
Abstract
In the past few decades, reported human cases of Colorado tick fever in the western United States have decreased dramatically. The goal of this study was to conduct surveillance for Colorado tick fever virus (CTFV) in Dermacentor ticks in recreational sites in Colorado, Wyoming, and California to determine whether the virus is still present in Dermacentor ticks from these states. Surveillance focused on regions where surveys had been conducted in the 1950s, 1960s, and 1970s. Adult Rocky Mountain wood ticks (Dermacentor andersoni), Pacific Coast ticks (Dermacentor occidentalis), and winter ticks (Dermacentor albipictus) were tested by PCR. A subset of PCR-positive D. andersoni ticks (n = 7) were cultured in Vero cells. CTFV-positive Rocky Mountain wood ticks were found in all states: Colorado (58% prevalence), Wyoming (21%), and California (4%). Although no winter ticks tested positive, Pacific Coast ticks tested positive in one county (Siskiyou County, 15% prevalence) and were positive only in a location that also maintained Rocky Mountain wood ticks and golden mantled ground squirrels, a known CTFV host. In summary, CTFV is prevalent in D. andersoni and D. occidentalis in regions where they are sympatric in California and in D. andersoni in Colorado and Wyoming. Although the number of human CTFV cases has declined dramatically, this decrease in reported disease does not appear to be due to the disappearance or even the decline in prevalence of this virus in ticks in historically endemic regions of the country.
Introduction
Colorado tick fever virus (CTFV) is a tick-borne virus in the genus Coltivirus (family Reoviridiae), endemic to mountainous regions of western North America above 1000 meters elevation. With an incubation period of 0–14 days in humans, Colorado tick fever (CTF) presents clinically with a sudden onset of fever (up to 40°C), commonly in conjunction with headache, chills, myalgia, and/or photophobia (Klasco, 2002, Romero and Simonsen, 2008, Yendell et al., 2015). The characteristic biphasic fever of CTF is distinct from most other tick-borne diseases and involves sudden onset of fever, typically 3–6 days after tick bite, followed by a remission for 2 days, and recurrence of symptoms for 1–2 days.
Although CTF has been described as causing “intense illness” with 31% of cases requiring hospitalization, CTF is rarely fatal, although pediatric fatalities have been reported in northern California (Yendell et al., 2015; California Department of Public Health [CDPH] archived reports). Diagnosis is facilitated early in disease by an RT-PCR test that detects viral RNA. This test is available at some state public health laboratories and at the U.S. Centers for Disease Control and Prevention (CDC). Later in disease progression, IgG antibodies can be detected and a fourfold increase in titer supports a confirmed diagnosis (McDonald et al., 2019).
Treatment is supportive. Clinically, CTF may resemble tick-borne relapsing fever caused by Borrelia hermsii, a soft tick-transmitted disease that also occurs in high mountainous areas in the western United States. Tick-borne relapsing fever may be differentiated from CTF clinically by a longer period between febrile episodes (typically 5–7 days), multiple bouts of febrile episodes, and diagnostically, by the presence of Borrelia spirochetes on a Giemsa-stained blood smear; other serological tests can differentiate these two diseases (Forrester et al., 2015).
The primary tick vector of CTFV is Dermacentor andersoni, the Rocky Mountain wood tick; the adult stage of this tick is most commonly active in the spring and summer months (Williamson et al., 2019). Immature ticks acquire the virus from rodent hosts, such as golden-mantled ground squirrels (Callospermophilus lateralis) and chipmunks (Tamias spp.) (Clark et al., 1970; Sonenshine et al., 1976; Carey et al., 1980). The virus is not transovarially (vertically) transmitted to larvae from infected female ticks (Eklund et al., 1961), but can be passed transstadially from larvae to nymph to adult. The virus is found in the salivary glands of D. andersoni and can be transmitted soon after attachment (Goodpasture et al., 1978).
As early as the 1850s, CTF was recognized as a tick-borne disease in the Rocky Mountain region, distinct from Rocky Mountain spotted fever (Becker, 1930). The virus was not identified until 1946 when it was isolated and demonstrated to be pathogenic through transmission experiments, including experimental transmission of the virus through sera transferred from sick people to volunteers (Florio et al., 1944, Florio and Stewart, 1947). Between 1948 and 1959, a total of 552 cases were reported from 10 western states, and more recently, between 1985 and 1995, 864 cases were reported in 8 western states.
