
Abstract
Schistosoma mekongi infection is endemic in countries along the Mekong River and certain of its tributaries in the lower Mekong basin, especially in Lao People's Democratic Republic and Cambodia. Diagnosis of schistosomiasis is crucial before treatment and epidemiological surveys before and/or after an intervention, such as a mass drug administration. A newly developed immunochromatographic test (ICT) for the diagnosis of schistosomiasis mekongi, based on antiparasite antibody detection in human sera, was evaluated. The schistosomiasis mekongi
Introduction
Schistosoma mekongi causes schistosomiasis mekongi in humans and is endemic in the southern parts of the Lao People's Democratic Republic (Lao PDR) and in northeastern Cambodia along the Mekong River (Muth et al. 2010, Gordon et al. 2019, Sayasone et al. 2020). The parasite is also zoonotic, infecting dogs and pigs (Ohmae et al. 2004, Muth et al. 2010). More than 140,000 people are estimated to be at risk of infection in these two countries, where morbidity levels are high (Urbani et al. 2002, Chai and Jung 2019, Sayasone et al. 2020). Although geographically restricted in parts of Lao PDR and Cambodia, S. mekongi affects not only people living in endemic areas but also immigrants and travelers to the endemic areas (Leshem et al. 2009).
Humans are infected by the percutaneous penetration of the infective cercariae that are released from the intermediate host snail (Neotricula aperta) into freshwater (Attwood and Upatham 2012, Limpanont et al. 2015).
The mature worms are paired, and the females lay eggs in the superior mesenteric veins of the host. The eggs are carried by blood flow from the mesenteric veins into the liver, where they are trapped and can cause local granuloma formation, and pathology can progress to hepatosplenomegaly, enlarged periportal vein, and portal hypertension (Biays et al. 1999, Ohmae et al. 2004, Sinuon et al. 2007, Colley et al. 2014, Sayasone et al. 2020). The pathology of S. mekongi infection is similar to that of Schistosoma japonicum, and infection with either species can have serious outcomes if left untreated (Zhou et al. 2010, McManus et al. 2018). These two Schistosoma species are very closely related (Attwood et al. 2015).
The regional action plan for neglected tropical diseases in the Western Pacific Region for years 2012–2016 recommended targeting schistosomiasis mekongi for elimination (WHO Regional Office for the Western Pacific 2013). The first step in attacking any parasitic diseases is to establish methods for accurate diagnosis. This is crucial before treatment and also for epidemiological surveys of schistosomiasis in endemic areas to determine the prevalence of infection before and/or after an intervention, such as mass drug administration (Ross et al. 2001, McManus et al. 2018).
Various techniques have been established to diagnose schistosomiasis mekongi in humans and animals. These include parasitological (Sayasone et al. 2015), immunological (Ittiprasert et al. 2000, Ohmae et al. 2004, Zhu et al. 2005, Nickel et al. 2015, Sangfuang et al. 2016, Vonghachack et al. 2017), and molecular methods (Sanpool et al. 2012, Kongklieng et al. 2013, Thanchomnang et al. 2013). The parasitological approach to detect Schistosoma eggs in human stool samples, particularly the Kato–Katz thick smear technique, is time consuming and might overlook light infections.
However, this method has been utilized for control programs in Lao PDR and Cambodia (Vonghachack et al. 2017, Sayasone et al. 2020). Therefore, highly sensitive, user
However, false-positive results were seen among patients with opisthorchiasis and urinary tract infections and hematuria (Homsana et al. 2020). Until now, there has been no report of a lateral flow device “ICT” for detecting anti
Materials and Methods
Ethical approval
All procedures performed in studies involving human participants were in accordance with ethical standards of the Khon Kaen University Ethics Committee for Human Research (HE621265) and with the 2013 Declaration of Helsinki and its later amendments or comparable ethical standards. Experimental mice and N. aperta snails were handled according to the Guidelines for Animal Experimentation of the National Research Council of Thailand and approved by Faculty of Tropical Medicine Animal Care and Use Committee at Mahidol University in Bangkok, Thailand (FTM
Preparation of S. mekongi antigen
Frozen S. mekongi adult worms were obtained from the Applied Malacology Center, Department of Social and Environmental Medicine, Faculty of Tropical Medicine, Mahidol University, Thailand. The preparation of the antigen was performed as follows: briefly, the worms (∼200 mg wet weight) were homogenized with a tissue grinder in a small volume of distilled water (500 μL) containing proteinase inhibitors (Mini EASYpack Protease Inhibitor Cocktail Tablets; Roche, Basel, Switzerland), and the homogenate was centrifuged at 10,000 × g at 4°C. The protein concentration of the resultant supernatant was determined using a standard method (Lowry et al. 1951).
