
Abstract

Introduction:
Arteria lusoria identification during preoperative imaging evaluation indicates the right nonrecurrent laryngeal nerve (RNRLN).1–3 Toniato et al. classified the RNRLN anatomy into three types. 4 However, these types cannot be predicted on preoperative imaging evaluation 2 and require surgery to ensure identification, consequently leading to challenges in RNRLN identification and preservation. Intraoperative neuromonitoring (IONM; NIM-Response 3.0; Medtronic Inc., Minneapolis, MN, USA) is commonly used in thyroid and parathyroid surgeries to prevent recurrent laryngeal nerve injury and confirm its anatomical and functional preservation. RNRLN identification and preservation may be more difficult in endoscopic thyroidectomy than in conventional surgery from the neck incision because of limited vision, despite the applicability of IONM.
Materials and Methods:
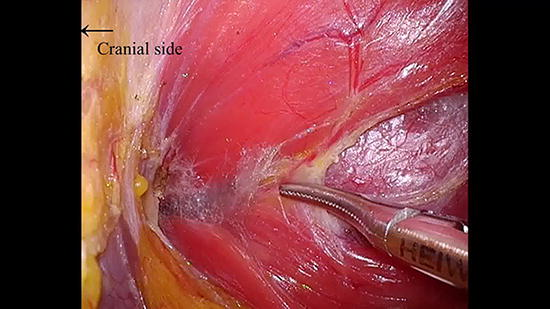
We created a 4-cm and 5-mm incision in the subclavian area and neck of the endoscope, respectively. A mistless video-assisted neck surgery (VANS) retractor (Hakko, Tokyo, Japan) was placed through the 4-cm incision in the subclavian area to lift the skin flap, while the thyroid gland was approached through the small supraclavicular fossa. In contrast, the lateral technique, involving an approach from the medial margin of the sternocleidomastoid muscle (SCM), was used in the original VANS method. 5 In this procedure, SCM may obstruct the internal jugular vein and carotid artery exposure due to limited vision during endoscopic surgery. However, in the present approach, the internal jugular vein and carotid artery were easily identifiable after cutting the omohyoid muscle. The vagus nerve was identified longitudinally between the internal jugular vein and carotid artery. IONM stimulation of the vagus nerve was used to indicate the RNRLN branching point. However, a negative IONM response along the vagus nerve indicates type 1 RNRLN according to Toniato’s classification. 4 In type 1 RNRLN cases, the nerve runs along the superior thyroid arteries, and researchers should further explore this region. Conversely, in type 2A or 2B RNRLN cases, the point of IONM response change was identified as the RNRLN branching point from the vagus nerve. A small supraclavicular fossa approach to the thyroid gland exposed the internal jugular vein, carotid artery, and vagus nerve. Therefore, after confirming the RNRLN branching point from the vagus nerve, RNRLN was easily identified and preserved, as in cases without an RNRLN.
Results:
In our modified technique, the RNRLN anatomy was identified during the surgery. Using IONM, surgeons can identify the RNRLN branching point from the vagus nerve because positive to negative IONM response change to vagus nerve stimulation can indicate this branching point. 6 This technique requires longitudinal exposure of the vagus nerve over a long distance. Furthermore, the small supraclavicular fossa approach in the VANS method can provide the required field of vision despite the limited working space during endoscopic thyroidectomy.
Conclusion:
Applying the small supraclavicular fossa approach in the VANS method can facilitate the identification of the RNRLN branching point from the vagus nerve and minimize the risk of RNRLN injury.
Authors’ Contributions
: T.H. acquired the data, interpreted the results, and drafted the article; T.H., Y.H., and T.I. acquired the data; K.F., M.O., N.G., Y.W., S.N., and Y.T. interpreted the results. All authors approved the final version of the article.
Author Disclosure Statement
: The authors declare no conflicts of interest for this article.
Funding Information
: No funding was received for this article.
Runtime of video: 7 min 18 sec.
Keywords
Get full access to this article
View all access options for this article.