
Abstract
Introduction:
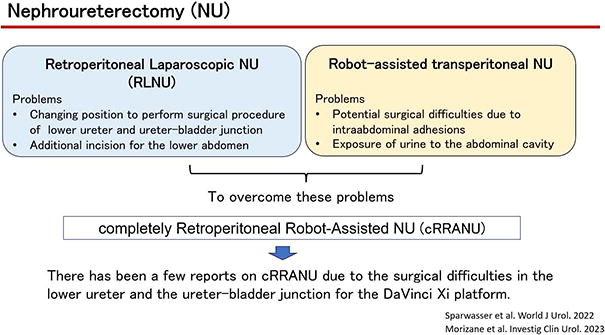
To date, nephroureterectomy has been performed using two main approaches, one of which is laparoscopic nephroureterectomy (LNU) via a transretroperitoneal approach (RLNU). This approach has two problems. First, it is necessary to intraoperatively change the patient’s position from the lateral to supine position in order to perform surgery on the lower ureter and the ureter-bladder junction. Second, an additional lower abdominal incision is required to perform the surgical procedure.
Robot-assisted transperitoneal nephroureterectomy is another approach that is recently being performed globally. 1 However, there are two problems with this procedure. First, potential surgical difficulties arise due to intra-abdominal adhesions from previous intra-abdominal surgery, and the other is potential leakage of urine into the abdominal cavity.
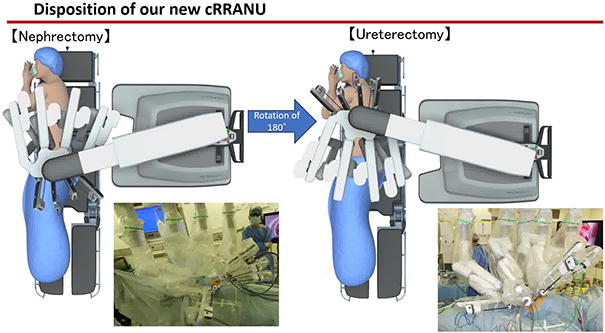
To overcome these problems, a completely robotic retroperitoneal nephroureterectomy was considered appropriate. However, there have been only a few reports on completely retroperitoneal robot-assisted nephroureterectomy (cRRANU) due to the surgical difficulties related to the lower ureter and the ureter–bladder junction with the DaVinci Xi platform. 2,3 Thus, we developed a new cRRANU procedure to overcome these difficulties. The aim of this study was to compare perioperative surgical outcomes and minimal invasiveness of our new cRRANU procedure with those of conventional RLNU.
Materials and Methods:
The study investigated 25 consecutive patients who underwent nephroureterectomy at our institution from April 2021 to March 2023. All cases were performed via the retroperitoneal approach, with eight cases undergoing cRRANU and 17 cases undergoing RLNU. The study compared perioperative parameters and wound conditions between the two procedures. The perioperative parameters evaluated included surgical duration, estimated blood loss (EBL), number of lymph nodes dissected, and perioperative complications. The wound was evaluated based on the number and frequency of painkiller usage, visual analogue scale (VAS) for pain at day 7 after surgery, and Derriford appearance scale (DAS59). DAS59 is currently the only available validated patient-reported outcome measure that assesses concerns about physical appearance.
Results:
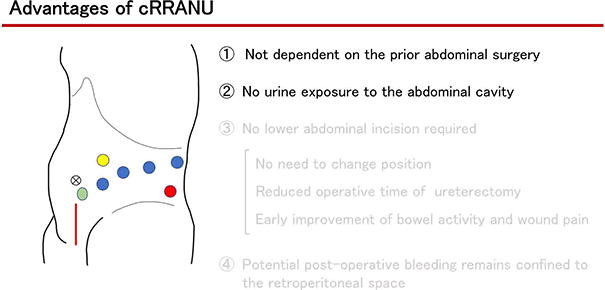
Total operative time was not significantly different between the two groups (RANU: LNU = 368 ± 51 min: 413 ± 76 min, p = 0.14). The time for ureterectomy was significantly shorter in the cRRANU group (cRRANU: LNU = 108 ± 23 min: 179 ± 52 min, p = 0.001). EBL, number of lymph nodes dissected, and perioperative complications were not significantly different between the two groups. Regarding the perioperative complications, the postoperative chyle discharge was observed in one patient who underwent LNU.
Time to flatus was significantly shorter in the cRRANU group (cRRANU: LNU = 2.1 ± 0.6 days: 3.6 ± 1.1 days, p = 0.002). No significant difference of the time to restoration of eating was observed between the two groups (cRRANU: LNU = 2.3 ± 0.7 days: 2.1 ± 0.5 days, p = 0.44). In addition, no significant difference in the time to mobilization was observed between the two groups (cRRANU: LNU= 1.5 ± 1.0 days: 2.0 ± 0.8 days, p = 0.22).
The number and frequency of postoperative pain killer usage were not significantly different between the two groups (cRRANU: LNU = 1.7 ± 2.4: 2.9 ± 2.2, p = 0.24). VAS scores at day 7 after surgery were significantly lower in the cRRANU group (cRRANU: LNU = 10 ± 14: 33 ± 22, p = 0.03). DAS59 was not significantly different between the two groups (cRRANU: LNU = 19 ± 27: 32 ± 38, p = 0.41).
Conclusions:
Our cRRANU procedure is less invasive than RLNU, reducing the operative time for ureterectomy and providing early improvement of bowel activity and early relief from postoperative pain.
Patient Consent Statement:
The authors obtained and archived patient consent for video recording/publication prior to video recording the procedure.
Runtime of video: 9 mins 57 secs.
All authors have no conflict of interest.
Get full access to this article
View all access options for this article.