
Abstract
Introduction:
The morbidities associated with transperitoneal route for robot-assisted radical prostatectomy are postoperative ileus and potential bowel injuries. The extraperitoneal approach avoids the peritoneal cavity and potential associated morbidity. We report our technique and the perioperative and short-term postoperative outcomes of our series.
Materials and Methods:
Between May 2016 and April 2017, 15 consecutive patients who met inclusion criteria (body mass index [BMI] < 30, D'amico low- to intermediate-risk prostate cancer, prostate volume <60 mL, and no previous laparotomy) were recruited prospectively. The extraperitoneal space was created posterior to the subumbilical rectus sheath in the preperitoneal fat plane with a balloon dissector. A five- to six-port technique was used with reduced Trendelenburg angle. Antegrade dissection of prostate was performed. Vesicourethral anastomoses were by the Velthoven technique with modified Rocco's stitch. Patient demographics, characteristics, and peri- and postoperative short-term outcomes were analyzed.
Results:
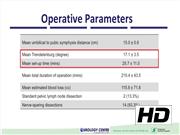
The median age was 64 (range 57–70) years and mean prostate volume was 46.3 ± 12.0cc. The mean prostate specific antigen (PSA) was 7.5 ± 2.8 µg/L. The mean BMI was 23.8 ± 2.2 kg/m2. All 15 patients underwent extraperitoneal approach effectively. The mean umbilical to pubic symphysis distance was 15.0 ± 0.8 cm. The mean setup time (creation of extraperitoneal space and robot docking) was 25.7 ± 11.0 minutes and mean total operative time was 215.4 ± 43.5 minutes. The mean Trendelenburg degree was 17.1 ± 3.5. Mean estimated blood loss was 115.8 ± 71.8 mL. There was a small peritoneal breach during balloon dilatation in a patient with previous open appendicectomy and another with previous open hernia repair. Two (13.3%) and 14 (93.3%) patients had standard pelvic lymph node and nerve-sparing dissections, respectively. Postoperatively no patients had ileus, intraabdominal, or other significant Clavien–Dindo complications. Thirteen (86.7%) patients passed flatus and had diet on postoperative day (POD) 1. Nine (60.0%) patients were discharged within 24 hours and the rest on POD 2. All patients received paracetamol 1 g when needed, whereas four required single dose intramuscular pethidine for breakthrough pain. Pathologic stage was pT0, pT2a, and pT2c in 1 (6.7%), 12 (80.0%), and 2 (13.3%) patients, respectively, representing downstaging in 1 (6.7%, pT0 in the prior-transurethral resection of prostate patient). One patient had focal (<1 mm) positive margins (anterior apical) with the majority (93.3%) having complete resection. At a mean of 126 ± 85.7 days, 14 patients (93.3%) achieved undetectable nadir PSA (<0.03 µg/L). Overall continence rate was 86.7% at 3 months. The follow-up duration was not long enough to meaningfully report recovery of erectile function.
Conclusion:
Total extraperitoneal resection of prostate, an extraperitoneal organ, in selected patients enables ileus-free early discharges.
No competing financial interests exist.
Runtime of video: 6 mins 49 secs


Get full access to this article
View all access options for this article.