
Abstract
Introduction:
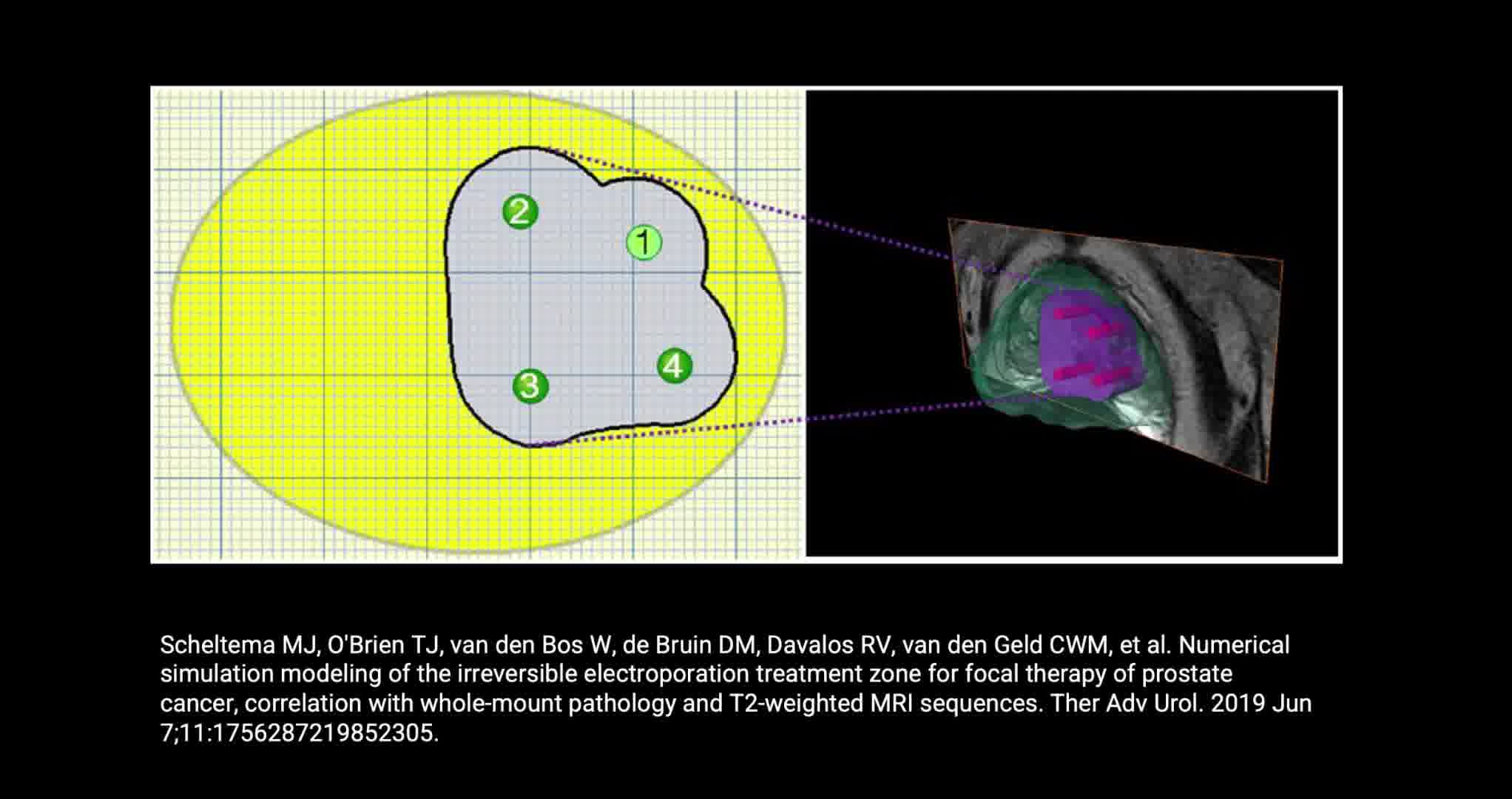
Focal therapy has emerged as an alternate treatment for men with localized prostate cancer (PCa). Irreversible electroporation (IRE) is an available technique for focal ablation. IRE ablates prostate tissue by delivering direct current between electrodes placed transperineally into the prostate. During IRE a characteristic sign, which we propose to term the “Stricker Sign,” is noted in the ablation field. The sign appears as a hyperechoic ring formed between the electrodes on the periphery of the ablated area, while the PCa lesion within becomes hypoechoic. The presence of this event provides real-time feedback to the surgeon, indicating that the targeted lesion has been covered during ablation with an acceptable margin of benign tissue around the tumor. The ablation zone extents outside the needle configuration due to resulting spheric electrical field. 1
Materials and Methods:
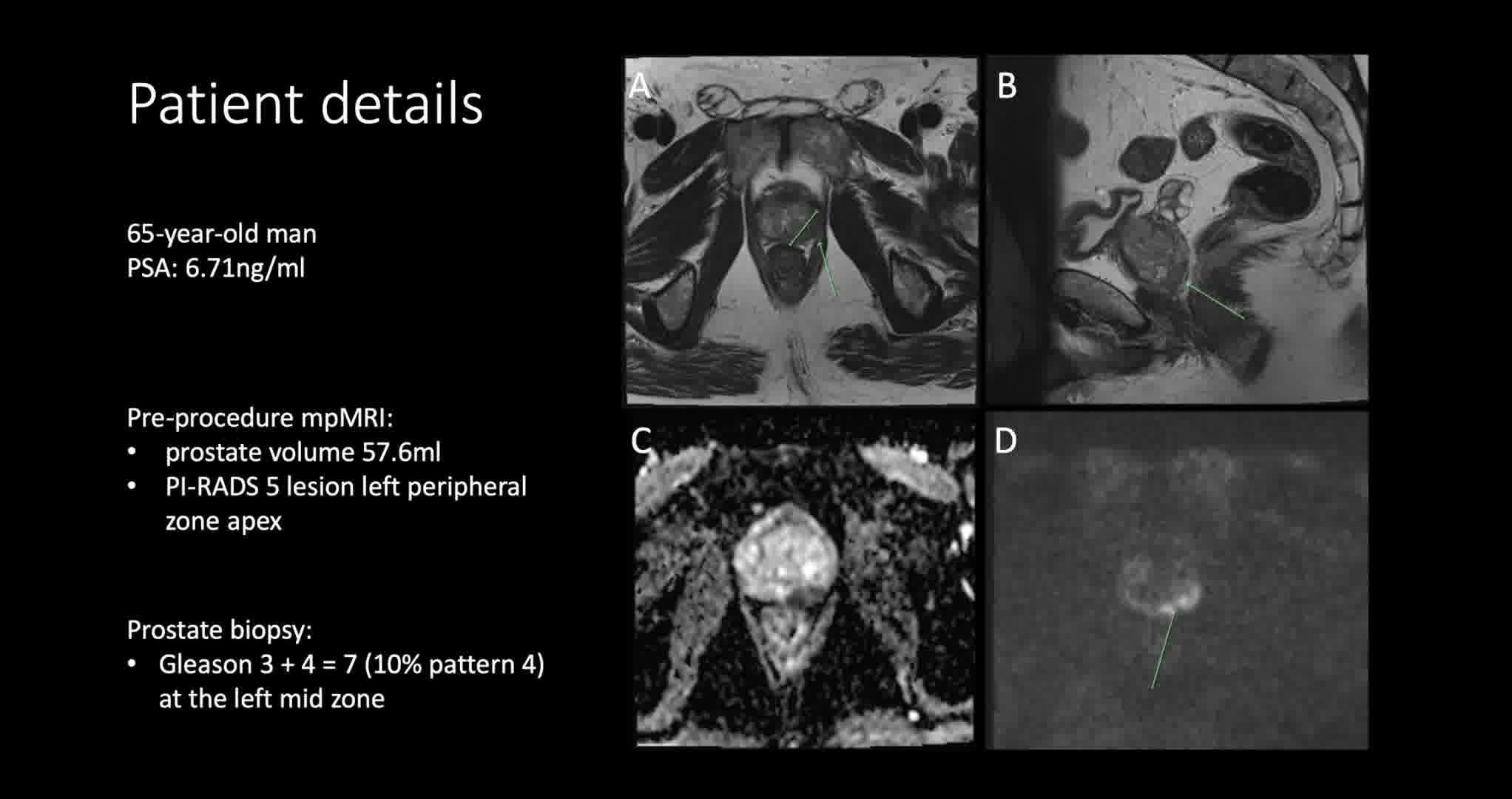
Written patient consent obtained. Intraprocedural transrectal ultrasound imaging was performed on a 65-year-old man referred with a PSA of 6.71 ng/mL. His preprocedure multiparametric magnetic resonance imaging (mpMRI) demonstrated a prostate volume of 57.6 