The 10-year incidence from 1985 to 1995 in cases per million population for the western states was WY 12.8, CO 9.9, UT 6.4, MT 1.3, NV 0.9, and CA 0.3, plus rare cases in ID and WA. A recent assessment of CTF in the United States between 2002 and 2012 documented a decrease of >90% of reported cases, with only 75 cases reported during this period (Yendell et al., 2015); only 59 cases were reported to CDC during 2010–2019 (Centers for Disease Control and Prevention, 2021). Wyoming currently has the highest annual incidence of CTF among residents followed by Montana and Utah.
California has had no locally acquired reported cases since 1995. Despite changes in diagnostic approaches (Basile, 2011), it is unclear whether the decrease in CTF case reports is due to lack of recognition of this disease by health care professionals, lack of laboratory testing, lack of reporting to state health departments, less tick exposure, or a decrease in prevalence of infection in ticks over time. Although CTF has remained a reportable disease in Wyoming, CTF was removed from state reportable disease regulations in Colorado in 1997 and in California in 2010.
In this study, adult Dermacentor spp. ticks were collected and tested for CTFV from areas in Colorado, Wyoming, and California where ticks tested positive between 1953 and 1971, the peak of CTFV reporting in the United States. Infection prevalence in ticks collected during 1953–1971 was compared with more recent collections. The goal of this investigation was to ascertain whether CTFV prevalence in ticks has decreased in the 21st century, following a similar trend to human CTF case numbers.
Materials and Methods
Historic tick collections and testing
Archived tick surveillance and test records were reviewed to determine prevalence of CTFV in ticks collected between 1953 and 1971 (including: Kohls, 1955). Before the advent of modern molecular testing for viruses, ticks were tested either individually or in pools by triturating within phosphate-buffered saline augmented with antibiotics and rabbit serum, and subsequent injection of tick samples intraperitoneally into 1- to 4-day-old suckling mice. The presence of virus was confirmed in mouse brain by neutralization tests or immunofluorescence staining (Eklund et al., 1958, Emmons, 1988).
Contemporary tick collections and testing
Adult Dermacentor spp. ticks were collected in 2010 and 2011 at sites with historic records of D. andersoni in California, Colorado, and Wyoming, typically in areas between 1000 and 2700 meters elevation (Fig. 1). In California, Dermacentor occidentalis were collected in eight counties including two counties at lower elevations outside the range of D. andersoni but where there was indication that CTFV, or a related virus, may be present in Pacific Coast ticks (Lane et al., 1982).
