
Abstract
Background:
Lyme borreliosis (LB) remains a public health concern in France despite improved patient management and medical care. Stay-at-home restrictions during the COVID-19 pandemic, which affected participation in outdoor recreational activities and disrupted access to health care services, may have impacted the risk of developing LB.
Methods:
We analyzed data from two general practitioner networks in France (Sentinel Network and an electronic medical records database [EMR]) and the national hospital discharge database to describe LB epidemiology in 2020–2021 and compare it to previous years. Google Trends’ search volume was used to evaluate the association between the population’s interest in LB and the evolving epidemiology.
Results:
Annual LB incidence rates in primary care decreased from 104 cases/100,000 population in 2018 to 71/100,000 in 2021 and from 82/100,000 to 60/100,000 according to Sentinel Network and EMR, respectively. Google Trends’ search volume for “Lyme” followed a similar trend, one year earlier. Annual hospitalizations were stable from 2012–2019 (1.6/100,000 on average) and declined to 1.3/100,000 in 2020 and 1.1/100,000 in 2021. This decline was observed primarily in adults (e.g., 3.4/100,000 in 2017–2019 to 1.8/100,000 in 2020–2021 for 70–79 years of age). Changes in regional incidence rates in primary care from 2017–2019 to 2020–2021 ranged from −75% to 208%. Hospitalizations decreased in all regions except in Bretagne.
Conclusions:
The estimated LB incidence decreased in 2020 and 2021 compared with previous years but this change may not be related to COVID-19. The incidence decrease observed in primary care could result from reduced population interest in LB, leading to lower care-seeking behavior. The decrease in LB hospitalizations may be explained by changes in clinical practice. Surveillance systems are critical to understand the evolution of LB epidemiology. However, external factors impacting incidence estimates should be considered.
Introduction
Lyme borreliosis (LB) is an infectious disease caused by a bacteria belonging to the genus Borrelia transmitted to humans through the bite of an infected tick (Stanek et al., 2012). The most common clinical manifestation of LB is erythema migrans, a characteristic localized skin rash (Stanek et al., 2012). If not recognized or treated, more severe clinical manifestations may develop a few weeks or months after the tick bite as part of a disseminated disease profile. LB is a public health concern in France despite improved patient management and medical care.
Understanding the epidemiology of LB, including its distribution by age, sex, and geography, is necessary to identify populations at high risk and to optimize preventive programs to mitigate risks of infection. In Europe, the most recent LB incidence reported by surveillance systems ranged from <20 cases/100,000 population per year (e.g., Bulgaria, Croatia, and England) to >100/100,000 (e.g., Estonia, Lithuania, Slovenia, Switzerland) (Burn et al., 2023). However, heterogeneity in surveillance methods (e.g., passive/active, case definitions, testing methods, types of data collected, and overall representativeness) impacts the accuracy of incidence estimates (Nagarajan et al., 2023).
In France, national LB data can be derived from two main sources: (1) LB cases reported by a network of general practitioners across France as part of the Sentinel Network or Réseau Sentinelles (Réseau Sentinelles, 2021) and (2) national hospital discharge data from the Programme de Médicalisation des Systèmes d’Information (PMSI), which mainly reports disseminated LB requiring hospitalization (ATIH, 2021). Previous analyses of Sentinel Network and PMSI data have estimated the incidence of LB since 2009 and 2004, respectively (Septfons et al., 2019; Vandenesch et al., 2014).
