
Abstract
Introduction:
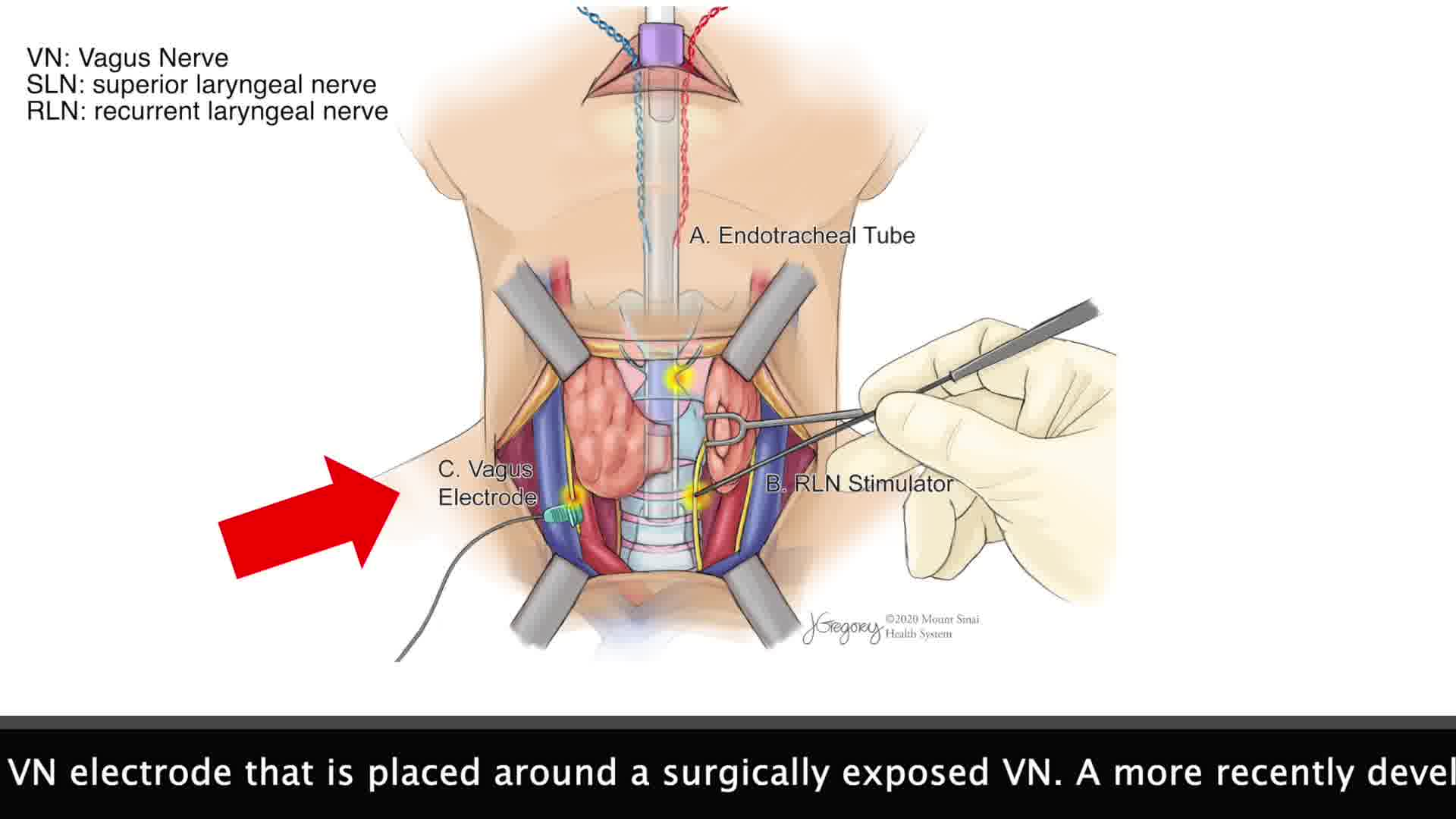
In neck endocrine surgeries, the recurrent laryngeal nerve (RLN) is at risk of injury, requiring reliable monitoring methodologies. 1 This video explains the integration of intermittent and continuous nerve monitoring, focusing on the laryngeal adductor reflex (LAR), 2 a noninvasive technique to assess RLN, vagus nerve, and superior laryngeal nerve integrity during surgery. 3
Materials and Methods:
Two main forms of nerve monitoring—intermittent and continuous (CIONM)—are currently employed. The noninvasive tube-based LAR technique offers real-time feedback without operative exposure or additional devices. A specialized endotracheal tube (NIM EMG ® Medtronic Xomed Inc., Jacksonville, FL, USA) is used for LAR stimulation and recording. For LAR elicitation, one pair of stainless-steel wire electrodes integrated in the tube are connected to the stimulating box delivering a single or short train of electrical pulses up to 25 mA intensity, 0.5–1 ms duration at 0.4 Hz rate. For LAR recording, the contralateral pair of wire electrodes are connected to the amplifier box. To optimize our recordings, one bipolar and two monopolar derivations were utilized (i.e., V+/V−; V+/Reference; V−/Reference). Direct nerve stimulation with a hand-held probe (mapping) at 0.5–0.8 mA intensity (0.2 ms duration) at 4 Hz rate aids in nerve localization, identification, and integrity. All electrophysiologic LAR stimulation and recordings were made using a Medtronic Eclipse® system (Medtronic Xomed, Inc.). The institutional review board of the Icahn School of Medicine at Mount Sinai Hospital approved this study (STUDY-23-01728).
