
Abstract
Introduction:
Multinodular goiter (MNG) can be a challenging pathology owing to its large size and possible significant airway deviation and compression. To secure the airway in such cases, awake fiberoptic intubation is recommended, but limitations include patient distress and varying success owing to operator skill. Therefore, veno-venous (V-V) Extracorporeal membrane oxygenation (ECMO) can be used as a backup for patients with severe tracheal stenosis due to a large MNG.
Materials and Methods:
We describe our technique for V-V ECMO cannulation followed by thyroidectomy and successful intubation. We also include four patients requiring prophylactic V-V ECMO for a large MNG presenting with extreme airway compression.
Results:
Four patients with severe critical tracheal stenosis underwent thyroidectomy at Emory University requiring prophylactic ECMO cannulation. Two patients required only wire access and were successfully intubated. The other two patients required V-V ECMO and thyroidectomy followed by fiberoptic intubation and bronchoscopy.
Technique.
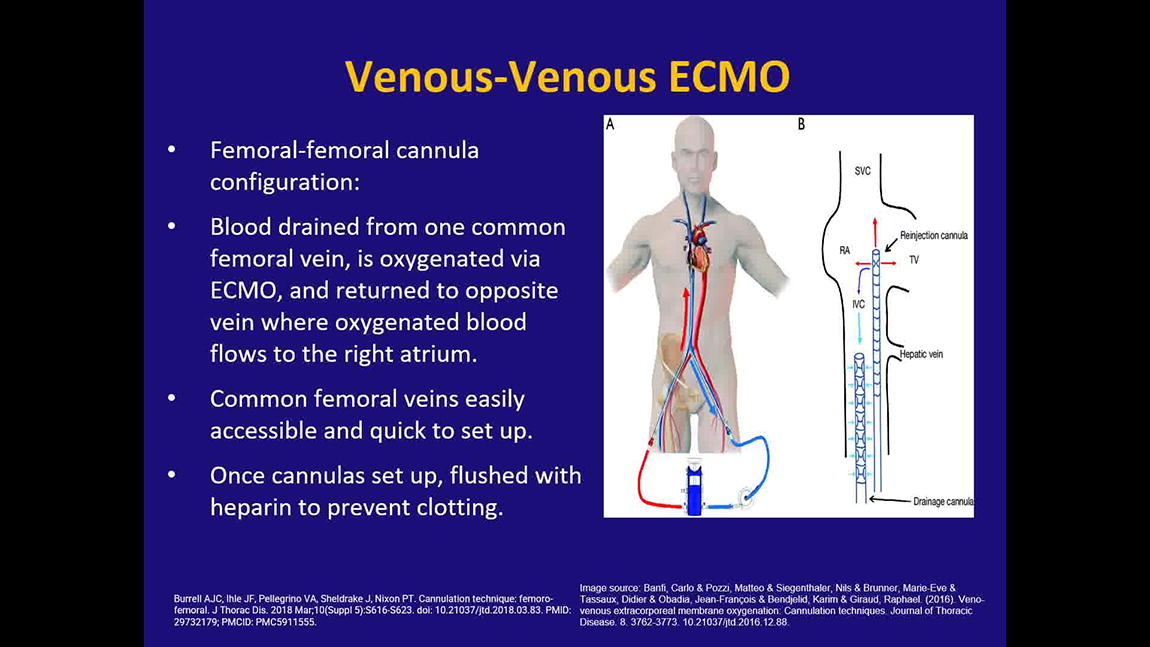
Cardiac surgery places wire access using ultrasound guidance of the right and left femoral veins with fluoroscopy. Fiberoptic intubation can be attempted, and if unsuccessful, V-V ECMO cannulas are inserted. Once V-V ECMO cannulas are placed, they are flushed with heparin, and the circuit is initiated. Surgeon begins the thyroidectomy with the patient on ECMO. After completion of the thyroid lobectomy, the tracheal compression is relieved. Anesthesia intubates with bronchoscopy and confirms that the compression is relieved. V-V ECMO cannulas are removed, and heparin is reversed with protamine. The neck incision is closed, and the patient is extubated.
Conclusion:
Large MNG with severe tracheal stenosis pose a challenging problem for successful intubation. Awake fiberoptic intubation can be limiting as it is distressing to the patient, and its success depends on patient tolerance and operator skill. Patients with severe critical tracheal narrowing have no backup to failed awake fiberoptic or rigid bronchoscopy. Prophylactic V-V ECMO provides a solution for the difficult airway and requires a multidisciplinary approach.
Disclosure Statement: No financial disclosures or conflicts of interest.
Runtime of video: 5 mins 25 secs
Get full access to this article
View all access options for this article.