More recently, we described LB incidence rates in primary care and hospital settings for 2010–2019, with a focus on 2017–2019, based on data from the Sentinel Network and PMSI and using for the first time data from electronic medical records (EMR) of an independent and larger network of general practitioners in France (Nuttens et al., 2023). Santé publique France publish annually the incidence estimates of LB extracted from the Sentinel Network and PMSI (Santé publique France, 2022). During 2010–2019, LB average annual incidence rates almost doubled, from 42.3/100,000 in 2010–2012 to 83.0/100,000 in 2017–2019, according to Sentinel Network estimates, before decreasing to 71/100,000 in 2021. EMR data show a similar trend (42.7/100,000 in 2010–2012 to 74.6/100,000 in 2017–2019). The LB hospitalization rate remained relatively stable between 1.6 and 1.8 hospitalizations/100,000 for 2012–2019. More recently, data published by Santé publique France indicated a decrease in 2020 and 2021 (Santé publique France, 2022). LB incidence rates peaked in children (i.e., 0–4 years for the Sentinel Network and 5–9 years for EMR and PMSI) and among older adults (i.e., 60–69 years for primary care and 70–79 years for hospitalizations). Geographic variability in LB incidence and hospitalization rates was also observed, with the highest LB incidence rates observed in Limousin and the north-eastern regions of France.
Although LB epidemiology has been well characterized in France, the most recent assessments were based on data from before the COVID-19 pandemic. As the COVID-19 pandemic had a considerable impact on the epidemiology of many infectious diseases, it is justified to analyze the most recent trends in LB epidemiology. In this article, we describe the evolution of LB epidemiology in primary care and hospital settings in France in 2020–2021 compared with previous years.
Methods
Data sources including epidemiological indicators
We used national LB data from three independent sources: the Sentinel Network, an EMR database from IQVIA, and the national hospital discharge data from PMSI. Further details on these data sources and the corresponding epidemiological indicators and time periods are provided in Supplementary Table S1 and have been published elsewhere (Nuttens et al., 2023). In addition, the relative search volume indicator from Google Trends was used for the keyword “Lyme.” Google Trends data can be used to analyze online interest in specific topics based on queries from Google search engine users.
Statistical analyses
The Sentinel Network provided estimates of LB incidence rates and 95% confidence intervals (CIs). LB incidence rates from EMR data were estimated using an extrapolation process similar to that used for the Sentinel Network data: for a given geographical area in mainland France, the average number of LB cases reported per general practitioner was multiplied by the total number of general practitioners and divided by the population (estimated by the National Institute of Statistics and Economic Studies). CIs were estimated assuming the number of reported cases followed a Poisson distribution. National incidence rates were calculated as the sum of all LB cases at the regional level divided by the national population. LB incidence rates were stratified by age group, region, and sex (EMR only). Patient-level data on hospital stays were used to calculate LB hospitalization rates by age group, sex, and region based on the place of residence of hospitalized patients (Nuttens et al., 2023). Since the PMSI database captures all hospitalizations in France, extrapolation and calculation of 95% CIs were not required. The average annual incidence rates of LB were calculated for multiyear time periods for data smoothing, i.e., to smooth the variability in annual data, allow for clearer patterns to emerge, and help identify differences during the study (e.g., 2017–2019 versus 2020–2021). The Method Of Variance Estimate recovery (MOVER) approach was used to construct 95% CIs (Donner and Zou, 2012)—these details were described previously (Nuttens et al., 2023). The male-to-female LB incidence rate ratio (IRR) was calculated by dividing the LB incidence rate in men to the LB incidence rate in women for the time period under observation. For the Google Trends analysis, monthly relative search volumes for the keyword “Lyme” from France between January 2004 and December 2022 were extracted, and the average annual relative search volume was calculated.
We used SAS software version 9.4 (SAS Institute; Cary, NC) to derive estimates of LB incidence rates in primary care and LB hospitalization rates. We used the R package, gtrendsR, (version 1.5.1) to extract Google Trends data on relative search volumes over time (Eddelbuette and Massicotte, 2022). We generated figures using R 4.2.1 (R Foundation for Statistical Computing; Vienna, Austria).
Ethical approval and consent to participate
This article analyzed previously collected data from general practitioner networks and the national hospital discharge database; no new studies involving human participants were performed. Therefore, Institutional Review Board approval and patient consent to participate were not required.
