
Abstract
Introduction:
There are multiple fluoroscopic puncture techniques described to perform percutaneous nephrolithotomy. However, to our knowledge, there is still no standardized puncture technique. Our objective is to present the description of a modified biplanar technique of 0–90° puncture for percutaneous nephrolithotomy effectiveness and outcomes. 1
Methods:
We performed a retrospective review of 136 patients operated with our modified 0–90° puncture technique (Escovar–Leon modification) for percutaneous nephrolithotomy between 2015 and 2018. A descriptive statistical analysis was performed in SPSS; for the description of the effectiveness, outcomes, and safety, we divided all patients in relation to stone complexity with nephrolithometric scoring systems Guy, STONE, and Clinical Research Office of the Endourological Society (CROES). Guys score, 2 STONE score, 3 and nephrolitometric nomogram CROES, 4 are scores by which each one evaluates the complexity of the stone, as well as the percentage of stone-free rate after one treatment with percutaneous nephrolithotomy. In the case of the STONE score system, this predicts the risk of post-operative complications after a percutaneous nephrolithotomy. To assess stone-free rate, a CT scan was performed in all patients; residual stone was defined as stone >2 mm. Complications were divided according to the Clavien–Dindo classification.
Results:
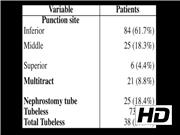
One hundred thirty-six patients with an overall age of 44.36 ± 13.23 years were punctured with our modified puncture technique: 51 were men and 85 were women. In 121 patients, nephrolithotomy was performed in Valdivia–Galdakao position and 15 in prone position. Global stone-free rate was 62.5%, stone-free rate regarding stone complexity was in GUYS I (95%), GUYS II (74.3%), GUYS III (37.9%), GUYS IV (25%), STONE with a low complexity 86.6%, moderate complexity 73.2%, and high complexity 40%, and in relation to CROES score low complexity 84.2%, moderate complexity 51.9%, and high complexity 37.03%. The mean fluoroscopy time was 69.47 ± 7.1 seconds. Nephrostomy tube was used in 25 (18.4%) patients, tubeless in 73 (53.3%) patients, and total tubeless in 38 (27.9%) patients. Mean operative time was 128.9 ± 59.09 minutes and hospital stay was 2 days. Patients with a single tract in inferior, middle, or superior calix were 84, 25, and 6 respectively, in 21 (8.8%) patients, multitract was performed. Complications were present in 25.7% of all patients and were graded according to the Clavien–Dindo classification. There were grade 1 (13.2%), grade 2 (11%), grade 3 (1.5%) complications but no grades 4 and 5. The overall stone-free rate reaches 83.8% after an ancillary procedure.
Conclusion:
In our experience, this novel technique allowed low fluoroscopy time, was effective and safe concerning stone-free rate, and maintained a low complications profile. Despite we having no puncture failures, novice urologists could need a learning curve, and could have some puncture failures at the beginning.
No competing financial interests exist.
Runtime of video: 5 mins 55 secs

Get full access to this article
View all access options for this article.