
Abstract
Introduction:
Minimally invasive simple prostatectomy is one of the recommended treatment options for large prostatic adenomas, 1 and laparoscopic simple prostatectomy (LSP) is favored at the authors' institution when the prostate volume is >150 cc. LSP can be performed using transvesical, transcapsular, and transvesicocapsular approaches. 1 In our experience, vesicocapsular adenoidectomy provides good observation and works well for large benign prostate glands. We present our surgical technique with video demonstration and report the outcomes.
Materials and Methods:
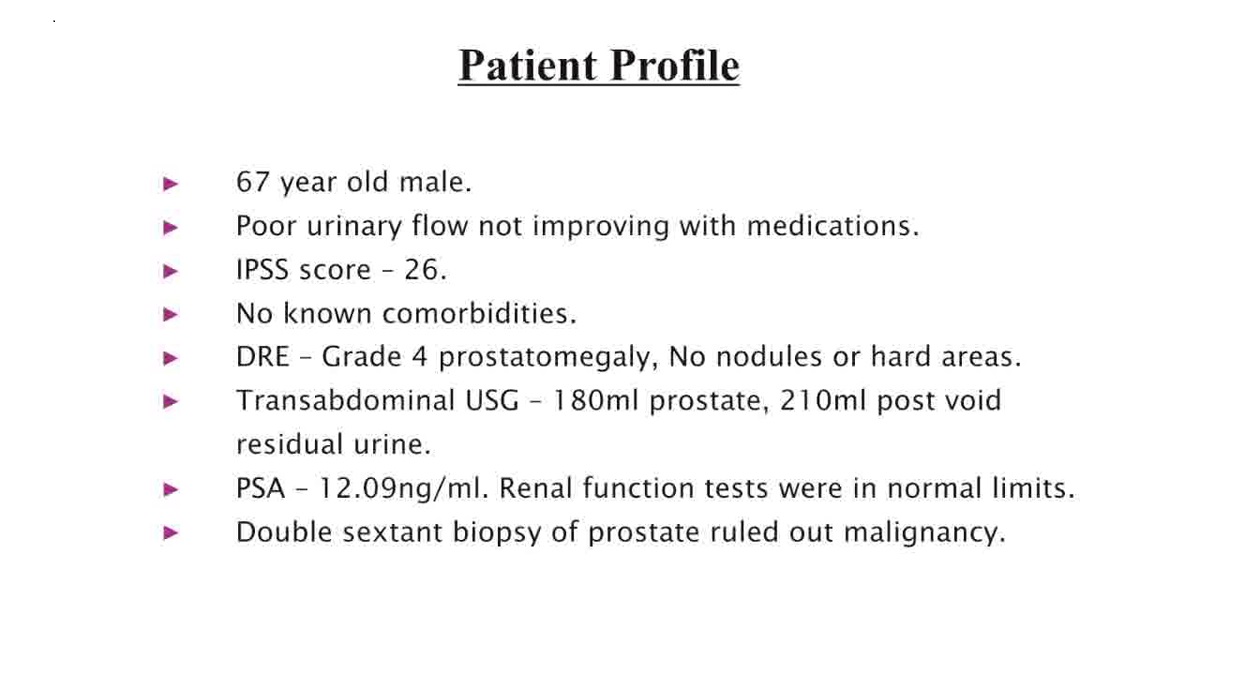
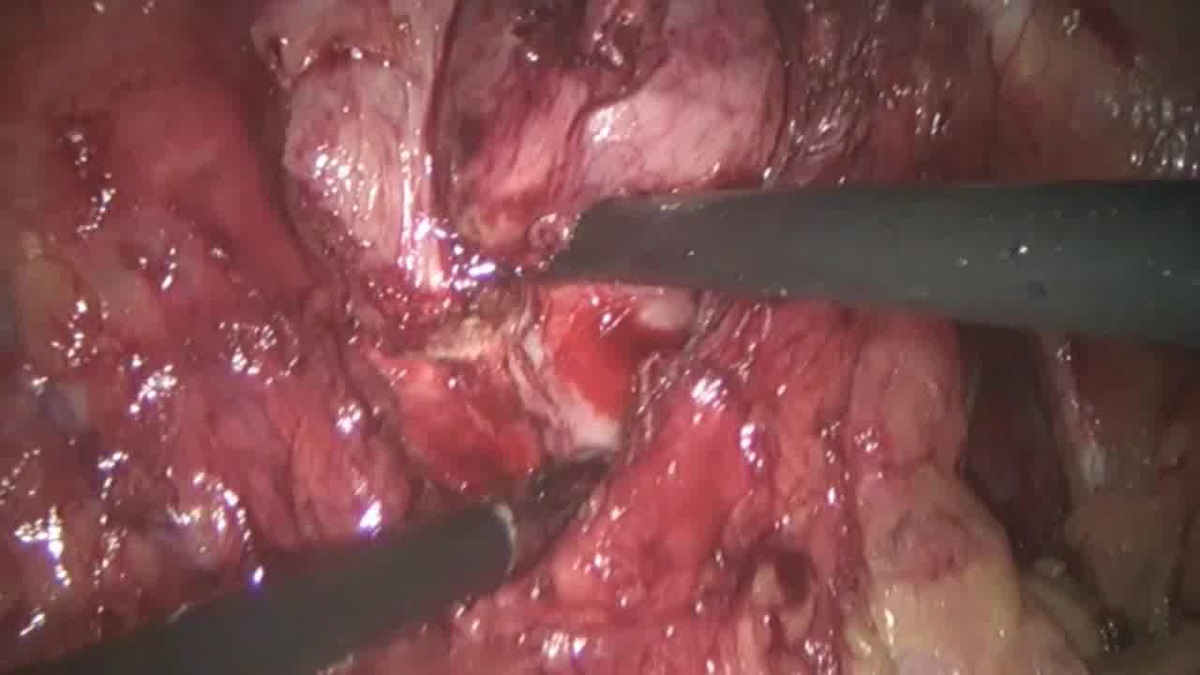
The procedures were performed by a single surgeon with good experience in laparoscopic radical prostatectomy. The patients were positioned in Trendelenburg position. After transperitoneal access, urinary bladder was mobilized completely and the prostate was exposed. The endopelvic fascia was incised and puboprostatic ligament was partially divided. The dorsal vein complex was then ligated. 2 Hemostatic stiches were not routinely placed on the lateral pedicles of the prostate before enucleation. Bladder neck was identified and adequate anterior vertical vesicocapsular incision was made. Circumferential enucleation of the prostatic adenoma was completed from the prostatic base to apex. Care was taken not to injure the external sphincter during apical dissection. Retrigonization was performed by suturing the bladder trigonal mucosa to posterior wall of the urethra and/or posterior prostatic capsule. 3 The anterior vesicocapsular incision was closed over a Foley catheter. Data of patients with prostate volume >150 cc in transabdominal ultrasonography and who had undergone LSP during the period between January 2014 and December 2020 were collected retrospectively.