Results
Evolution of LB incidence and hospitalization rates in France
According to Sentinel Network estimates, the annual incidence rate of LB was stable from 2010 to 2014, started to increase in 2015, and peaked at 104/100,000 (95% CI, 91–117/100,000) in 2018. Subsequently, the rate decreased to 71/100,000 (95% CI, 60–82/100,000) in 2021, representing a decrease of 32% from 2018 (Fig. 1). Similarly, the annual incidence rate estimated from the EMR peaked at 81.8/100,000 (95% CI, 77.2–86.9/100,000) in 2018 and reached 59.9/100,000 (95% CI, 55.6–64.1/100,000) in 2021, representing a decrease of 27%. Using annual average incidence rates for 2017–2019 and 2020–2021, rate declines of 2.4% and 15.3% were estimated from the Sentinel Network and the EMR, respectively (Table 1).
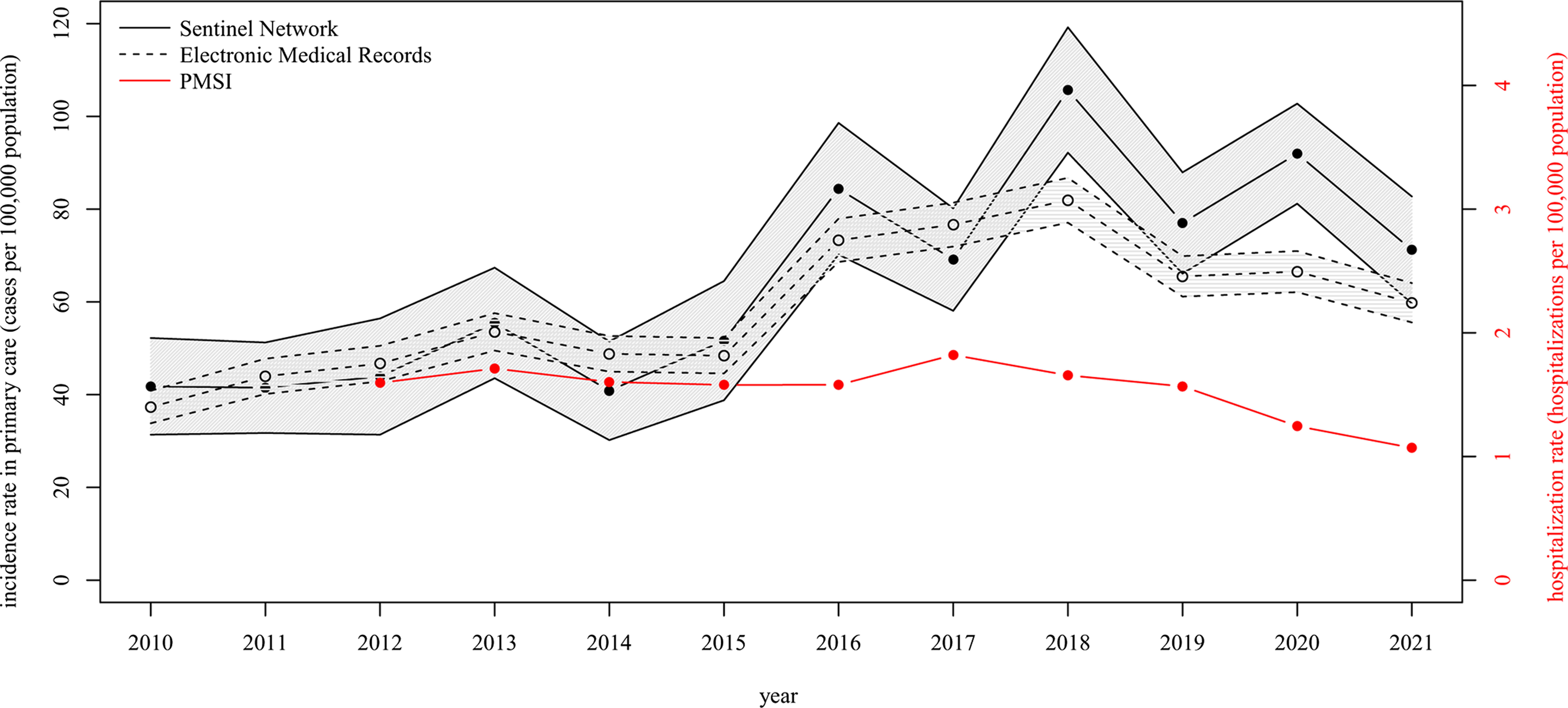
Evolution of LB incidence and hospitalization rates in France, 2010–2021. Annual rates reported as LB cases or LB hospitalizations per 100,000 population. Primary care incidence rates are extrapolated from the Sentinel Network and EMR data and hospitalization rates from P MSI data. The Y axes represent the incidence rate in primary care (left) and the hospitalization rate (right). Lower and upper 95% confidence intervals are provided for the Sentinel Network and EMR data. EMR, electronic medical record; LB, Lyme borreliosis; PMSI, Programme de Médicalisation des Systèmes d’Information (national hospital discharge database).
