
Abstract
Introduction and Objectives:
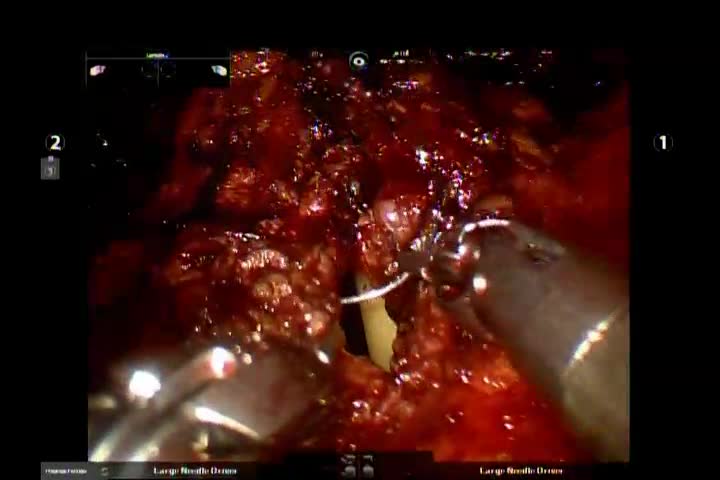
Bladder neck contracture and sexual dysfunction are associated with transurethral resection of the prostate for benign prostatic hyperplasia (BPH). Removing the obstruction without disrupting the prostatic urethra promises to improve the postsurgical quality of life of patients suffering from lower urinary tract symptoms caused by BPH by decreasing hematuria and preserving antegrade ejaculation. Our aim was to describe, in the accompanying video, the step-by-step approach for a robot-assisted urethra sparing simple prostatectomy (US-RASP).
Methods:
From January 2018 to March 2019, 10 consecutive patients who had undergone US-RASP were identified from our database. Procedures were performed as described stepwise in the accompanying video. In US-RASP, a 2.5 cm paraumbilical incision is made, a Veress needle is inserted and the peritoneal cavity entered. The peritoneal space is expanded using CO2 insufflation and a blunt ended camera port is inserted, enabling the placement of further three ports for robot docking. The bladder was opened longitudinally to identify the urethra and the median lobe followed by two longitudinal capsulotomies. Prostate adenoma is resected circumferentially while sparing the urethra in the midline. Electrocautery hemostasis is performed. The median lobe is pushed through the third arm to be resected through the same capsulotomies when needed. A 22F three-way catheter is placed. Anterior capsulotomy is closed in one layer using 3/0 V-loc suture. The bladder is closed in two layers using 3/0 V-loc suture. A drain is left in the retropubic space in cases of inadvertent urethral injury requiring repair. The patient is discharged usually on postoperative day 1 with the catheter in situ.
Results:
Of our 10 patients, median values were age 65 years (interquartile range [IQR]: 61.75–72) and median prostate volume measured by ultrasonography was 100 mL (IQR: 99.25–150). Median operative time was 135 min (IQR: 115–157.5). The median estimated blood loss was 150 mL (IQR: 100–150). Continuous bladder irrigation was avoided in all patients. The median time to catheter removal was 4.5 days (IQR: 3.75–7), with a median hospital stay of 1 day (IQR: 1–1.25). Clavien–Dindo complications were I (1) and II (2). Median resected prostate weight was 70 g (IQR: 60–103.75). Incidental prostate cancer was found in one patient and inadvertent urethral injury requiring repair (using 4-0 Vicryl) occurred in three patients. No patients were catheter-dependent postoperatively. At 12 months follow-up, median International Prostate Symptom Score and International Index of Erectile Function score were 8.5 (IQR: 7–10) and 19.5 (IQR: 16–22.75), respectively, median post-void residual was 23 mL (IQR: 10–25), and satisfactory anterograde ejaculation was reported in 7 patients (70%).
Conclusions:
We describe a robot-assisted technique to perform US-RASP. Our procedure, if validated, may add to the available methods to treat BPH and potentially reduce retrograde ejaculation and postoperative hematuria.
Acknowledgments: The author acknowledges and appreciates Dr. Sanjay B. Kulkarni for his review of the procedure in the video and his critical comments on the technique.
No competing financial interests exist.
Runtime of video: 9 mins 41 secs


Get full access to this article
View all access options for this article.