Results:
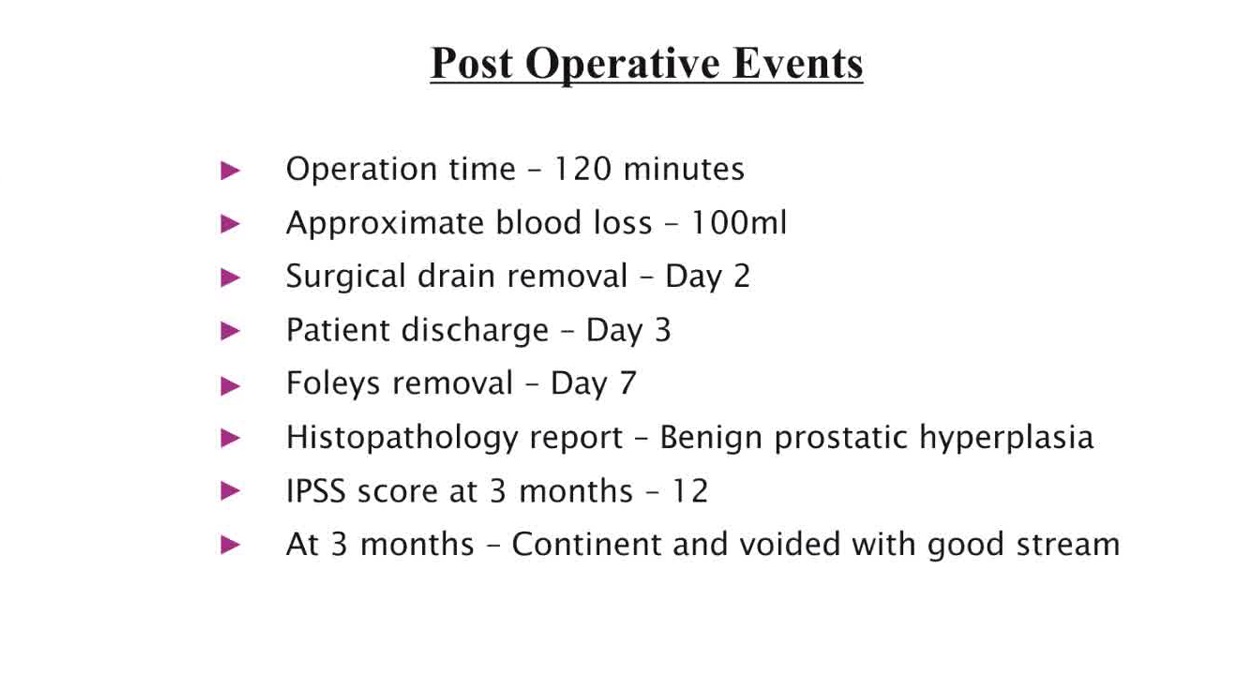
Five patients were available for the analysis. The mean age was 70.6 ± 5.727 years (range 63–77 years). The mean prostate volume in preoperative transabdominal ultrasonography was 188.4 ± 23.426 cc (range 160–224 cc). The mean preoperative international prostate symptom score (IPSS) was 24.2 ± 3.271 (range 21–29). The mean operative time was 121 ± 19.494 minutes (range 90–140 minutes). The mean intraoperative blood loss was 130 ± 21.213 mL (range 100–150 mL). None of the patients needed blood transfusion during or after surgery. The mean weight of the excised adenoidectomy specimens was 158 ± 21.389 g (range 125–180 g). The mean duration of hospitalization was 4.6 ± 0.548 days (range 4–5 days). The histopathology report was benign in all cases. The mean duration of Foley catheterization after surgery was 8.2 ± 1.304 days (range 7–10 days). None of the patients needed Foley reinsertion after initial removal. The mean postoperative IPSS score at 3 months was 12 ± 1.581 (range 10–14). None of the patients had incontinence at 3 months follow-up.
Conclusions:
LSP using the vesicocapsular approach for large benign prostatic adenomas is effective and safe. By this approach, morbidity can be kept to a minimum, prostate symptoms can be alleviated, and continence can be preserved. To our knowledge, this study is the first of the LSP techniques focused exclusively on prostate glands >150 cc. Prospective multicentric studies will help in assessing reproducibility of similar outcomes in a larger population. Also, comparative studies with other laparoscopy and robot-assisted techniques are required to clearly define the role of laparoscopic vesicocapsular adenoidectomy in the management of large benign prostate glands.
No competing financial interests exist.
The author(s) have received and archived the patient consent for video recording/publication before video recording of the procedure.
No external funding was used.
Runtime of video: 6 mins 57 secs
Keywords
Get full access to this article
View all access options for this article.