Human sera
In total, 209 serum samples were supplied from the Frozen Serum Bank at the Faculty of Medicine, Khon Kaen University and Department of Parasitology, National Institute of Infectious Diseases, Tokyo, Japan. Fourteen serum samples were collected from schistosomiasis mekongi patients located in the Champasak Province, southwestern Lao PDR (their demographic data are presented in Table 1 and Supplementary Table S1), and 30 samples were from schistosomiasis japonica patients located in Leyte Island, the Philippines (Table 1 and Supplementary Table S2).
Types of Human Sera Examined and Results of Screening these Using the Smk-Immunochromatographic Test Kit
Band intensity at the T-line was evaluated according to the reference color card.
Smk-ICT, schistosomiasis mekongi-immunochromatographic test.
Schistosomiasis mekongi patients were schistosome egg positive in stool samples according to the Kato–Katz thick smear method (Katz et al. 1972), whereas schistosomiasis japonica patients were schistosome egg positive in stool samples according to the direct smear technique using a total of 1 g of feces (Beaver et al. 1984). The remaining 135 serum samples were from patients with other parasitic diseases (Table 1), with infection status confirmed by parasitological and/or serological methods.
Cases of opisthorchiasis, paragonimiasis, taeniasis saginata, ascariasis, hookworm infections, trichuriasis, capillariasis philippinensis, and strongyloidiasis were confirmed by detection of parasite eggs or larvae in stool samples using the modified formalin ethyl acetate concentration method (Elkins et al. 1986). Cases of clonorchiasis were confirmed by the modified Kato–Katz technique (Katz et al. 1972). Cysticercosis was diagnosed using computed tomography scanning and immunodiagnostic tests (Intapan et al. 2008). Gnathostomiasis cases were confirmed using information from a combination of serological methods, clinical manifestations, and a history of risky dietary preferences (Intapan et al. 2010).
Angiostrongyliasis cases were confirmed by serology and clinical manifestations (Somboonpatarakun et al. 2020). Trichinellosis cases were confirmed by detection of larvae in muscles and serology (Morakote et al. 1991). Sparganosis was diagnosed by histopathological investigation (Boonyasiri et al. 2014). Thirty samples were included from healthy volunteers who resided outside endemic areas for S. mekongi and who proved to be negative for intestinal parasitic infections based on the formalin ethyl acetate concentration technique (Elkins et al. 1986) at the time of blood collection.