Average Annual Incidence and Hospitalization Rates (per 100,000 Population) and Number of Cases of LB in Primary Care (i.e., Sentinel Network, EMR) and Hospital (i.e., PMSI) Settings in France, 2017–2019 and 2020–2021.
Evolution of incidence rates between 2017–2019 and 2020–2021 has been expressed as relative difference (percentage).
CI, confidence interval; EMR, electronic medical record; IRR, incidence rate ratio; LB, Lyme borreliosis; NA, not applicable; PMSI, Programme de Médicalisation des Systèmes d’Information (national hospital discharge database); SN, Sentinel Network.
In comparison, annual LB hospitalizations were relatively stable from 2012 to 2019 (1.6 hospitalizations/100,000 on average) and declined to 1.3/100,000 in 2020 and 1.1/100,000 in 2021, representing a decrease of 32% between 2019 and 2021 (Fig. 1). Hospitalization rates decreased by 31.1% between 2017–2019 and 2020–2021 (Table 1).
Evolution of Google Trends’ search volume in France
Monthly and average annual Google Trends’ search volumes for “Lyme” in France are presented for 2004–2022 (Supplementary Fig. S1). Google Trends analysis of search volume for the keyword “Lyme” during 2010–2021 indicated a trend similar to that of LB incidence rates in primary care but preceding it by one year (Fig. 2). The search volume started to increase in 2014, peaked in 2017, and subsequently decreased by 29.7% between 2017 and 2020.

Evolution of LB incidence rates in primary care and Google Trends annual search volume for “Lyme” in France, 2010–2021. Annual incidence rates reported as LB cases per 100,000 population. Annual Google Trends search volume was calculated from monthly data, expressed as the relative percentage compared to the maximum volume over the study period. The Y axes represent the incidence rate in primary care (left) and the annual average search volume on a scale of 0% to 100% (right). Lower and upper 95% confidence intervals are provided for the Sentinel Network and EMR data. EMR, electronic medical record; LB, Lyme borreliosis.
When applying a lag of one year to the Google Trends data (i.e., using 2017 Google Trends data alongside 2018 LB incidence rates), the linear regression analysis indicated an R 2 of 0.74 for the Sentinel Network and 0.86 for the EMR data, suggesting that incidence rates of LB in primary care were highly correlated with the general population’s interest in Lyme disease (Supplementary Fig. S2).
Male-to-female incidence rate ratios
Male-to-female IRRs of LB were similar for 2020–2021 compared with 2017–2019 in the EMR and PMSI (Table 1). Slightly more women were seen in primary care settings (IRR = 0.84), whereas more men were hospitalized (IRR = 1.39).
Age-specific incidence and hospitalization rates
As observed for 2017–2019, the distribution of LB incidence rates by age group in 2020–2021 was bimodal, with peaks in children and older adults (Table 1). Compared with 2017–2019, LB incidence rates in 2020–2021 decreased in the pediatric and adolescent populations (0–19 years) in both primary care surveillance systems (−21.8% in the Sentinel Network and −13.5% in the EMR) (Table 1, Fig. 3). In the adult population, no decrease was observed for the Sentinel Network, and a 16.4% decrease was observed in the EMR data.

