
Abstract
Introduction:
The overstretching of the posterior vaginal wall can cause a rectocele or enterocele. Although these defects can be asymptomatic, they often cause discomfort such as bulging or stool bulking. The defect can be managed by classic vaginal repair (posterior colporrhaphy) through suturing the pelvic fascia and often additionally the levator muscles. In the 19th century, Breisky (1879), Savage (1868), and Fritsch (1881) developed and adopted these strategies.
1
These techniques were performed until the late 1990s; some of them are still in use.
2,3
The application of the traditional approach decreased constantly after introduction of vaginal mesh surgery, until the Food and Drug Administration issued its warnings in 2008 and 2009 (
Methods:
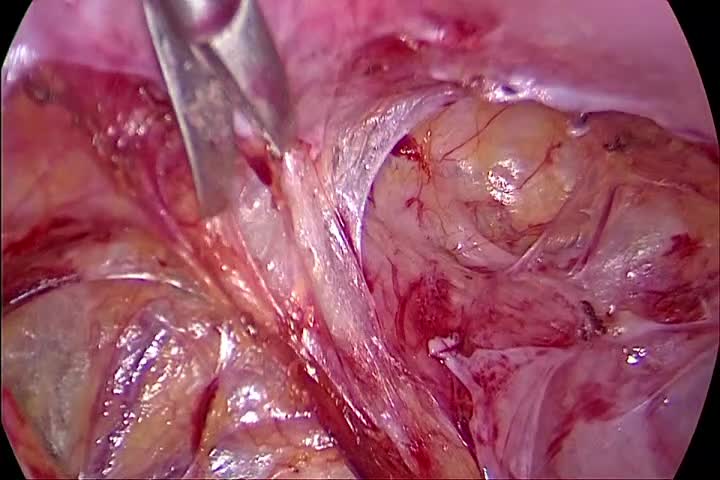
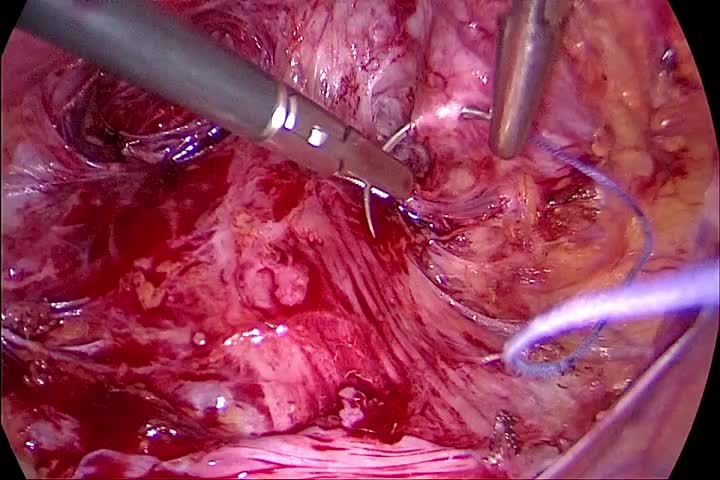
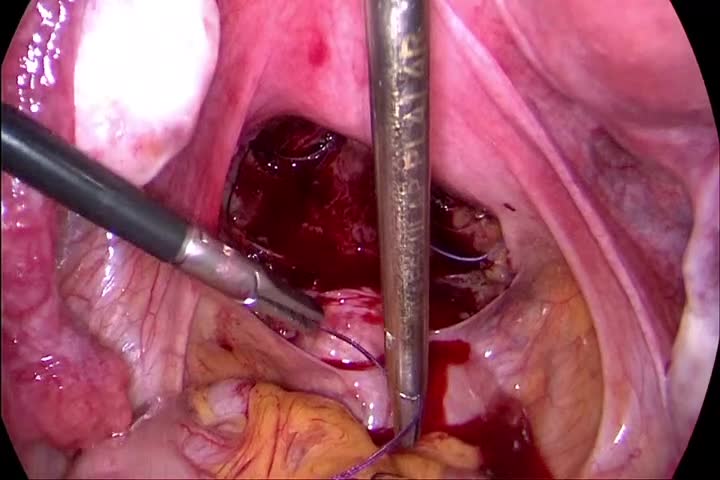
The video demonstrates the compression of the stretched posterior vaginal wall by performing the suturing laparoscopically. The fascia and vaginal mucosa are not divided and persist as one tissue layer. No tissue is resected and no vaginal scar results. The peritoneum is opened in the pouch of Douglas at the “fatty tissue” line. We use a bipolar grasper and a scissor for the dissection. The posterior vaginal wall is dissected down to the levator muscles, and the rectum is dissected to its entrance into the perineal body. We place a small clamp at the hymen area vaginally to mark the deepest preparation point. The fascia is sutured horizontally in an interrupted laparoscopic technique. We use a size 1 polyglycolic acid suture to provide firmness of the suture as well as a good stimulus for fibrozation. For the semicircular sutures, we take five to six bites to compress the tissue. While placing the deepest suture, the clamp at the hymen is pushed forward to ensure the deepest possible placement of the suture. The peritoneum is closed at the end of the procedure. In most cases, the approach is combined with an apical support procedure. We generally use the pectopexy to provide apical stability.
Results:
In a first examination series of 18 patients treated by posterior laparoscopic fascia repair, we detected one apical and two posterior relapse after 15 months. One patient had complaints related to the rectocele and received a reintervention. No pain, defecation disorders, or dyspareunia occurred. If the perineal body has to be narrowed, an additional vaginal access is needed. The video demonstrates the technique step by step.
Conclusions:
The combination of laparoscopic apical support surgery with native tissue repair by one route is feasible. As only one workspace is necessary, fewer instruments are needed and no time is lost due to change of setting, gloves, and so on. As no scars in the vaginal tissue result, the acceptance especially in younger women is very high. However, long-term follow-up date should be obtained before recommending this technique for daily use?
No competing financial interests exist.
Author(s) have received and archived patient consent for video recording/publication in advance of video recording of the procedure.
Runtime of video: 6 mins 11 secs
Get full access to this article
View all access options for this article.