
Abstract
Introduction and Objectives:
Bladder diverticula from bladder outlet obstruction (BOO) due to benign prostatic hyperplasia (BPH) can lead to high postvoid residuals (PVR), infections, stones, or malignancies, often requiring surgery. Combining a bladder outlet-reducing procedure with diverticulectomy may reduce morbidity and improve outcomes. Here, we report our experience with simultaneous holmium laser enucleation of the prostate (HoLEP) and robot-assisted bladder diverticulectomy, presenting what we believe to be the first robotic case series of this combined procedure. 1
Patient Characteristics and Outcomes IQR, interquartile range; BMI, body mass index; 5ARI, 5—alpha reductase inhibitors; PVR, postvoid residual volume; EBL, estimated blood loss; SUI, stress urinary incontinence.
Variables
Age, years, median (IQR)
70 (59.5–79)
BMI, kg/m2, median (IQR)
27.2 (24.6–30.7)
Prostate size, cm3, median (IQR)
42 (30–62.5)
The greatest dimension of the largest diverticula, cm, median (IQR)
9.3 (7.25–12.2)
Preop retention rate,
3 (60%)
Preop catheter dependence,
2 (40%)
Preop use of alpha-blockers,
5 (100%)
Preop use of 5ARIs,
2 (40%)
Preop PVR, mL, median (IQR)
343 (137.25–546.5)
History of previous interventions,
1 (20%)
ASA score,
2
3 (60%)
3
2 (40%)
Total procedure time, minutes, median (IQR)
334 (282.5–420)
EBL, mL, median (IQR)
125 (57.5–150)
Perioperative complications,
0
Length of catheterization, days, median (IQR)
26 (20.5–26.5)
Length of hospital stay, days, median (IQR)
2 (1–2)
Pathological weight of resected adenoma, gr, median (IQR)
18.4 (7.95–20.3)
Postop PVR, mL, median (IQR)
3 (0–26)
Time to first follow-up visit, weeks, median (IQR)
8 (2.5–8.5)
Postop SUI at first f/u,
1 (20%)
Postop SUI at 3 months,
1 (20%)
Postoperative complications:
Clavien Dindo Grade,
≤II
1 (20%)
≥III
1 (20%)
Postop readmission in 90 days,
1 (20%)
Methods:
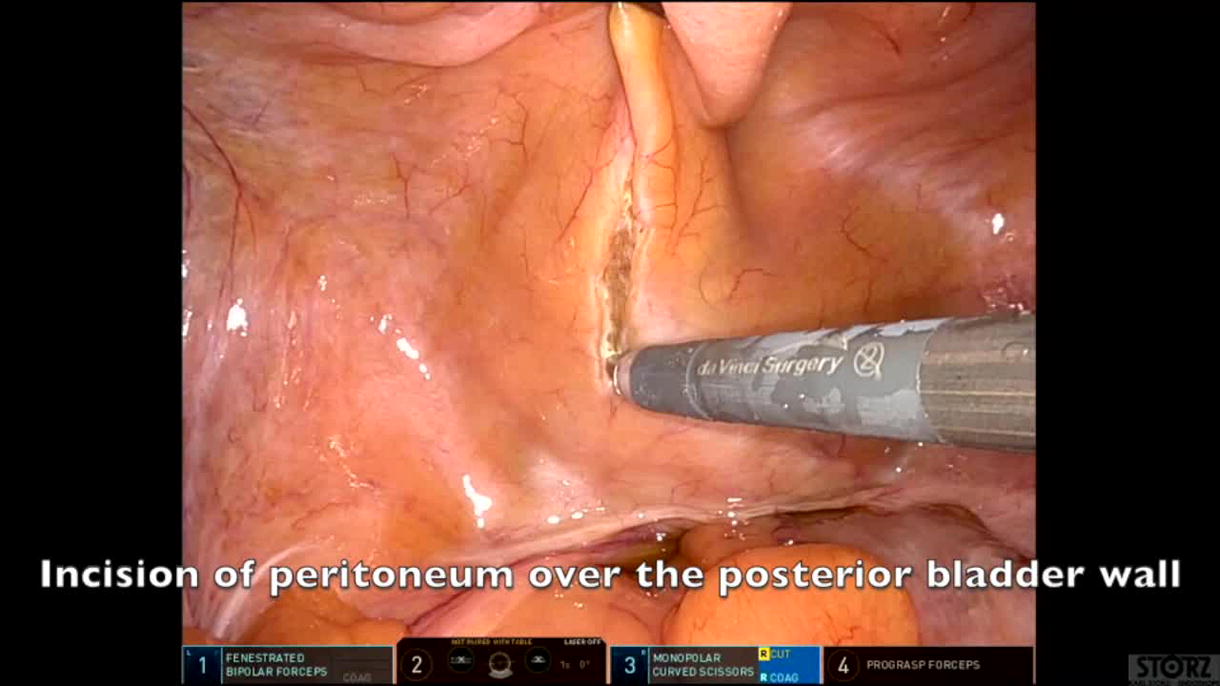
Five patients with bladder diverticula (ranging from 6.0 cm to 12.4 cm in diameter) and clinically diagnosed BOO due to BPH underwent concurrent HoLEP and robot-assisted bladder diverticulectomy between May 2023 and April 2024. The standard two-lobe technique was used for HoLEP, with the prostate adenoma morcellated endoscopically before the robot-assisted diverticulectomy. The cystotomy was closed in a single layer with 3-0 V-Loc, and a peritoneal flap was used to separate the repair from the bowels. Postoperatively, patients were admitted, received continuous bladder irrigation until the urine cleared, and had an indwelling catheter for at least 3 weeks. A cystogram confirmed an intact repair before catheter removal and a voiding trial.
Results:
The median age of the patients was 70 years (IQR 59.5–79), and the median preoperative PVR was 343 cc (IQR 137.25–546.5). Three patients had a history of urinary retention, with two being catheter-dependent before surgery. The median estimated blood loss was 125 cc (IQR 57.5–150), with no perioperative complications or need for transfusions. The average hospital stay was two days, and the median catheterization period was 26 days (IQR 20.5–26.5). The median postoperative PVR decreased to 3 cc (IQR 0–26). Four patients reported full continence by 3 months, and one patient experienced transient stress urinary incontinence, which resolved by 6 months (Table 1).
Conclusion:
Simultaneous HoLEP and robotic bladder diverticulectomy is a feasible option for patients with symptomatic diverticula and BOO. Further studies with larger patient cohorts are needed to evaluate long-term outcomes.
Conflicts of Interest:
None.
Disclosures:
No commercial associations or conflicts of interest to disclose. The author(s) have received and archived patient consent for video recording/publication in advance of video recording of the procedure. No commercial associations or funding to report.
Runtime of video: 6 mins 24 secs.
Keywords
Get full access to this article
View all access options for this article.