Abstract
Introduction:
Many patients with anaplastic thyroid cancer (ATC) present with vocal cord paralysis. Patients with BRAF-mutated ATC have been shown to have rapid and dramatic responses to BRAF/MEK inhibitor with immunotherapy.1–5 These rapid and dramatic responses have been associated with recovery of vocal cord function, as has been recently reported in a multi-institutional case series in the literature. 6 Herein we demonstrate pre- and post-treatment positron emission tomography (PET) scans and video laryngoscopies in a series of patients with BRAF-mutated ATC who had recovery of nerve function after treatment with BRAF/MEK inhibitor and immunotherapy.
Methods:
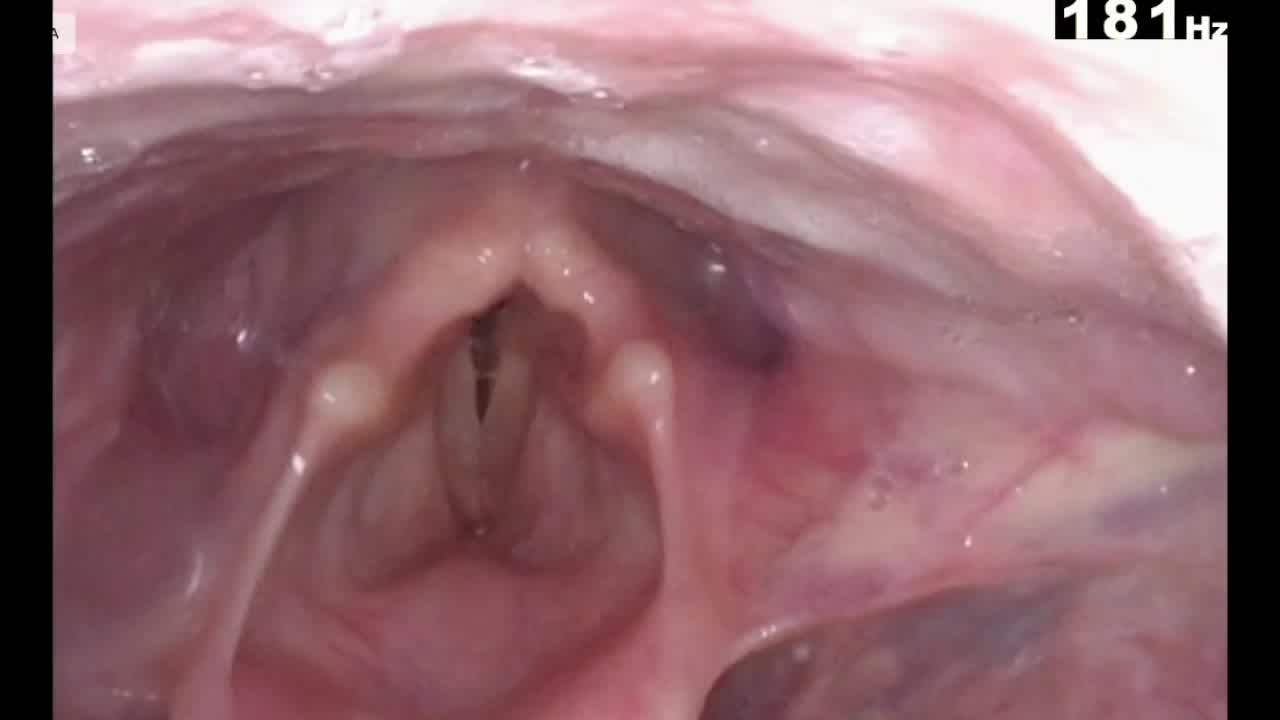
We present a case series of five patients with BRAF-mutated ATC who presented with either unilateral (four patients) or bilateral (one patient) vocal cord paralysis/paresis. Pre-treatment and post-treatment video laryngoscopies, and pre-treatment and post-treatment PET scans were performed for each patient.
Results:
All five patients presented with significantly locoregionally advanced ATC, as demonstrated by pre-treatment PET scans. Pre-treatment videostroboscopy was performed on all patients, displaying two with right vocal cord paralysis, two with left vocal cord paralysis, and one with bilateral vocal cord paresis. All patients underwent BRAF/MEK inhibitor with immunotherapy, with 3 (range 2–22) months median duration of therapy, followed by post-treatment PET imaging and video laryngoscopy. All five post-treatment PET scans showed complete or near-complete resolution of PET avid disease in the neck. Postneoadjuvant therapy video laryngoscopy demonstrated return of vocal cord function in all patients. All five patients proceeded to surgery after neoadjuvant therapy, wherein all patients had significant desmoplasia and fibrosis partially encasing the recurrent laryngeal nerve(s). Of the six nerves that were initially paretic and recovered function after neoadjuvant therapy, all were anatomically preserved during surgery. Intraoperative intermittent neural integrity monitoring (NIM) of these six nerves revealed the following: two nerves initially stimulated but lost stimulation during dissection, whereas four nerves did not ever stimulate at any time during the procedure. Flexible laryngoscopy of the six affected vocal cords postsurgery revealed the following: five vocal cords were mobile and one remained pending evaluation.
Conclusions:
Given that ATC represents an extremely fast-growing malignancy, and initial nerve paralysis/paresis may be reversible with rapid initiation of therapy with rapid disease response. With BRAF-mutated ATC, BRAF/MEK inhibitors with immunotherapy have been demonstrated to induce these rapid and dramatic responses in many patients. This allows for the possibility of nerve recovery in some patients if nerve compression and/or early nerve invasion is quickly reversed.
IRB approval:
This research was conducted after MD Anderson Cancer Center IRB approval and patient consent was waived.
M.E.C. receives Bayer, Exelixis, Lilly advisory board/consulting fees and grant funding from Merck, Genentech:. K.H. has funding from the PCORI, NIH/NIDCR, NIH/NCI, Atos Medical, Charles and Daneen Stiefel Fund, DOD, and MD Anderson Institutional Research Grant Program. C.B. has funding from MD Anderson Internal Research Grant and NIH/NCI. R.D. has research support from Exelixis, Eisai, Merck, AstraZeneca; consulting fees from Exelixis, Bayer. N.L.B. has research funding from Novartis; is on ad board of Eisai; and consultant of Exelixis. M.E.Z. has clinical trial research funding to MD Anderson Cancer Center from Merck and Eli Lilly. E.E.H., S.H.S., P.C.I., J.R.W., and A.M. have no disclosures.
One of these five patients in this case series was recently published as a Letter to the Editor in Thyroid (reference included herein) as part of a multi-institutional case series (six patients total). This recently published Letter to the Editor did not include pre-/post-treatment video laryngoscopies or pre-/post-treatment PET scans. This current case series submitted to VideoEndocrinology includes an additional four patients, plus one patient included in the aforementioned multi-institutional case series. We could not include three other patients from MDACC who were included in the recent multi-institutional series, as they did not have pre- and post-treatment video laryngoscopies, which we feel is essential for this video article.
Runtime of video: 7 mins 43 secs