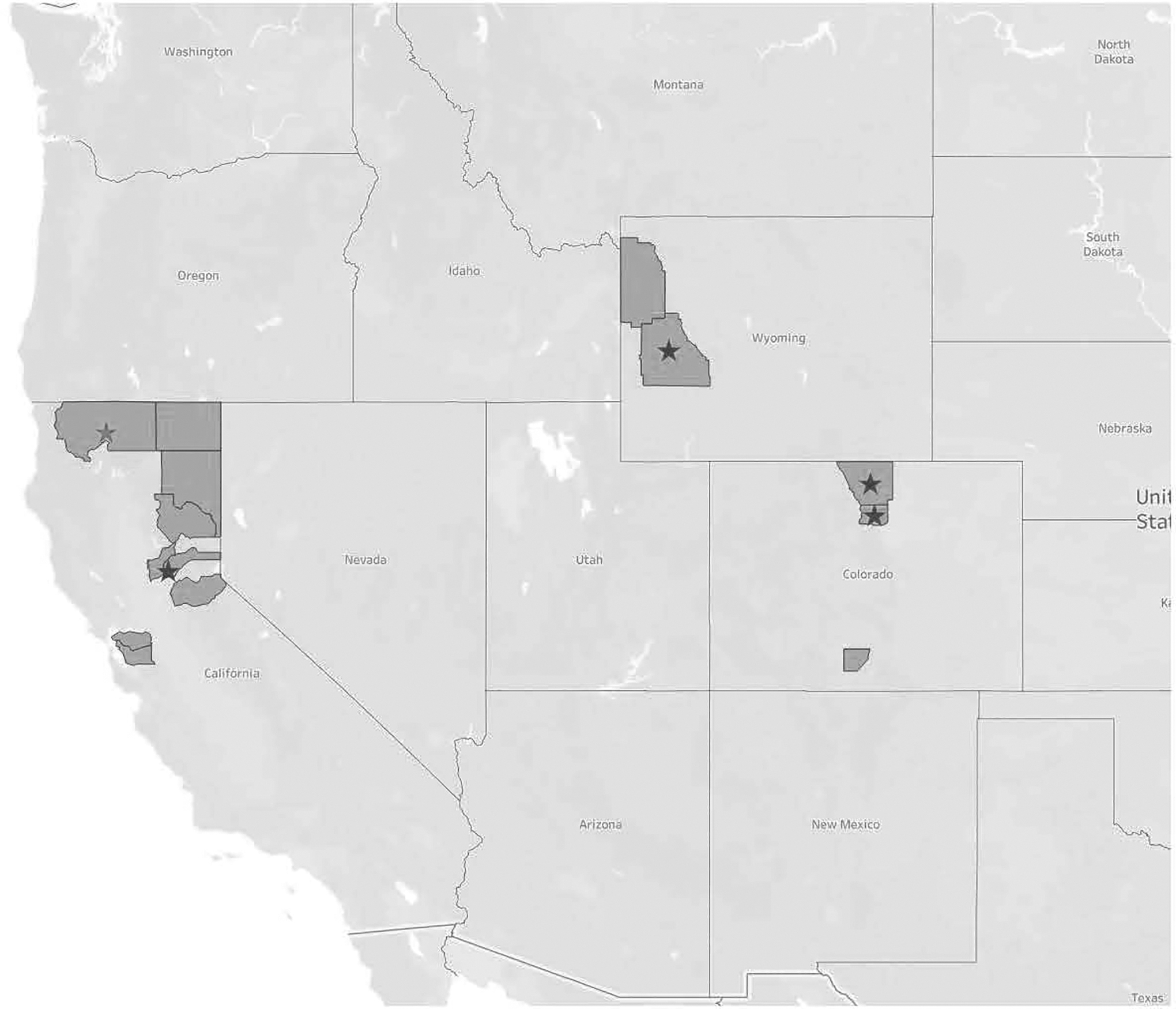
Counties where ticks were collected in 2010–2011 are shaded. Locations with colorado tick fever virus-positive ticks are indicated by stars.
Ticks were collected from vegetation using 1 meter2 white flannel flags and retained before testing in 37-mL polystyrene containers (Fisher Scientific) in sealed plastic bags with moistened paper toweling at 3°C or in 70% ethanol within 1.5-mL microcentrifuge snap-cap tubes. All ticks were identified to species, life stage, and gender using taxonomic keys (Furman and Loomis, 1984).
Tick testing
All ticks collected in 2010 and 2011 were tested at CDC, Division of Vector-borne Diseases, Arbovirus Disease Branch, Fort Collins, Colorado. RNA was extracted from individual ticks using the QIAamp Viral RNA mini kit, following the manufacturer's instructions (QIAGEN, Valencia, CA). Extracted RNA was tested with primers and probes designed from the CTF virus strain Florio VP2 from GenBank AF139758, targeting the second genomic segment of the 12 segments of double-stranded RNA as detailed in Lambert et al., 2007 (Basile, 2011). The criterion for considering a tick positive with this real-time RT PCR TaqMan assay was a cycle threshold value ≤38. A subset of D. andersoni ticks from Colorado also were tested by Vero cell culture.
Results
Historic tick testing results
In California tick collections made in 1953, 1968, and 1971 in Lassen, Modoc, Plumas, and Siskiyou counties, the minimum CTFV infection prevalence in D. andersoni was 4.4% (21 pools positive of 481 ticks tested); in D. occidentalis, the minimum CTFV infection prevalence was 36.2% (92 pools positive of 254 ticks tested) (Table 1). In addition, the Viral and Rickettsial Disease Laboratory (VRDL), California Department of Public Health, cultured two virus isolates from two pools of two and three adult D. andersoni collected from Sagehen Creek, Nevada County, collected in July 1958. VRDL also cultured one virus isolate from a pool of 17 adult D. andersoni collected in May 1958 and a pool of a single female D. andersoni collected in July 1958 from the site of a Civilian Conservation Corps camp near Hackamore, Modoc County (CDPH, archives).
Historic Tick Testing Results, California, 1953–1971, Lassen, Modoc, Plumas, Siskiyou Counties
Data acquired from California Department of Public Health Archived Records.
Per Kohls (1955).
Dermacentor andersoni and Dermacentor occidentalis from Mt. Hebron and Tennant sites, May 1968, were tested as one pool.
