
Abstract
Introduction:
Radiofrequency ablation (RFA) is an ultrasound-guided thermal ablative technique that uses high-frequency alternating current to raise tissue temperature and cause tissue necrosis and fibrosis. 1 RFA is increasing in popularity as a safe and effective method for the treatment of benign thyroid nodules.1–10 Benefits of this technique are minimizing risks inherent to thyroid surgery; most importantly greatly reducing the risk of recurrent laryngeal nerve and parathyroid gland injury and the need for thyroid hormone supplementation postprocedure.5,11–14 It also avoids the use of general anesthesia for high-risk patients. 5 Other advantages include decreased pain, absence of scar, and ability to be performed in the outpatient setting. As RFA is becoming a more acceptable treatment modality, this project aims to show how RFA can be carried out in an outpatient setting and that it is a safe and effective method for the management of benign thyroid nodules.
Methods:
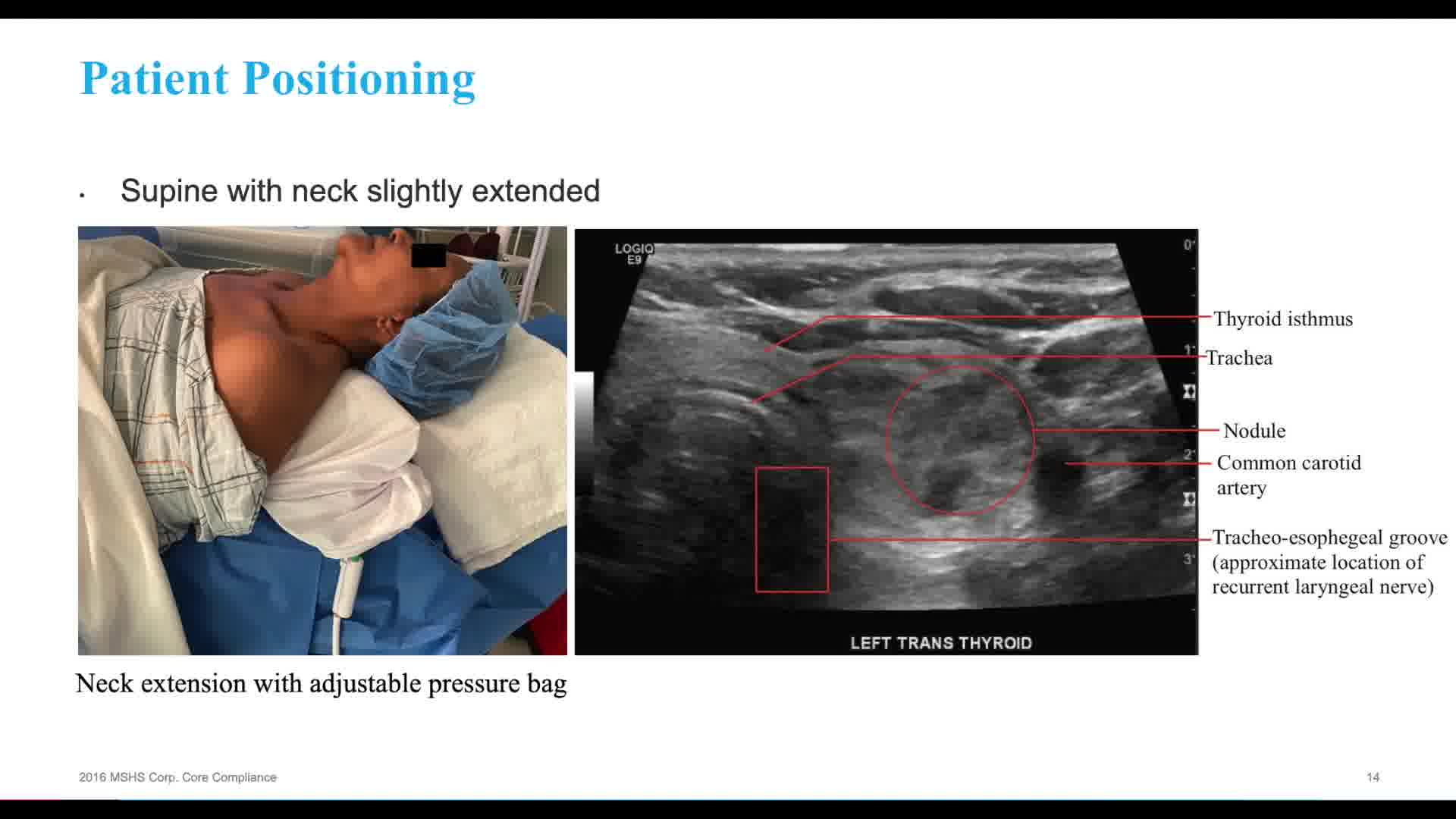
After Institutional Review Board approval, we enrolled patients seen in the endocrine surgery practice with symptomatic benign nodules both nonfunctioning and autonomously functioning. Exclusion criteria were age <18 years, history of thyroid malignancy, malignant findings on biopsy, indeterminate nodules on biopsy (Bethesda 3 or 4), and those unable to provide informed consent. Patients who met these criteria were presented with the option of being evaluated for RFA. Interested patients were referred to the RFA clinic. Ultrasound images were obtained in the office; thyroid function tests and relevant studies including prior ultrasounds and biopsy results were reviewed. Informed consent was obtained. All procedures were performed in the office. Patients were prepped and draped in standard sterile manner. Local anesthetic was injected. RFA probe size was selected based on nodule size. Communication between the patient and surgeon was maintained to assess comfort level with the procedure. At the conclusion of the procedure, patients were monitored for 30 minutes and discharged from the office with a plan to return within 2 weeks and serial follow-ups at 2-, 6-, 9-, and 12-month intervals.
