
Abstract
Introduction:
Intraductal papillary mucinous neoplasm (IPMN) is a disease process normally found in pancreatic ducts, and very rarely is this seen isolated to the intrahepatic ducts. Biliary duct IPMNs (BT-IPMNs) are the biliary equivalents of IPMNs of the pancreas. They are premalignant lesions found in the biliary tree that produce mucin and present with papillary frond-like lesions that can be seen on cholangioscopy. It is believed that they can progress into cholangiocarcinoma. This is the case of a patient presenting with IPMN extending from the extrapancreatic common bile duct to the right hepatic duct.
Case Report:
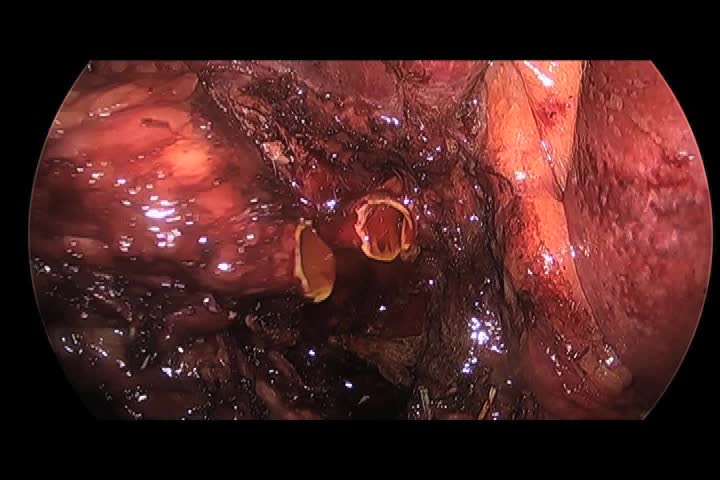
A 60-year-old man presented with vague abdominal pain, intermittent fevers, and elevated liver function tests. A dilated biliary tree down to the ampulla was appreciated on magnetic resonance cholangiopancreatography. On endoscopic retrograde cholangiopancreatography (ERCP) and cholangioscopy, an intrahepatic low-grade IPMN was found with the majority confined to the main trunk with extension into the right main hepatic branch. We performed a resection of the neoplasm through a laparoscopic right hepatectomy with common bile duct and right hepatic duct excision and Roux-en-Y hepatojejunostomy with an internally placed biliary stent. A total of five trocars were utilized as was a robotically controlled laparoscope holder (VideoendosKopY, ViKY, Endocontrol, Grenoble, France). Estimated blood loss was 200 mL, and the surgery took a total of 6 hours.
Results:
The patient's drain was removed on postoperative day 5 as it had minimal serous drainage. The patient was sent home on postoperative day 6. Final pathology report was consistent with a low-grade BT-IPMN with disease-free margins. Postoperatively he continued to suffer from intermittent fevers and ultimately underwent percutaneous drainage on postoperative day 60 for a small postoperative fluid collection along his transection margin and was treated for a pseudomonal infection. His intermittent fevers persisted until he underwent ERCP and endoscopic removal of his preoperatively placed biliary stent 6 months postsurgery.
Discussion:
IPMNs are considered the precancerous counterpart to carcinoma of the pancreas.1 Between 1994 and 2006, 23/253 (9%) histopathologic samples of IPMNs were determined to be BT-IPMNs. In 2 of these 23, BT-IPMN was localized to the extrahepatic ducts not involving the hilum in 12 patients (52%), to the intrahepatic ducts in 6 patients (26%), and to the hilum in 5 patients (22%).2 Like most cases of BT-IPMNs, our case presented as merely a dilated bile duct with intrahepatic extension.3 The uncommon location of our patient's neoplasm undoubtedly made the nature and logistics of this surgery more complex. Because of the extrahepatic nature of the disease, a complex reconstruction of the biliary tree was necessary.4 BT-IPMNs are premalignant lesions and should be completely excised. Owing to the mucinous secretions in the bile duct and associated biliary stasis, it may be prudent to also cover patients for pseudomonas. Patients with BT-IPMNs may also be ideal candidates for minimally invasive resections as they may benefit from decreased pain, shorter return to work, and improved cosmesis associated with laparoscopy.
No competing financial interests exist
.
Runtime of video: 8 mins
This video was presented at the American College of Surgeons in San Diego, California, October 22–26, 2017.


Keywords
Get full access to this article
View all access options for this article.