
Abstract
Clinical History:
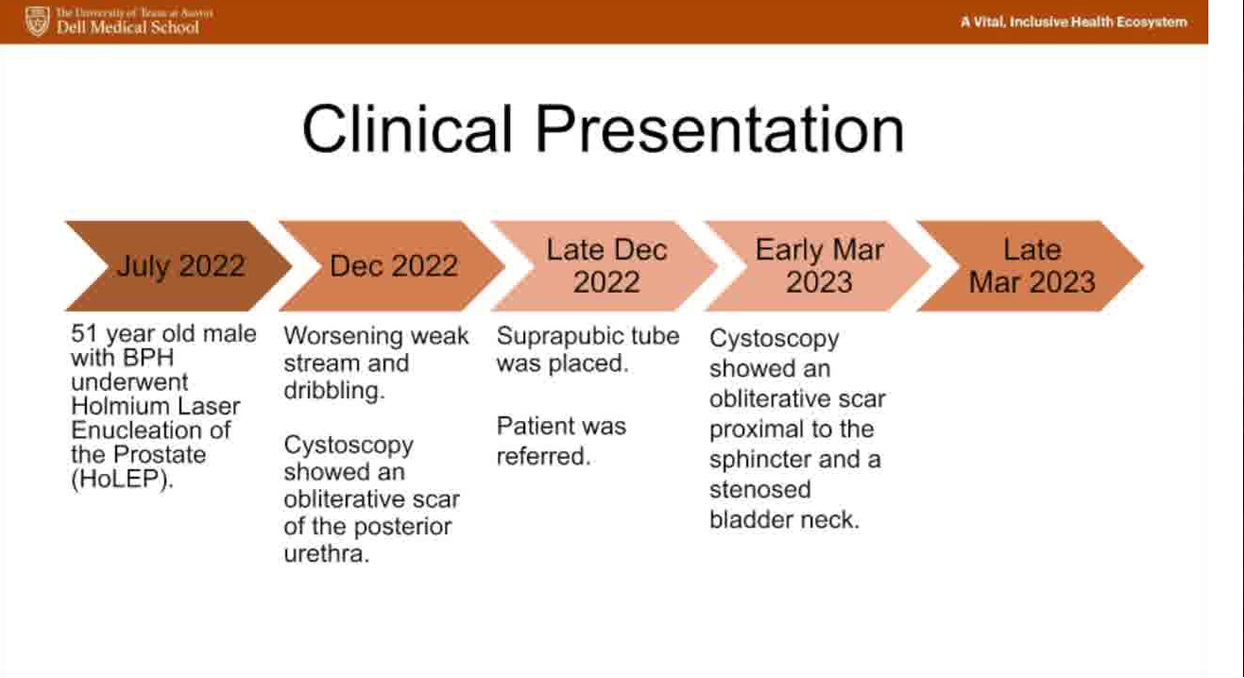
A 51-year-old man underwent holmium laser enucleation of the prostate (HoLEP) for benign prostatic hyperplasia. Within 6 months, he developed worsening lower urinary tract symptoms.
Physical Examination:
Physical examination was unremarkable.
Diagnosis:
Retrograde cystoscopy demonstrated an obliterative stenosis 2 cm proximal to the external sphincter, and antegrade cystoscopy through his suprapubic tube tract demonstrated a 5F stenosed bladder neck. A transvesical robotic bladder neck reconstruction for posterior urethral stenosis was then performed.
Intervention:
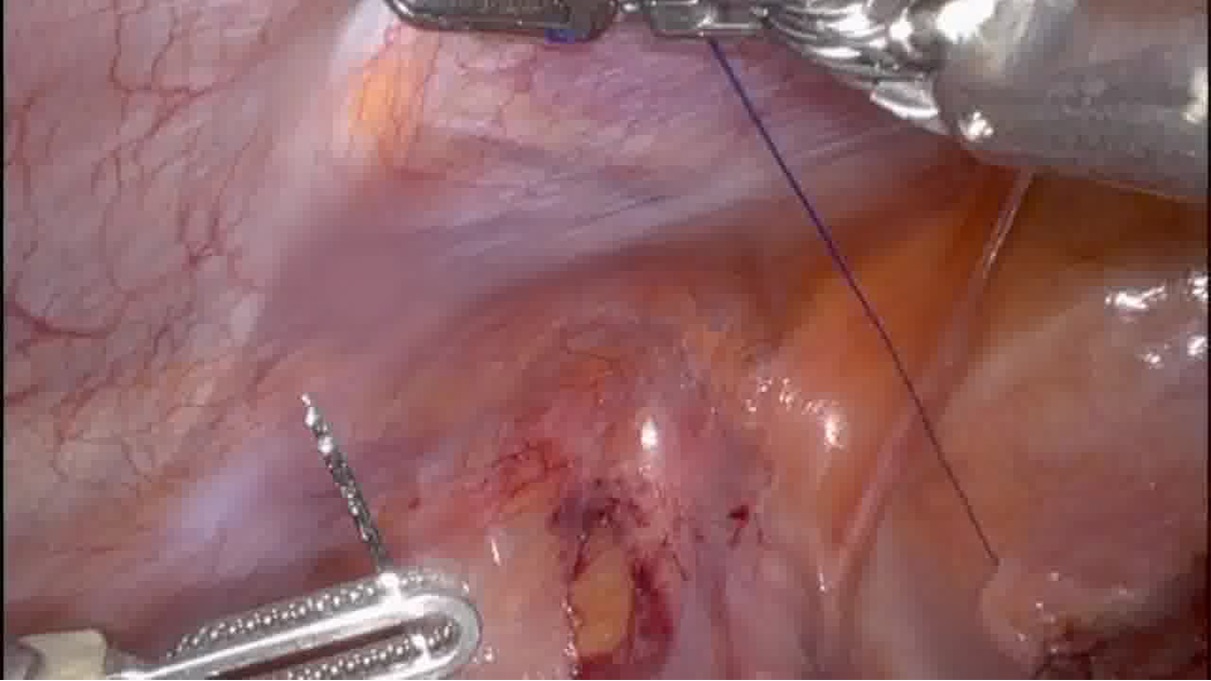
The procedure began with retrograde and antegrade cystoscopy confirming the presence of the bladder neck stenosis. After standard entry into the abdomen, a 4 cm vertical cystotomy of the bladder was performed for a transvesical approach. A circumscribing incision around the bladder neck contracture was made using electrocautery. The stenosed bladder neck and prostatic urethral stenosis were excised. The bladder neck mucosa was then undermined allowing for the release of a local bladder neck advancement flap. A running anastomosis with 3-0 Monocryl was performed to reapproximate urethral mucosa to bladder neck mucosa. A Foley catheter was left in place.
Follow-Up/Outcomes:
The patient's postoperative course was uncomplicated. He was discharged home on postoperative day 1 with a Foley catheter in place. Two weeks later, a voiding cystourethrogram showed a well-healed anastomosis without evidence of contrast extravasation. At 3-month follow-up, cystoscopy showed a patent anastomosis. In this case, we validate the usefulness of a conventional robot-assisted system for a transvesical bladder neck reconstruction to repair posterior urethral stenosis after HoLEP, highlighting the surgical technique and its potential clinical utility.
No competing financial interests exist.
Music: Pixabay.com, PaulYudin, Romantic Piano Inspirational (not copyrighted).
Patient Consent: Authors have received patient consent for video recording/publication in advance of video recording of procedure.
Source: Dell Seton Medical Center at The University of Texas at Austin
Runtime of video: 5 mins 55 secs
Get full access to this article
View all access options for this article.