Average annual LB incidence and hospitalization rates by age group in France, 2017–2019 and 2020–2021. Annual average rates reported as LB cases or LB hospitalizations per 100,000 population in the age groups. Primary care incidence rates are extrapolated from Sentinel Network data and hospitalization rates from PMSI data. The Y axes represent the incidence rate in primary care (left) and the hospitalization rate (right). LB, Lyme borreliosis; PMSI, Programme de Médicalisation des Systèmes d’Information (national hospital discharge database); SN, Sentinel Network.
In contrast, the decrease in LB hospitalizations was observed among adolescents and adults but not in the pediatric population (Fig. 3). The decrease from 2017–2019 to 2020–2021 ranged from 24.5% in the 30–39 years age group to 46.2% in the 70–79 years age group (Table 1, Fig. 3). The comparison of individual years indicated the reduction observed in 2020 was restricted to persons ≥50 years old (Fig. 4). In 2021, hospitalization rates further decreased, starting in the 30–39 years age group and up to 60–69 years of age but remained stable in the 70–79 and ≥80 years age groups.

Annual LB hospitalization rates by age group in France for individual years, 2012–2021. Annual hospitalization rates reported as LB hospitalizations per 100,000 population in the age groups. LB, Lyme borreliosis; PMSI, Programme de Médicalisation des Systèmes d’Information (national hospital discharge database).
Regional variability in LB incidence rates
In 2020–2021, LB cases were reported in all regions of France, with important variability observed in regional incidence rates (Table 1). Across the three surveillance data sources, LB incidence and hospitalization rates in 2020–2021 were the highest in the Limousin (Sentinel Network: 416.0/100,000; EMR: 482.9/100,000; PMSI: 4.1/100,000), followed by Alsace (Sentinel Network: 306.0/100,000; EMR: 134.6/100,000; PMSI: 2.3/100,000). LB hospitalization rates in Center (2.1/100,000) and Bretagne (1.9/100,000) were relatively high compared with other regions but not their incidence rates in primary care (Table 1).
From 2017–2019 to 2020–2021, regional variability was observed in the evolution of primary care incidence rates, with either increases or decreases depending on the region, in both the Sentinel Network and EMR data (Fig. 5 and Table 1). During these two time periods, LB hospitalizations decreased in all regions except Bretagne, with notable declines in Poitou-Charentes (71.5%), Languedoc-Roussillon (58.7%), and Limousin (50.4%).

Evolution of average annual LB incidence and hospitalization rates (A = EMR, B = PMSI, C = SN) by region of France, 2020–2021 to 2017–2019. Annual rates (reported per 100,000 population) were averaged over the multi-year time period. Shades of blue indicate lower rates in 2020–2021 compared to 2017–2019, and shades of orange indicate higher rates in 2020–2021 compared to 2017–2019. EMR, electronic medical record; LB, Lyme borreliosis; PMSI, Programme de Médicalisation des Systèmes d’Information (national hospital discharge database).
Discussion
This study analyzed the epidemiology of LB for the period 2020–2021 and compared findings to 2010–2019, which we previously studied and published (Nuttens et al., 2023). We reported an increase in the LB incidence rate in primary care from 2015 and a stable hospitalization rate throughout the study period. In this analysis, we observed that LB incidence rates in primary care started to decrease in 2019, and the hospitalization rate decreased significantly in 2020 and 2021.
Collectively, these observations point toward a recent decline in the number of LB infections in France. This could be attributed to reduced contact with infected ticks during the lockdown periods of the COVID-19 pandemic or disrupted access to general practitioners and hospitals. In contrast, tick-borne encephalitis (TBE)—another tick-borne disease—increased during the COVID-19 pandemic in other countries in the European Union, and it was postulated that the population had more exposures to ticks outdoor recreation (Zając et al., 2022). However, this has not been clearly observed in France because of the low incidence of TBE (Santé publique France, 2023). In addition, the decrease of LB incidence rates started slightly before the COVID-19 pandemic, at least in primary care, and continued in 2021 despite reductions in stay-at-home restrictions and a return to normal access to health care services. The Sentinel Network recently published incidence estimates for 2022 showing a continued decrease to 51 cases/100,000 population (Réseau Sentinelles, 2022) and crude PMSI data from 2022 and 2023 indicate a similar trend (ATIH, 2023). If the decrease in LB incidence resulted from the COVID-19 pandemic, we likely would have observed an increase in LB incidence in 2022. Another explanation for decreasing trends in LB incidence in primary care and in hospitalizations could be the increasing adherence to preventive methods, such as removing ticks rapidly and wearing clothes that cover arms and legs.