mL (PSA density 0.11 ng/mL2) and a 24 mm Prostate Imaging-Reporting and Data System (PI-RADS) 5 lesion in the left peripheral zone at the apex. His prostate biopsy revealed Gleason 3 + 4 = 7 with 10% pattern 4 in 30% of material at the left midprostate. Prostate-specific membrane antigen (PSMA) positron emission tomography-computed tomography following biopsy revealed intense PSMA avidity in the posterolateral left peripheral zone at the prostatic apex, without metastatic disease. After thorough counseling, the patient elected focal therapy and proceeded to have irreversible electroporation (IRE) of the left apex using the Nanoknife® system. The technique for IRE has been previously published in detail. 2,3
Results:
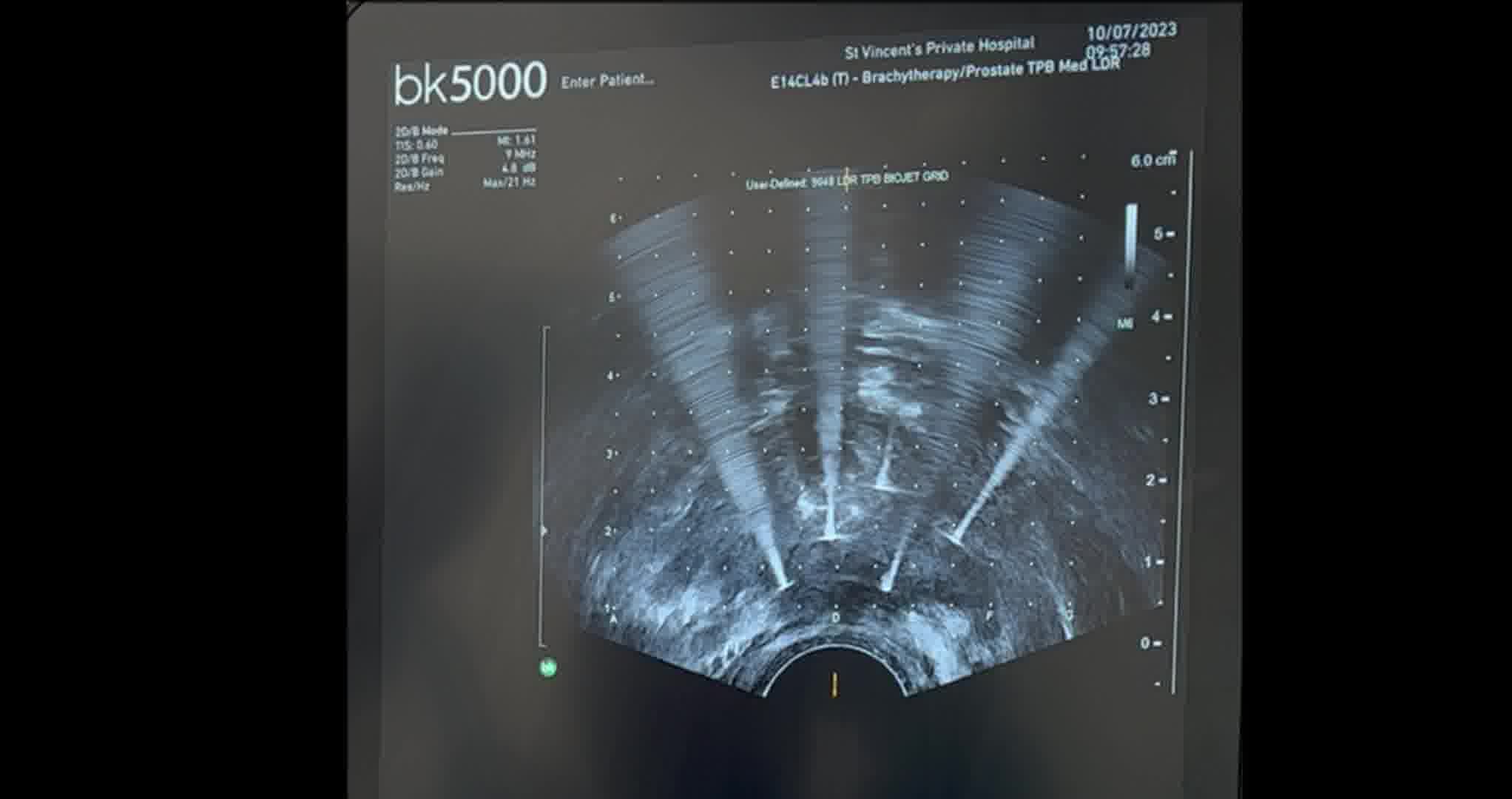
Throughout the course of the procedure, as shown on ultrasound imaging, a characteristic sign is noted in the ablation field—the PCa lesion remains hypoechoic, while a hyperechoic ring forms as the current runs between/around the electrodes on the periphery of the ablated area. This assists in confirming that the region of interest has been successfully targeted. A MRI was performed 2 days after IRE to confirm the ablation covered the tumor location, overlapping the “Stricker sign.” The sign arises from the increased tissue density and reduced water content of PCa, compared to normal prostatic tissue. It has been well established that PCa has a different density and water content compared to normal prostatic tissue and results in restricted diffusion in mpMRI of the prostate. 4,5 The hyperechoic ring is formed due to the comparatively high water content of the ablated benign tissue. As the electrical impulses are transmitted, electrolysis of water occurs which leads to production of hydrogen and oxygen gas. In contrast, PCa has a lower water content, and thus does not produce as much gas, leading to the progressively hypoechoic appearance.
Conclusions:
Currently, patients are required to have a repeat mpMRI within 1 week of the procedure to confirm the region of interest has been covered. Use ultrasound-guidance provides the surgeon with real-time feedback, immediately demonstrating ablation of the targeted lesion with a margin of benign tissue.
Authors received/archived patient consent for video recording/publication in advance.
M.J.S.: Angiodynamics Educational grant. P.D.S.: Angiodynamics paid consultant
.
Runtime of video: 3 mins 29 secs
Get full access to this article
View all access options for this article.