Preparation of the lateral flow immunochromatography strip
The Smk
Colloidal gold (40 nm) conjugated with mouse anti
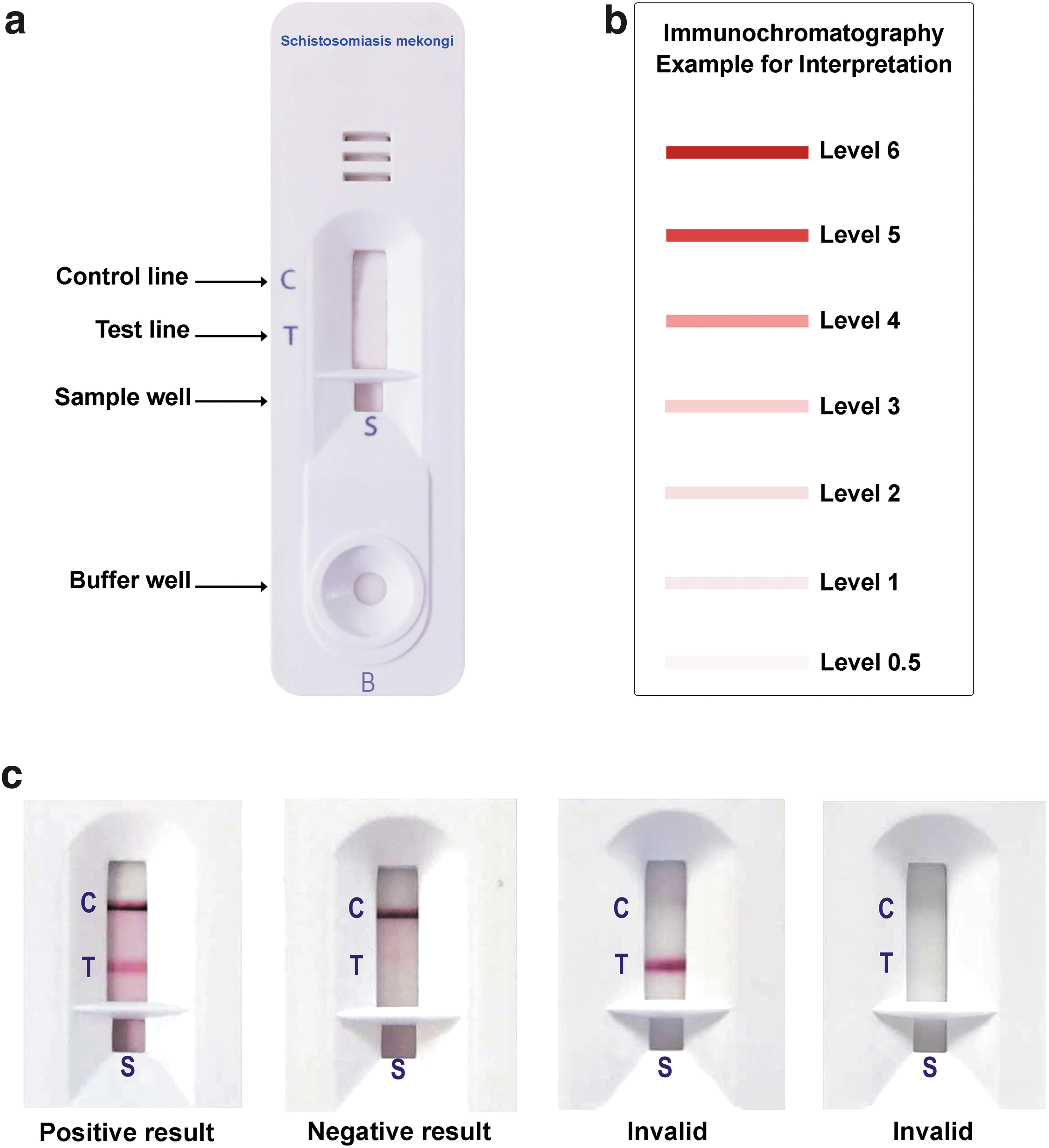
The lateral flow immunochromatographic test for schistosomiasis mekongi.
Testing of the Smk-ICT
The optimized Smk
Results
After optimization, Smk
Diagnostic Values of the Smk
Numbers in parenthesis indicate ranges of 95
Diagnostic value calculation for schistosomiasis mekongi only
Diagnostic value calculation for schistosomiasis japonica only
Diagnostic value calculation when combining schistosomiasis mekongi and schistosomiasis japonica as a composite disease entity
The diagnostic sensitivity and specificity values for schistosomiasis mekongi were calculated as 78.6% (95% confidence interval [CI] 49.2–95.3) and 97.6% (95% CI 93.9–99.3), respectively. Most of the serum samples from schistosomiasis japonica cases were positive (73.3%, 22/30), and relevant diagnostic values are shown in Table 2. Combining S. mekongi and S. japonicum infections as a composite disease entity yielded values for diagnostic sensitivity and specificity of 75.0% (95% CI 59.7–86.8) and 97.6% (95% CI 93.9–99.3), respectively. Cross
Discussion
Human schistosomiasis is a tropical helminthic disease, which remains prevalent in several nations (McManus et al. 2018). In Asia, S. japonicum, S. mekongi, and very rarely Schistosoma malayensis are zoonotic species causing schistosomiasis (Gordon et al. 2019). The present study focused on the development of a diagnostic system for the detection of schistosomiasis mekongi patients in the Mekong River basin, especially in Lao PDR and Cambodia.
Previously, serological assays were developed for diagnosis of S. mekongi infection (Ittiprasert et al. 2000, Ohmae et al. 2004, Zhu et al. 2005, Nickel et al. 2015, Sangfuang et al. 2016, Vonghachack et al. 2017). Ittiprasert et al. (2000) reported 100%, 35.2%, and 50%, respectively, of sensitivity, specificity, and accuracy for antibody detection by enzyme-linked immunosorbent assay (ELISA) using a crude adult S. mekongi antigen. Furthermore, an ELISA to detect antibodies against soluble S. japonicum egg antigens, used in a survey of communities along the Mekong River in Cambodia, gave positive results varying from 40% to 90% (Ohmae et al. 2004).
