
Abstract
Introduction:
The mini-perc technique was developed in 1997 to reduce trauma during percutaneous nephrolithotomy (PCNL) in children. 1 The first ultrasound-guided mini-perc was performed in 1999 by Desai et al. 2 Super mini PCNL (SMP) developed by Zeng et al. improves the mini-perc by using an irrigation–suction sheath that allows continuous suction of fragments and prevents excessive intrarenal pressure, improving observation and extraction of the stone. 3 Ultrasound-guided SMP has demonstrated a safe and effective treatment with the advantage of avoiding radiation. 4 Li et al. described the two-step dilation in standard ultrasound-guided PCNL 5 ; in this video, we describe the advantages of this technique in improving safety in SMP totally ultrasound-guided.
Materials and Methods:
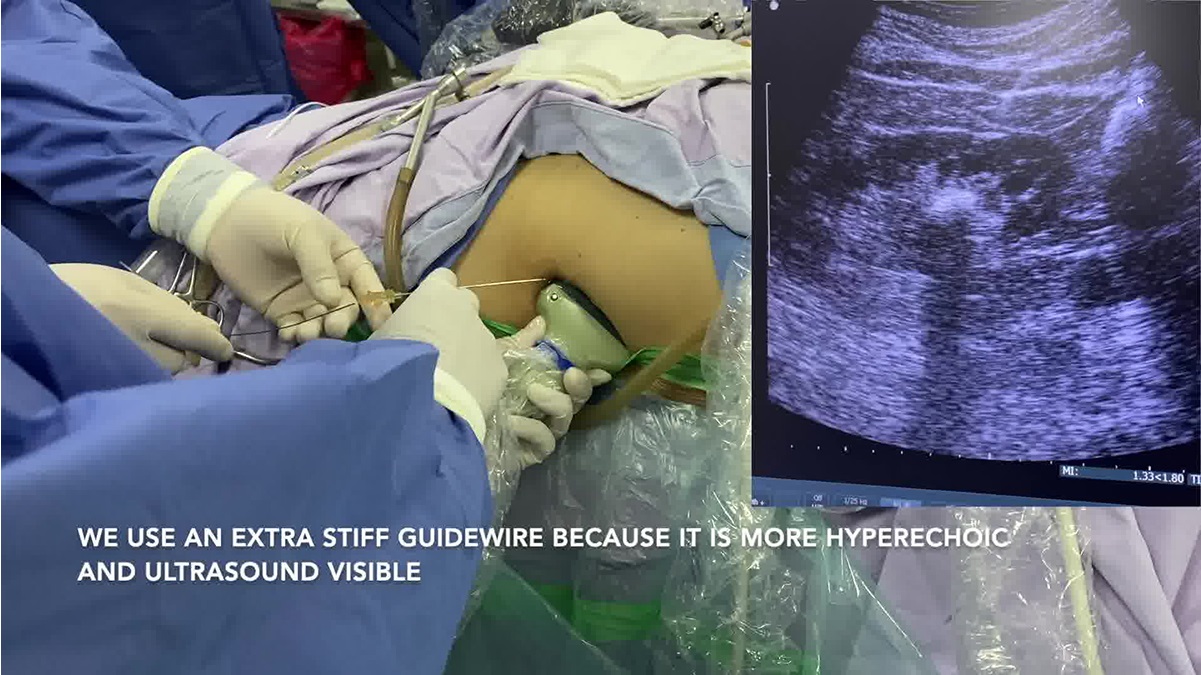
Between July 2022 and July 2023, 15 patients underwent totally ultrasound-guided SMP with a two-step tract dilation. Surgical technique: In the Galdakao-modified Valdivia position, previous placement of a ureteral occlusion catheter, we adjusted the ultrasound parameters: gain, focus, depth, and dynamic range, and used an echogenic needle. 6 The access was obtained with a longitudinal freehand technique, obtaining urine indicates a successful puncture, an extra stiff guide was passed and sequential dilation (Step 1) with 10F to 12F to 14F fascial dilators; as it advances into the collector system, the dilator hides the guide and a plastic 14F peel-away sheath is placed (The plastic sheath does not create artifacts when observed with ultrasound, unlike metal sheaths, allowing better and safer control of dilation). An antegrade nephroscopy is performed to check the renal cavities and measure the length of the tract, and a pair of guides are placed in the ureter, one for definitive dilatation and the other as a safety guide. (Step 2): Placement of definitive metallic 14F irrigation–suction sheath (Hawk) under ultrasound control; insert 1 cm in addition to the previously measured length of the plastic sheath to avoid a short dilation; lithotripsy was performed with a 40 W holmium laser using fragmentation settings. The safety guidewire remains outside of the definitive sheath, and this enhances safety and prevents tract loss if the sheath is accidentally removed.
Results:
Dilation problems such as short dilation, tract loss, and collecting system injury were not encountered in any patient. The average age was 44 years, with a BMI of 28.3 ± 4.5 kg/m2, with a predominance of left kidney stones in 53% of cases. The average stone burden was 2263 ± 1213 mm3 (837 HU) the most frequent location was in the lower calix (46%). The mean operative time was 79 minutes (80–120). The lower calix was punctured in 53% with an average puncture time of 51 seconds. Because of the hypermobility of the lower pole, we migrated to routinely access the middle calyx. A single tract in 93% of cases, obtaining 93% stone free and totally tubeless in all cases. 80% of the procedures were ambulatory. The mean hemoglobin loss was 1.14 g/dL; only three patients had fever (Clavien I), and no other complications were recorded.
Conclusions:
This dilation technique appears to increase the safety of the procedure. SMP allows a good stone-free rate and can be an ambulatory and totally tubeless surgery.
The study adhered to institutional review board protocols. Surgical videos were recorded with patient consent during routine care.
Consent for video recording and publication of procedure was obtained and archived before the recording.
No competing financial interests exist.
Runtime of video: 8 mins 32 secs

Get full access to this article
View all access options for this article.