Results:
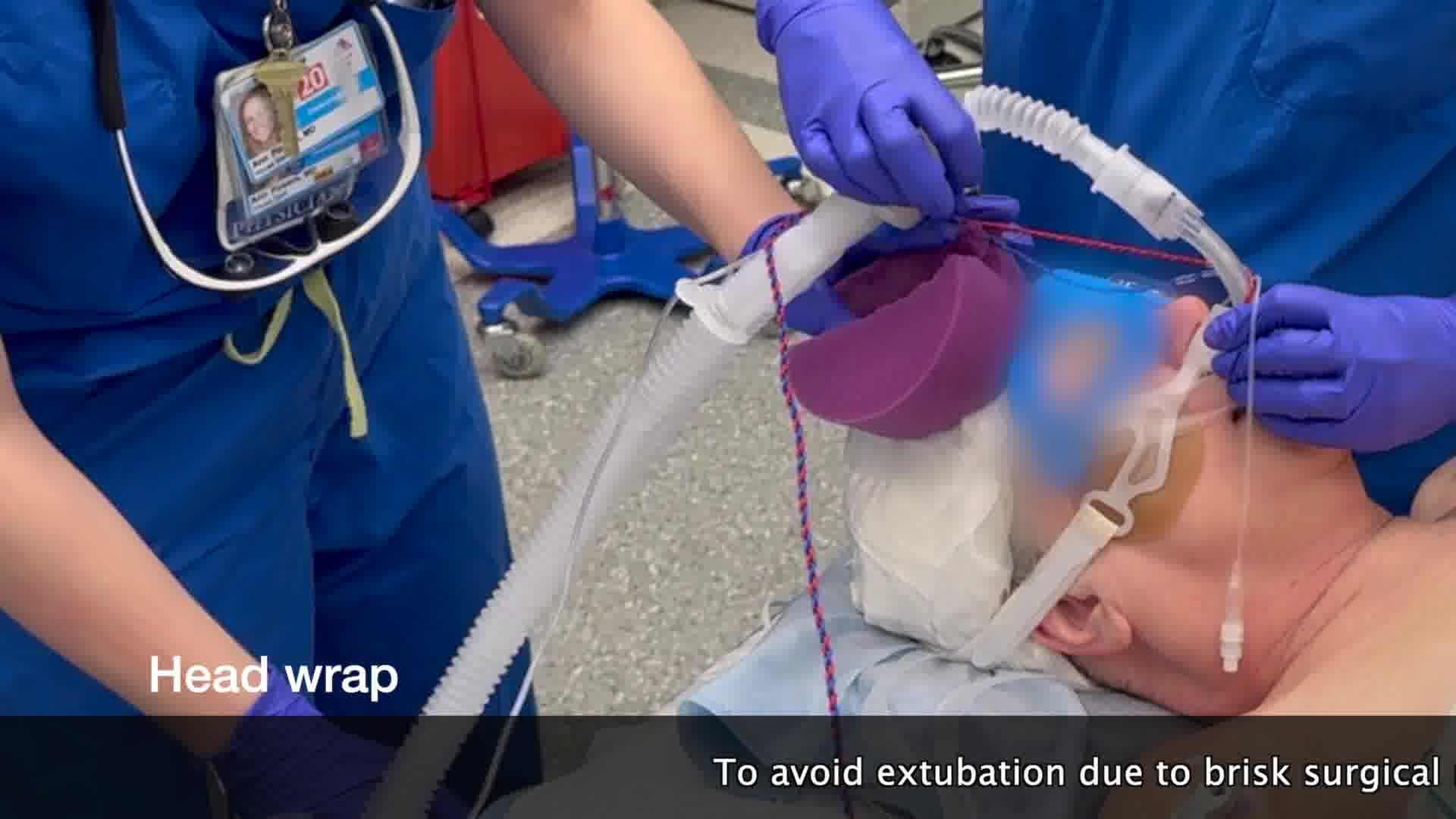
The video illustrates the intubation process under video laryngoscope observation (GlideScope, Verathon Inc., Seattle, WA, USA), emphasizing the importance of maintaining optimal electrode contact with laryngeal structures. The setup, positioning, and tube fixation procedures (Anchor-Fast™, Libertyville, IL, USA) are detailed. The characteristics of the LAR recordings are described. LAR preskin incision opening baselines provide reference values crucial for monitoring during surgery. Surgical approaches are discussed, emphasizing constant communication between surgeons and neurophysiologists during RLN localization and dissection. The LAR technique aids surgeons in timely corrective actions when intraoperative changes in nerve signals occur. Previous studies have shown that the LAR methodology presents high specificity, presenting no false negatives.4–9 Therefore, if the LAR is stable as the surgery is advanced, the surgeon can be confident that the RLN's integrity and function are preserved. While adding costs by the neurophysiologist participation, the potential benefits in enhancing patient safety justify this approach.
Conclusions:
This study emphasizes the advantage of combining intermittent mapping with LAR-CIONM over mapping alone in challenging scenarios, such as revision surgery. LAR-CIONM offers continuous real-time assessment of laryngeal nerve function without operative nerve exposure, but its success depends on optimal endotracheal tube positioning and expert neurophysiologist support. The study discusses prospects, anticipating improved monitoring with dedicated advanced EMG endotracheal tubes, and dedicated machine programming.
No authors have conflicts of interest in connection with the video.
Runtime of video: 11 mins 00 secs
Get full access to this article
View all access options for this article.