A dipstick dye immunoassay kit, using S. japonicum soluble egg antigen for the diagnosis of schistosomiasis mekongi, had sensitivity of 97.1%, but cross-reaction occurred in 18.3% of patients infected with Opisthorchis viverrini (Zhu et al. 2005). We observed no cross-reaction with opisthorchiasis samples. This could be due to the use of a different antigen type from that used by Zhu et al. (2005) and the fact that we collected opisthorchiasis sera from areas nonendemic for schistosomiasis mekongi. However, cautious interpretation should be made in areas where both S. mekongi and O. viverrini co-exist. The calculated sensitivity of a S. mansoni
Recently, a survey in villages in Lao PDR and Cambodia, using ELISA to detect antibody against S. mansoni antigens, gave positive results for 43.1% and 26.5% of those tested, respectively (Vonghachack et al. 2017). In the present study, the diagnostic values of our kit were calculated as 78.6%, 97.6%, and 96.1% for sensitivity, specificity, and accuracy, respectively. This kit can also detect schistosomiasis japonica cases, a result expected given their shared antigenic epitopes (Zhu et al. 2005). Combining results from schistosomiasis mekongi and schistosomiasis japonica samples, the sensitivity was 75.0% and the accuracy was 92.8%.
Despite their being S. mekongi egg positive, our Smk-ICT gave negative results in three individuals. One possible reason is that these serum samples were collected from cases soon after S. mekongi infection, resulting in low antibody responses. Serial blood collections following infection are required to determine when seroconversion occurs. In S. mansoni and S. haematobium infections, seroconversion took at least 6 months, while eggs were detected much earlier (Bottieau et al. 2006). Another possibility is variation in host genetic factors affecting immune responses, that is, relating to major histocompatibility complex class II phenotypes in infected populations as revealed in another schistosomiasis endemic area (Waine et al. 1998).
Cross-reactions were observed in paragonimiasis heterotremus, sparganosis, trichinellosis, and taeniasis saginata serum samples collected from areas not endemic for schistosomiasis mekongi. Previous workers on diagnosis of human schistosomiasis have made similar observations (Ittiprasert et al. 2000, Yu et al. 2011, Jiang et al. 2014). Despite the relatively low cross-reaction rate we found (2.4%), which is much lower than that in those studies, this is still a concern with the POC tool. A questionnaire about risk behaviors for parasite infections can support the interpretation of results in a population-level study. Moreover, clinical symptoms of other parasitic infections usually differ from those of schistosomiasis at the symptomatic stage (Biays et al. 1999, Gottstein et al. 2009, Blair 2014, Liu et al. 2015, Sanpool et al. 2017).
In addition to the limitations detailed above, there are investigations and enhancements that could be pursued in the future. The Smk-ICT has been developed as a POC tool for the rapid diagnosis of human schistosomiasis mekongi (and schistosomiasis japonica). The test is only semi-quantitative: intensity of color at the T-line can be read directly by the naked eye. However, quantification of color intensity should be performed using a machine such as a chromogenic test reader (Mewamba et al. 2021), and possible correlation of T-line intensity with Schistosoma egg counts in fecal samples should be investigated.
Prospective users of these kits should also be aware that only a small number (n = 14) of human schistosomiasis mekongi sera were used for sensitivity evaluation: additional schistosomiasis mekongi sera are required to confirm the reliability of the assays. The performance of the Smk-ICT kits may be affected by batch-to-batch variation of S. mekongi somatic antigens (Viana et al. 2019, Graeff-Teixeira et al. 2021). Sensitive and specific recombinant antigens that can be mass produced in the future will likely replace native antigens, such as we used here, and will lead to uniform performance.
Our Smk-ICT could be used for screening travelers who visit endemic areas
Conclusions
This rapid testing tool can be used to determine the seroprevalence of S. mekongi infection in endemic areas in countries along the Mekong River and certain of its tributaries in the lower Mekong basin. Thus, data can be provided on the real boundaries of schistosomiasis mekongi in these areas and act as ground truthing for geographical information systems. Although our Smk-ICT showed no cross-reactions with opisthorchiasis and clonorchiasis in the present study, further evaluation is necessary to verify this.
Footnotes
Acknowledgments
We would like to thank David Blair for valuable suggestions and assistance with the presentation of this article via Publication Clinic Khon Kaen University, Thailand.
Authors' Contributions
All authors contributed to the study conception and design. R.R., L.S., S.L., Y.L., P.C., H.O., Z.L., and H.Y. performed the material preparation and the sample collection. R.R., L.S., O.S., P.B., T.T., P.J., H.O., H.Y., P.M.I., and W.M. performed the data collection, methodology, investigation, and analysis. R.R., Z.L., H.Y., P.M.I., and W.M. contributed to the first draft of the article. All authors contributed to the editing, and reviewed and approved the final article.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This study was supported by a Distinguished Research Professor Grant from the Thailand Research Fund (O.S., P.M.I., and W.M.; grant number DPG6280002), a grant from Khon Kaen University Research and Graduate studies (O.S., P.M.I., and W.M.; Research Program Grant), a Scholarship under the Post-Doctoral Training Program from Khon Kaen University (R.R., grant number PD2564
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.