Results:
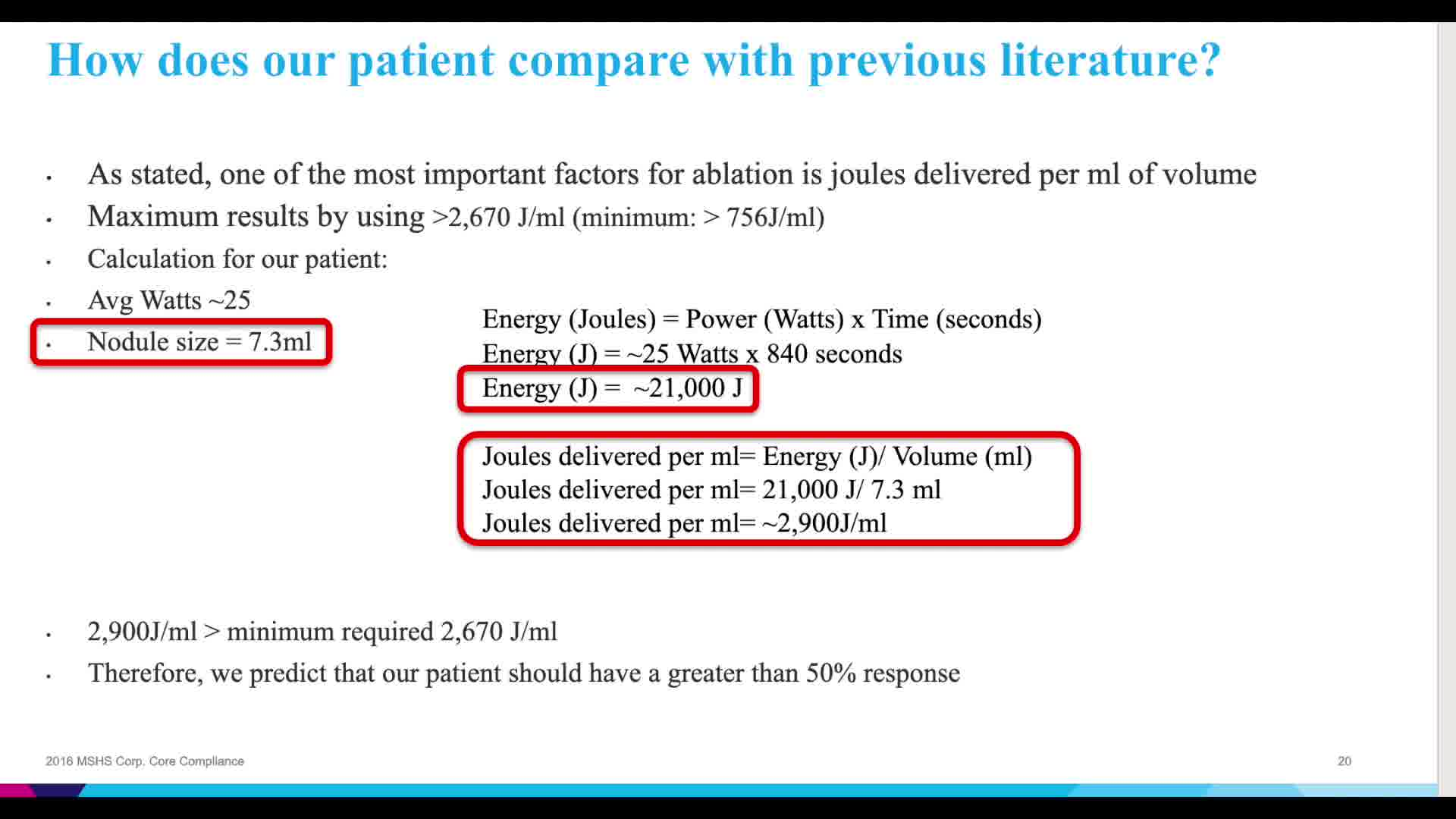
Our video presentation illustrates the tools and steps for performing RFA and highlights one patient's experience. The results for this patient were quite promising. The initial calculated volume of her thyroid nodule was 7.33 mL. At her follow-up visit at 2 weeks, the calculated volume was 3.41 mL and the relative reduction of the nodule was 53.5%. At 6 weeks, the nodule measured 2.46 mL and the calculated reduction was 66.4%. There were no acute complications. The only complaint was minor pain after the procedure that resolved with an ice pack before leaving the office. More data are currently being collected as to the durability of these results and long-term patient outcomes.
Conclusion:
RFA can be implemented as an alternative to thyroid surgery for benign nodules in an office-based setting. Patients report satisfaction with the procedure;15,16 decreases in nodule size can be dramatic. Further data are currently being collected as to the durability of the results and long-term patient outcomes.
Source of Work/Study:
This is an IRB-approved prospective study at Mount Sinai hospital. Patients who are deemed candidates to participate are all offered to participate. Risks, benefits, and alternatives are explained to each patient and informed consent is obtained from each patient.
We have no financial disclosures or conflicts of interest. No competing financial interests exist.
Runtime of video: 11 mins 57 secs
Get full access to this article
View all access options for this article.