
Abstract
Introduction:
Percutaneous nephrolithotomy (PCNL) is the current gold standard for the management of large renal stones. Traditionally PCNL has been done in prone position. Although supine PCNL was first described by Valdivia Uria et al in 1987, the use of supine position is becoming popular in the recent decades only. 1,2 Although supine PCNL has a lot of advantages, there are two disadvantages associated with this position. 3 These are longer tract length and hypermobility of kidney during tract dilatation. 3 We present our ultrasound-guided anterior caliceal approach in supine PCNL that can overcome these two problems in supine PCNL, making supine PCNL a more refined technique.
Patients and Methods:
Between June 2016 and March 2020, 94 patients underwent supine PCNL in ultrasound-guided supine PCNL. Of these, six patients in whom anterior caliceal approach could not be used because of interference of colon or liver were excluded. All patients were evaluated using computed tomography scan preoperatively. Informed consent was obtained from all patients. The mean stone size was 2.7 cm. Patients were placed in supine oblique hemilithotomy position, in which the contralateral lower limb was kept in lithotomy and ipsilateral lower limb was kept straight on a pillow. The patient was tilted to 30°–45°. We do not use any arbitrary anterior limit for puncture site. We prefer lower anterior calix for entry. Ultrasound scan was used to find the most direct and shortest tract in all patients. Tranexamic acid was used in all patients as per the previously reported protocol. 4 Tract was dilated using 14F screw dilator followed by a single-step teflon dilator over guide rod. The tract size used ranged from 14F to 22F. Stones were observed using 12F or 18.5F Wolf nephroscope and fragmented using pneumatic lithotripter. Flexible nephroscope was used when the tract size of 18F or above was used. Double-J stent was placed in all patients. Most of the patients underwent a tubeless procedure. Hemoglobin loss was estimated postoperative hemoglobin value on discharge. Stone clearance was assessed using kidney, ureter, and bladder radiograph and ultrasonogram on postoperative day 1 and after 1 month. Complete clearance was defined as stone fragment <4 mm in size.
Results:
The mean operative time was 55 minutes (32–135 minutes). The commonly reported problems of long tract, difficulty in manipulation and hypermobility during tract dilatation were not encountered in any patient. Mean hemoglobin loss was 0.8 g/dL. None of the patients required blood transfusion. Nephrostomy tube was placed in selected patients with pelvic injury or previously treated infected hydronephrosis (7.9%). Complete stone clearance rate at 1 month was 93.1%.
Conclusions:
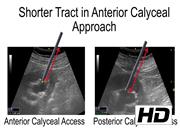
Anterior caliceal approach in supine PCNL has a shorter tract length when compared with posterior caliceal entry. Moreover, the problem of hypermobility is avoided because of good support from posterior abdominal wall muscles. Use of ultrasound helps in assessing the shortest and direct tract, which is mostly through an anterior calix.
No commercial associations during the past 3 years that might create a conflict of interest in connection with the video
.
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Runtime of video: 8 mins 37 secs


Get full access to this article
View all access options for this article.