Tick testing results
Contemporary testing by RT-PCR of ticks collected in 2010 and 2011 in California, Colorado, and Wyoming yielded CTFV-positive D. andersoni and D. occidentalis in all three states (Table 2; Fig. 1). Larimer and Boulder Counties in Colorado yielded infection prevalence of 61% and 59%, respectively. Although two Dermacentor albipictus from Jackson County, Wyoming, tested negative, 21% of D. andersoni collected from Sublette County, Wyoming, were positive for CTFV. In California, 15% of adult D. occidentalis from a single collection event in Siskiyou County were positive for CTFV; no other Pacific Coast ticks tested positive. Positive D. andersoni ticks were collected from Sagehen Creek, Nevada Countyl, in both 2010 and 2011; 2/31 (6.3%) ticks positive in 2010 and 2/67 (3.0%) ticks positive in 2011.
Adult Ticks Tested for Colorado Tick Fever Virus, Colorado, Wyoming, California, 2010–2011
Discussion
Although CTF is currently a rarely reported disease, the prevalence of CTFV-infected ticks sampled in 2010–2011 remained as high as it was in the mid-20th century, when CTF was regularly reported in some regions of the western United States. Between 1956 and 1965, 1767 human cases of CTF were reported, primarily from Boulder and Larimer Counties in Colorado and from Sublette County, Wyoming (McLean et al., 1981). From 1954 to 1979, an average of 8.8 human cases were reported per year in California, despite CTF not being a reportable disease in California at that time (Lane and Murray, 1980).
Based on archived records, tick surveillance conducted in California from 1955 to 1973 indicated high prevalence of CTFV-infected ticks in far-northern and northeastern regions of the state. Surveillance in Larimer County (Poudre Canyon), Colorado, in the 1970s indicated minimum infection prevalence between 11% and 38% (Eads and Smith, 1983). Similar to recent findings from Montana (Williamson et al., 2019), the prevalence of infection in two of the historic sites revisited in California and Colorado indicates a similar risk of exposure to CTFV-infected ticks in the 21st century.
In California, CTFV was the suspected agent in an outbreak of a biphasic fever with onset in May and June 1933, in ∼25 people from a Civilian Conservation Corps camp based at Hackamore near Alturas, Modoc County (Kohls, 1955). In 1953, the virus was isolated from D. andersoni and D. occidentalis near this location as well as from a patient in Alturas in 1954 (CDPH archives). In May 2010, two CDPH biologists revisited and surveyed multiple sites around Alturas for 2 days to collect D. andersoni; only one adult D. occidentalis was found. This may reflect changing habitat or ecology of the ticks in the area.
At one site, University of California Berkeley Sagehen Creek Field Station in the Truckee/Tahoe Basin area, Nevada County, CTFV was detected as early as July 1958 from a pool of one female and two male adult D. andersoni ticks (VRDL strain Ar 504, CDPH archives). Tick surveillance has been conducted at least every other year at this site, starting in 2010, to determine persistence, abundance, and prevalence of CTFV (only 2010 and 2011 results shown here due to testing constraints).
Of note, one of the authors has sampled this site periodically since 1994, and in the past 30 years, the site has become much more commonly used by hikers, dog walkers, and fishermen (K.A.P., personal observation). In addition, the risk of human exposure to CTFV may potentially be greater than in years prior as the human population in this region has grown considerably in the past 70 years (e.g., Truckee 1950 population 1025; 2020 population 17,131) (Nevada County, 2021).
In Colorado, ticks were collected at three different sites for this study: Great Sand Dunes National Park (Alamosa County), Poudre Canyon, Roosevelt National Forest (Larimer Country), and Boulder Mountain Park (Boulder County); Table 2. All sites are popular for outdoor recreation. Of note, Boulder Mountain Park is on the outskirts of Boulder, Colorado, a city that, similar to the Tahoe Basin region of California, has experienced a large population growth in the past 70 years (1950 population 19,916 [U.S. Census Bureau, 1950]; 2019 population 105,673: U.S. Census Bureau QuickFacts: Boulder city, Colorado). In Wyoming, ticks were collected in Grand Teton National Park (Jackson County) and Bridger-Teton National Forest (Sublette County); both sites are also popular for outdoor recreation.
