
Abstract
Introduction:
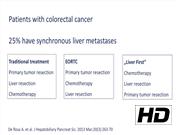
Minimally invasive techniques have been adopted as the standard of care in specialized centers for hepatobiliary surgery. Laparoscopic extended major hepatectomies (LEMH) is a technically demanding and challenging procedure. However, outcome data for LEMH in terms of morbidity and mortality appear to be comparable with laparoscopic major hepatectomies (LMH). 1 At this time, several studies comparing LMH with open major liver resections report lower rates of pulmonary complications, 2 less blood loss, and shorter hospital stay, 3,4 without compromising oncological resection. 5 –7 This video reports a laparoscopic extended right liver resection. 8,9 Approximately 25% of patients with colorectal cancer have synchronous liver metastases at the time of diagnosis. The traditional treatment approach is resection of the primary tumor followed by liver resection if possible. Chemotherapy was mainly performed in an adjuvant treatment protocol or following the European Organisation for Research and Treatment of Cancer (EORTC) trail in a neoadjuvant setting before liver resection. Recently a “liver first” approach especially for patients with a high metastatic liver tumor burden has been advocated. In this approach, as described in our video, liver resection is performed in a first step usually after a period of down staging chemotherapy. In a second step the primary tumor gets resected. The rationale behind this approach is to optimize the chance of potentially curative liver resection, which might have an impact on long-term survival.
Materials and Methods:
After obtaining a pneumoperitoneum, total vascular inflow control by a Pringle maneuver was obtained. As a precaution the hepatoduodenal ligament is looped with an extracorporal accessible tourniquet. Inflow control was obtained next by dividing the right portal and hepatic arteries using clips and ties. A demarcation line of ischemia was discerned, and intraoperative ultrasonography confirmed the location of the metastatic lesions. The parenchymal transection was performed using ultrasonic scissors, laparoscopic Cavitron Ultrasonic Surgical Aspirator, and stapling devices. Furthermore, the intracorporeal hanging maneuver was applied during the liver resection. 10 The specimen was retrieved through a Pfannenstiel incision.
Results:
Operative time was 5 hours 40 minutes with an estimated blood loss of <200 mL and no transfusions were required. The patient remained in the ICU for 24 hours and was discharged home on postoperative day 8. Laparoscopic resection of the primary rectal cancer was performed 24 days post liver surgery. Again, the patient had an uneventful course and was discharged 10 days postsurgery. All resections were histologically graded R0. The patient is disease free at 3 months postoperatively.
Discussion:
Approximately 25% of patients with colorectal cancer have synchronous liver metastases at the time of diagnosis. The traditional treatment approach is resection of the primary tumor followed by liver resection if possible. Chemotherapy was mainly performed in an adjuvant treatment protocol or following the EORTC trail in a neoadjuvant setting before liver resection. Recently a “liver first” approach especially for patients with a high metastatic liver tumor burden has been advocated. In this approach, as described in the video, liver resection is performed in a first step usually after a period of down staging with chemotherapy. In a second step the primary tumor is resected. The rationale behind this approach is to optimize the chance of potentially curative liver resection, which might have an impact on long-term survival. The long-term results need to be ascertained before making this protocol the standard of care.
No competing financial interests exist.
Runtime of video: 8 mins 11 secs


Get full access to this article
View all access options for this article.