
Abstract
Introduction and Objective:
The advancement of robotic technology has revolutionized surgical treatment for prostate cancer. Although the robot has facilitated surgery in narrow working spaces, it still has its shortcomings such as the collision of robotic and laparoscopic instruments both inside and outside the patient. Magnetic anchoring and guidance system (MAGS) technology provides extra tools within the patient without the use of additional trocars or bulky instruments. MAGS has not yet been described in robotic urologic surgery.
Methods:
We present two robotic urologic cases in which we used a magnetic retractor device. The magnetic retractor is inserted through the air seal trocar and deployed with a laparoscopic handheld device by the bedside assistant. The retractor is then coupled to a handheld magnet that is placed outside of the patient's abdominal wall in the desired position. The device is designed for use in patients of body mass index between 20 and 34 kg/m2. Although the external magnetic controller is reusable, the handheld device and the detachable tip are disposable. The first case is a 56-year-old man who was found to have Gleason 7 prostate cancer on prostate biopsy. He elected for nerve-sparing robot-assisted laparoscopic prostatectomy (RALP). The second case is a 56-year-old man with recurrent urinary tract infections and a history of transurethral microwave thermotherapy of the prostate who presented with two large bladder diverticula. He elected for a transurethral button vaporization of the prostate and robot-assisted laparoscopic bladder diverticulectomy (RABD) in the same operative setting.
Results:
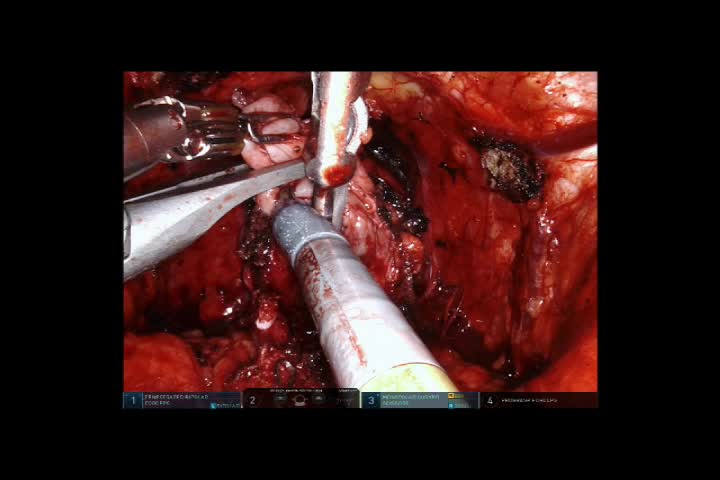
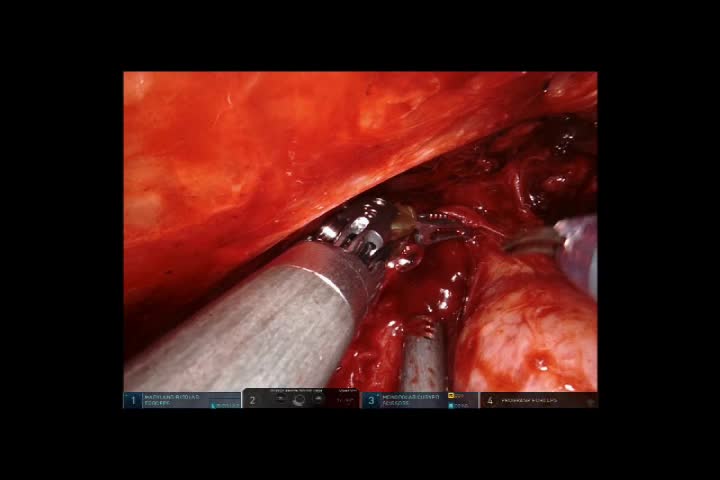
In the RALP, the magnetic retractor provided anterior retraction of the vasa deferentia during the dissection of the seminal vesicles. The magnetic retractor was then used to retract the vasa and seminal vesicles to facilitate posterior dissection of the prostate, whereas the fourth robotic arm provided cephalad retraction of the bladder. During the dissection of the neurovascular bundles and prostatic pedicles, the magnetic retractor was helpful in pulling the prostate medially without the use of the fourth robotic arm. There were no intraoperative complications. In the RABD, the magnetic retractor was used for additional retraction of the bladder in angles that the robotic fourth arm was not able to provide. There were no intraoperative complications.
Conclusions:
The use of a magnetic retraction device facilitates certain steps in RALP and may be useful in other robotic urologic surgeries.
No competing financial interests exist.
Runtime of video: 5 mins

Get full access to this article
View all access options for this article.