
Abstract
Introduction:
A recognized adverse effect from radiation therapy is radiation-induced ureteral strictures (RIUS) resulting in renal damage, infection, and pain. Buccal graft ureteroplasty is being increasingly utilized with high success rates and minimal complication rates. 2,3 Use of the daVinci single port (SP) for bilateral ureteral stricture repair has not been described. In this video, we demonstrate a case of bilateral RIUS following radiation therapy for cervical cancer, treated with bilateral buccal graft onlay ureteroplasty using the daVinci SP robot, which allowed access to both ureters without having to redock or reposition the patient.
Clinical History:
This is a patient with a history of cervical cancer treated with hysterectomy and radiation therapy who subsequently developed bilateral ureteral strictures managed with ureteral stents.
Diagnosis:
The patient underwent placement of bilateral nephrostomy tubes and removal of ureteral stents for ureteral rest 6 weeks prior to planned intervention. Combined antegrade nephrostogram and retrograde pyelogram revealed a 4-cm right mid-ureteral stricture and a 2-cm left mid-ureteral stricture.
Intervention:
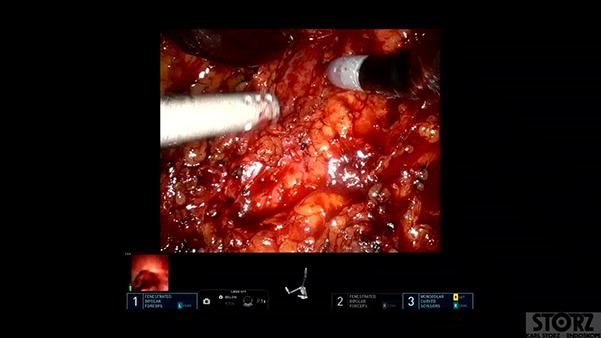
She was brought to the operating for robotic assisted bilateral ureteral stricture repair with buccal graft using the daVinci SP robot. She was positioned supine on a split-leg table. Flexible cystoscopy was used to cannulate both ureters with two guidewires to allow for facile intra-operative ureteroscopy. A 3-cm infra-umbilical incision was made through her prior hysterectomy scar. The intuitive SP globe was utilized for floating dock technique. 1 A 5-mm assistant port was placed in the right lower quadrant. After extensive lysis of adhesion was performed, the posterior peritoneum was incised at the pelvic brim and was tacked to the anterior abdominal wall using traction sutures on a Keith needle. There was dense fibrosis and rind encasing both of her ureters, so intra-operative ureteroscopy with Firefly™ was used to help identify the ureters and their corresponding strictures. On right-sided ureteroscopy, mid-ureteral stones were identified and extracted with a basket. There were still endoluminal findings consistent with a ureteral stricture, so an approximately 5-cm right-sided ureterostomy was performed until the ureteroscope could easily pass into the proximal ureter. Left sided ureterostomy was performed in a similar manner and measured approximately 3 cm. Buccal harvest was performed. Bilateral buccal graft onlay was performed using two 4-0 polydioxanone sutures over ureteral stents. Perivesical fat was used to guilt both grafts. Bilateral nephrostomy tubes were removed in the recovery room after confirmation of appropriate ureteral stent positioning.
Follow-Up/Outcomes:
She was discharged on postoperative day 1. Ureteral stents were removed after 6 weeks. At 5 months postoperatively, a renal function scan demonstrated prompt drainage with a tracer half-life of 12.7 minutes on the left and 6.2 minutes on the right.
Conclusions:
Using the daVinci SP robot allowed for access and treatment of both of the ureters through her prior incision, without having to redock or reposition the patient. The use of the SP robot is an excellent option for patients in need of bilateral ureteral reconstruction.
Author Disclosure Statement:
Authors do not have any commercial associations during the last 3 years that might create a conflict of interest in connection with the video. The authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Runtime of video: 5 mins and 0 secs.
*This video was presented at the North American Robotic Urology Symposium 2024.
Get full access to this article
View all access options for this article.