The reduction in LB cases could also be explained by alternative hypotheses, unrelated to COVID-19. It has been previously postulated (Nuttens et al., 2023) that the “Plan Lyme,” an initiative from the health authorities launched in autumn 2016 to improve patient management and medical care, increased the knowledge and interest of LB in the general population and resulted in an increase in LB incidence rates because of its impact on primary care-seeking behavior, as identified through the primary care surveillance systems. To test this hypothesis, data from Google Trends for the keyword “Lyme” were analyzed, and we observed a high correlation between the LB incidence rate in primary care and Google Trends’ search volume data. Notably, the evolution of Google Trends data precedes the evolution in the incidence of LB by one year, suggesting that increasing interest in LB may have led to the increase in incidence rates observed from 2015. The Health Barometer Survey, a population survey on LB knowledge and awareness of LB in France, confirms this observation with an increase of Lyme disease awareness in the French population between 2016 and 2019 (Septfons et al., 2021). If this hypothesis is correct, the observed decrease in incidence rate in primary care since 2019 may not reflect a decrease in the actual number of LB cases but result from the decreasing interest in LB in the general population since 2018, leading to the reduction in the number of medically attended LB cases. Google Trends search volume for “Lyme” continued to decrease in 2021, which seems to correlate with the latest estimate from the Sentinel Network. We could also postulate that increasing interest in LB observed from 2014 to 2017 led to greater adherence to measures to prevent LB, resulting in a decline in the number of LB cases after a few years. The Health Barometer Survey indicates an increase in the use of protective measures against LB between 2016 and 2019 (Septfons et al., 2021).
The number of hospitalized cases started to decrease after a modest increase in 2017, and the speed of reduction was amplified in 2020 and 2021. Interestingly, the decreasing rate varied by age group, with older age groups more impacted in 2020 and then shifting to all adults in 2021. This observation should be taken into consideration. In 2019, the French guidelines on Lyme management evolved to recommend the use of oral doxycycline to treat Lyme neuroborreliosis instead of intravenous ceftriaxone, which may require hospitalization (Figoni et al., 2019). This recommendation was implemented in patients aged 8 years and older only. Also, the guidelines recommended the use of doxycycline as a first-line antibiotic, instead of amoxicillin, to treat erythema migrans in the adult population (Jaulhac et al., 2019), given the continuum between early localized and disseminated borreliosis and the efficacy of doxycycline for the treatment of neuroborreliosis (Stupica et al., 2018; Ljøstad et al., 2008). The application of this recommendation may have reduced the number of cases of disseminated LB, leading to reduced hospitalizations in the adult population.
Other explanations are the reduction in lumbar puncture performed since the COVID-19 pandemic, which may also require hospitalization, and the creation of Reference Centers for Tick Vector-Related Diseases (Centres de Référence des Maladies Vectorielles liées aux Tiques or CRMVT) in 2019. These centers are specialized in the treatment of disseminated forms of LB; as a result, they may request hospitalization less frequently compared with other health care professionals and also have better ICD-10 coding practices. In general, coding practices for LB could have improved in recent years, which may contribute to the decrease in hospitalizations coded as LB. However, additional data are needed to confirm these hypotheses.
It is difficult to explain the regional trends observed in LB incidence rates and underlying inconsistencies between the Sentinel Network and EMR data. This may arise from the limited number of active general practitioners in these primary care surveillance networks. LB hospitalization rates decreased in almost all regions but with important differences. While there is no clear pattern emerging from the data, the finding seems related neither to the initial incidence of hospitalization nor to the geographic location. This might be because of different rates of adoption of the new antibiotic guidelines into clinical practice.
