar was placed in the patient's left side to have a direct visual check of the peritoneal cavity and the viability of the hernia sac contents. The rectus sheaths were isolated and incised to enter the retromuscular space on both sides. The two branches of a linear stapler were inserted into the two rectus sheaths; because of the patient's tissues thickness (in particular, the posterior rectus sheets), 4.0–5.0 mm linear stapler (EndoGIA™ 60 mm black reload with Tri-Staple™ technology; Medtronic) was used. Two EndoGIA reloads were used to suture the two rectus sheaths first toward the sternum and then toward the pubis, to create a wide retromuscular space. A single-port device (GelPOINT® mini; Applied Medical) was then introduced through the umbilical incision inside the neo-formed retromuscular space. The retromuscular space was then dissected on both sides using a monopolar hook until reaching the costal margins cranially, the arcuate line caudally, and the rectus neurovascular bundles laterally. Three other reloads of EndoGIA 60 mm were used to endoscopically complete the suture of the rectus sheaths from the xiphoid to the Retzius space. Because of the presence of high tension on the midline suture and to the high risk of recurrence associated with the patient's obesity, it was decided to perform a totally endoscopic TAR as an adjunct to the THT technique. Starting from a distance of 5 mm from the origin of the neurovascular peduncles, the posterior rectus sheaths were incised preserving the peritoneum and, as much as possible, the transversalis fascia. The incision was extended to the arcuate line caudally and the costal margin cranially. The transversus muscles were dissected with a high-energy device (Ligasure) creating a wide space between the transverse muscle and the transversalis fascia where the mesh was positioned. At this point, 8 cm per side were gained, allowing a reduction of the tension along the midline. After the measurement of length and width (30 × 27 cm) of the neo-formed retromuscular plane, a macroporous light-weight mesh (Softmesh, Bard) was tailored and positioned endoscopically through the umbilical access. After the removal of the GelPOINT Mini, the two rectus abdominis were joined together using absorbable stitches. The same stitches were also used to transversally suture the margins of the anterior rectus sheaths. A polydioxanone suture was used to reattach the umbilicus to the fascial plane. The cutaneous wounds were closed with intradermal stitches and cyanoacrylate.
Results:
In the first postoperative 24 hours, the analgesic therapy was set as follows: paracetamol 1 g i.v. every 8 hours, ketoprofen 160 mg i.v. as rescue. The patient was discharged on postoperative day (POD) 2. Antithrombotic prophylaxis (low-weight heparin 4000 UI every 24 hours) was continued for 12 days after. At the follow-up visit on POD 7, a superficial infection (SSI) on the umbilical incision was diagnosed. The infection was limited at the subcutaneous layer on the left margin of the wound. Fifteen days later, the wound appeared to be fully recovered. After 3 months, neither major nor minor complications had been reported. Follow-up at 18 months is free from recurrences.
Conclusions:
The THT technique associated with TAR represents a feasible and effective treatment for incisional hernias. At present, this technique has been used in eight cases with a short length of hospital stay (2 days) and a fast return to normal activities of daily living (2–4 weeks) along with an excellent quality of life. Except for the SSI of this patient, no other major or minor complications have been reported. In a mean follow-up of 12 months, no recurrences were reported. Nevertheless, more studies are necessary to confirm these preliminary results.
Runtime of video: 10 mins
Get full access to this article
View all access options for this article.