The high CTFV prevalence in D. andersoni collected from Sublette County, Wyoming (21%, Table 2), Bridger-Teton National Forest, Wyoming (21%; Geissler et al., 2014), Larimer (61%) and Boulder (59%) counties, Colorado (Table 2), the Bitterroot Valley, Montana (6.6%; Williamson et al., 2019), and 4% along a popular recreation trail in Nevada County, outside of Truckee, California (Table 2) documents the continued and widespread presence of CTFV in the western United States and supports increasing public health outreach regarding tick-bite prevention measures such as posting informational signage at heavily used trails or other outdoor recreational sites.
In addition, educational outreach and online resources that target health care providers in counties that harbor D. andersoni are warranted and should include information on both historical and contemporary CTFV cases. Health care providers are recommended to inquire about tick-bite history when patients present with a febrile illness in spring or summer months. Besides outreach and education, additional D. occidentalis surveillance and testing in areas where this tick is sympatric with D. andersoni would clarify whether the CTFV prevalence is similar between the two tick species; in some California sites, both historic and contemporary, D. occidentalis had higher CTFV prevalence than D. andersoni and may locally present a higher disease transmission risk to people.
Although D. andersoni is the primary vector of CTFV, D. occidentalis has been shown to have similar CTFV prevalence in areas where the two ticks overlap in California. Dermacentor occidentalis can be an abundant tick in many parts of California and readily bites humans. The distribution of D. occidentalis is restricted to the Pacific coastal states (Washington, Oregon, and California) and northern Baja Mexico, and is not found in the Rocky Mountain states such as Colorado and Wyoming (Furman and Loomis, 1984; Elizabeth Dykstra, Washington State Department of Health, personal communication).
Previous studies have detected CTFV in other tick species, but many of the positive ticks were removed from vertebrate hosts, such as D. albipictus, D. parumapertus, Otobius lagophilus, Haemaphysalis leporispalustris, Ixodes spinipalpis, and Ixodes sculptus (Kohls, 1955, Emmons, 1988); these CTFV-positive ticks, all wildlife focused and not human biting, were collected only in the geographic range of D. andersoni. In this study, only two D. albipictus were collected from Sublette County, Wyoming, and both tested negative. The potential for other tick species to maintain CTFV in nature and potentially transmit to humans should be investigated.
The distribution of CTF disease in people overlaps the geographic distribution of D. andersoni as well as one of the primary vertebrate hosts, the golden-mantled ground squirrel. This tick is also found on a variety of other vertebrates including yellow-pine chipmunks (Tamias amoenus), least chipmunks (Tamias minimus), mice (Peromyscus spp.), porcupines (Erethizon dorsatum), and other mammals (Burgdorfer and Eklund, 1959, Emmons, 1966, 1988, McLean et al., 1981, Furman and Loomis, 1984).
By providing current information about CTFV in western tick populations, we hope to increase physician awareness of CTF in areas of risk. Based on these results, as well as recent results from tick surveillance in Montana (Williamson et al., 2019), tick and human surveillance in Wyoming (Geissler et al., 2014), and human case follow-up and serological surveillance in Oregon (McDonald et al., 2019), CTF may still be a tick-borne disease of public health importance (Brackney et al., 2010). CTFV-infected ticks are abundant in many regions in the west, including popular recreational areas, and thus it is reasonable for a health care provider who has a patient presenting with a biphasic fever to consider CTF as a differential diagnosis, particularly if the patient lives or recreates in mountainous areas or reports tick bite exposure.
As a case in point, just months after hearing a presentation on CTFV and California data at a meeting of epidemiologists and physicians in 2012, one physician identified a CTF case in a California resident with exposure in Colorado; this case would not have been diagnosed and reported correctly without this outreach. Increasing awareness for health care providers of CTF risk in endemic areas may improve detection of this disease and elucidate current public health risk.
Footnotes
Acknowledgments
We thank the biologists who contributed to this study by collecting ticks, including Larry Bronson, Joshua Ogawa, Charlie Smith, and Stefan Sielsch. We would also recognize Dr. Carol Glaser for astutely diagnosing CTFV in a California resident (acquired in Colorado), the first reported case of CTFV in California for 17 years, after hearing a summary of these tick surveillance results. We also gratefully acknowledge the support of Robert Lanciotti (CDC) for tick testing and Vicki Kramer (CDPH) for reviewing this article.
Disclaimer
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the CDC, the California Department of Public or the California Health and Human Services Agency. Use of trade names is for identification only and does not imply endorsement by the Public Health Service or by the U.S. Department of Health and Human Services.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.