There were limitations of the study. First, data from disseminated disease cases who were not hospitalized but treated by specialists (e.g., rheumatologists and neurologists) in the community or as outpatients in the hospital setting were not analyzed. The Sentinel Network reports disseminated disease seen by general practitioners but does not include specialists. The EMR data analyzed in this study were extracted from general practitioners only. As this network also includes a panel of diverse specialists, it may be worth investigating these data, despite the limited number of active specialists involved. Also, the Reference Centers for Tick-borne Diseases are treating an increasing number of patients with disseminated manifestations, and the analysis of their activities could provide a better understanding of LB epidemiology. Second, the relative accuracy of LB incidence estimations from the Sentinel Network and EMR data led to substantial annual variability across regions because of the limited number of active general practitioners by region within the surveillance system. This limitation was addressed by pooling data over a multiyear time period. Third, low specificity and reliability of ICD-10 codes for LB in PMSI data have been reported previously, and LB cases from the EMR have not been validated by a panel of experts.
Interpretation of LB epidemiology data is complex as current surveillance systems have inherent limitations. In primary care, the estimated LB incidence is highly dependent on the capacity of the population to recognize the early signs of LB and seek medical care. Hence, changes in LB rates reported in primary care settings may simply reflect changes in care-seeking behaviors for early disease. Further, reductions in LB hospitalizations may not reflect reductions in the number of disseminated cases but rather improved disease management leading to fewer hospitalizations. Unfortunately, there are limited data currently available from specialists who manage the vast majority of disseminated LB cases, and this analysis did not track the evolution of disseminated cases that are not hospitalized. Improved surveillance systems, broader LB surveillance, or new methodologies, such as mathematical modeling based on seroprevalence, could help to better estimate the incidence of LB.
Conclusions
The reported LB incidence decreased in 2020 and 2021 compared with previous years. The decrease observed in primary care is likely because of reduced population interest in LB, leading to lower medical care-seeking behavior. The decrease in LB hospitalizations may be explained by the implementation of new antibiotics guidelines in 2019, and the evolution of clinical practice, including patient management. Surveillance systems are critical to understand the evolution of LB epidemiology. However, they are affected by numerous external factors that need to be considered for an accurate and comprehensive picture of disease burden.
Footnotes
Acknowledgments
The authors extend their gratitude to Réseau Sentinelles and Agence technique de l’information sur l'hospitalization for collecting and providing the data used in this epidemiological analysis. The views and opinions of the authors expressed herein do not necessarily state or reflect those of these institutes and the health authorities. The authors thank Melissa Furtado of Pfizer for medical writing support and editorial assistance and Sonia Philipose of Pfizer for editorial assistance; medical writing support and editorial assistance were funded by Pfizer.
Authors’ Contributions
C.N., S.D., A.B., and J.H.S. conceptualized the study. J.H.S. acquired funding for the study. C.N., S.D., A.B., J-F.F., J.C.M., and J.H.S. developed the study methodology. C.N. and J.H.S. provided project administration. All authors contributed to the study investigation. C.N., S.D., and A.B. curated the study data. All authors contributed to the formal analysis of study data and validation. C.N. wrote the original draft of the article and developed data visualizations. All authors contributed to reviews and edits of subsequent drafts. All authors reviewed and approved the final version for submission.
Author Disclosure Statement
S.D. and A.B. are employees of IQVIA, which Pfizer contracted with to support data acquisition and analysis for this study. E.B. has no conflict of interest to declare. J-F.F. received honoraria for an advisory board from Pfizer. C.N., A.P., J.C.M., and J.H.S. are employees of Pfizer and may hold stock or stock options.
Data Availability Statement
Data from PMSI that support the findings of this study are available from the Technical Agency for Information on Hospital Care-ATIH (PMSI holder). While these data are not publicly available, an authorization was requested and received for the current study. Data from EMRs that support the findings of this study are available from IQVIA; however, restrictions apply, and the data were used under license for the current study and therefore not publicly available. Data from the Sentinel Network are publicly available on their website within the annual reports (![]() ).
).
Funding Information
This study was jointly funded by
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.