
Abstract
Objectives:
To study the epidemiological characteristics of malaria and the effects of comprehensive malaria control implementation in Yantai, as well as to provide a scientific basis for future malaria elimination.
Materials and Methods:
A retrospective analysis was conducted to explore the epidemiological changes and prevention effects in Yantai from 1951 to 2017. The malaria data before 2004 were collected from paper-based annual reports, and data after 2004 came from the Infectious Diseases Information Reporting Management System.
Results:
A total of 81,286 malaria cases were identified in Yantai from 1957 to 2017, with two peaks occurring in 1966 (120.93/100,000) and 1970–1972 (366.12/100,000). From 1951 to 2003, the case classification was mainly Plasmodium vivax (99.80%); the first case attributed to Plasmodium falciparum occurred in 2004, and P. falciparum became the main cause of malaria after 2011. All cases reported since 2010 have been imported cases, and the last indigenous case was caused by P. vivax in 2008. A total of 129 imported cases were reported from 2010 to 2017, most of which originated in Africa (93.80%), mainly in men aged 30–49 years (68.28%). From 1951 to 1973, 73,868 cases of malaria were diagnosed with clinical symptoms, and from 1974 to 2017, 818,943 cases in fever patients were diagnosed with blood tests.
Conclusions:
To achieve the goal of eliminating malaria by 2020, Yantai should continue to strengthen the management of migrant population, including improving malaria surveillance for returnees and immigrants from overseas endemic areas, and continue to increase the training of medical personnel to improve their diagnostic ability.
Introduction
Malaria is a debilitating vector-borne, protozoan tropical disease that is widely distributed in many countries (Zhang et al. 2016, Dhewantara et al. 2019, Kweyamba et al. 2019). Under certain environmental conditions, malaria epidemics are due to the Anopheles mosquito-borne transmission of Plasmodium vivax, Plasmodium falciparum, Plasmodium ovale, and Plasmodium malariae (Mace et al. 2018). The World Health Organization (WHO) estimates that between 2010 and 2017, malaria incidence decreased significantly by 18% and malaria mortality decreased by 28% (WHO 2017).
Despite significant progress, updated estimates have indicated that there were still 219 million malaria cases globally in 2017, 435,000 of which had fatal outcomes. Most malaria cases occur in the Africa continent (92%) (WHO 2018), especially in the sub-Saharan region, followed by the WHO's South-East Asia region (5%) and the Eastern Mediterranean region (2%) (Ramsay et al. 2016, Patouillard et al. 2017). In 2015, the WHO set ambitious new targets to reduce the global malaria burden by 90% by 2030 and encouraged member states to achieve the goal of malaria elimination (WHO 2017). However, due to the threat of malaria introduction and reintroduction, many countries face challenges in achieving the goal of elimination, especially in border areas adjacent to high malaria-endemic countries.
P. falciparum is the major cause of malaria in Africa, while P. vivax is the most widely distributed species outside Africa (Gething et al. 2012). In China, P. vivax has been prevalent for many years and has a high incidence historically (Zhang et al. 2014, Feng et al. 2015). Before 1949, there were ∼30 million cases of malaria in the country each year, reaching a peak in 1970 (2961/100,000). From 2004 to 2017, China reported that P. vivax accounted for 70.1% of all malaria cases and peaked in 2006. Through the increase in several fund-driven campaigns over recent decades, China has achieved remarkable success in controlling local malaria transmission (Feng et al. 2018). Since 2008, the number of P. vivax cases has declined; however, the proportion of P. falciparum has risen sharply. For example, the number of P. falciparum cases reported in 2009 was only 1033, accounting for 7.1% of all reported cases, while the number of reported P. falciparum cases in 2016 was 2066, accounting for 65.7% of all reported cases.
In the early 1960s and 1970s, two large-scale malaria epidemics occurred in Shandong Province, with 6 million and 4 million people, respectively, infected annually (Zhang et al. 2014). After the implementation of the malaria control strategy, the epidemic was effectively controlled, and the incidence of malaria dropped to very low levels, remaining below 1/100,000 annually (Xu et al. 2016).
Yantai, Shandong Province, used to be a high P. vivax-malaria-endemic area with Anopheles sinensis as the single vector (Dai et al. 2015). After decades of implementing comprehensive prevention and control measures, indigenous cases have been eliminated. However, since the 21st century, imported malaria from overseas from Africa and Southeast Asia has become an increasingly serious public health problem in Yantai, and the epidemiological characteristics and potential hazards of these malaria cases are relatively unknown. This study summarizes the epidemiological characteristics of malaria in Yantai from 1951 to 2017, as well as the effective measures taken for the prevention and control of malaria in different contexts. This study aims to provide scientific insights for the further development of targeted malaria control strategies and accelerate the realization of Shandong Province.
Materials and Methods
Study setting
Yantai is located in the northeast of Shandong Peninsula at 119°34′–121°57′ east longitude, 36°16′–38°23′ north latitude, adjacent to Weihai in the east, Weifang in the west, Qingdao in the Southwest, and the Yellow Sea and Bohai Sea in the north; Liaodong Peninsula and Dalian are just across the Bohai sea. Yantai had five districts, seven cities, and one county and has a warm, temperate continental monsoon climate. According to the local meteorological department website, the annual average temperature and precipitation are 13.0°C and 722.2 mm, respectively. The river network in Yantai is relatively developed, with 121 rivers over 5 km. Among the rivers, six rivers, including the Wulong River, Dagu River, and Xinan River, have an area of more than 300 square km; in addition, there are many small and medium-sized rivers (Fig. 1).
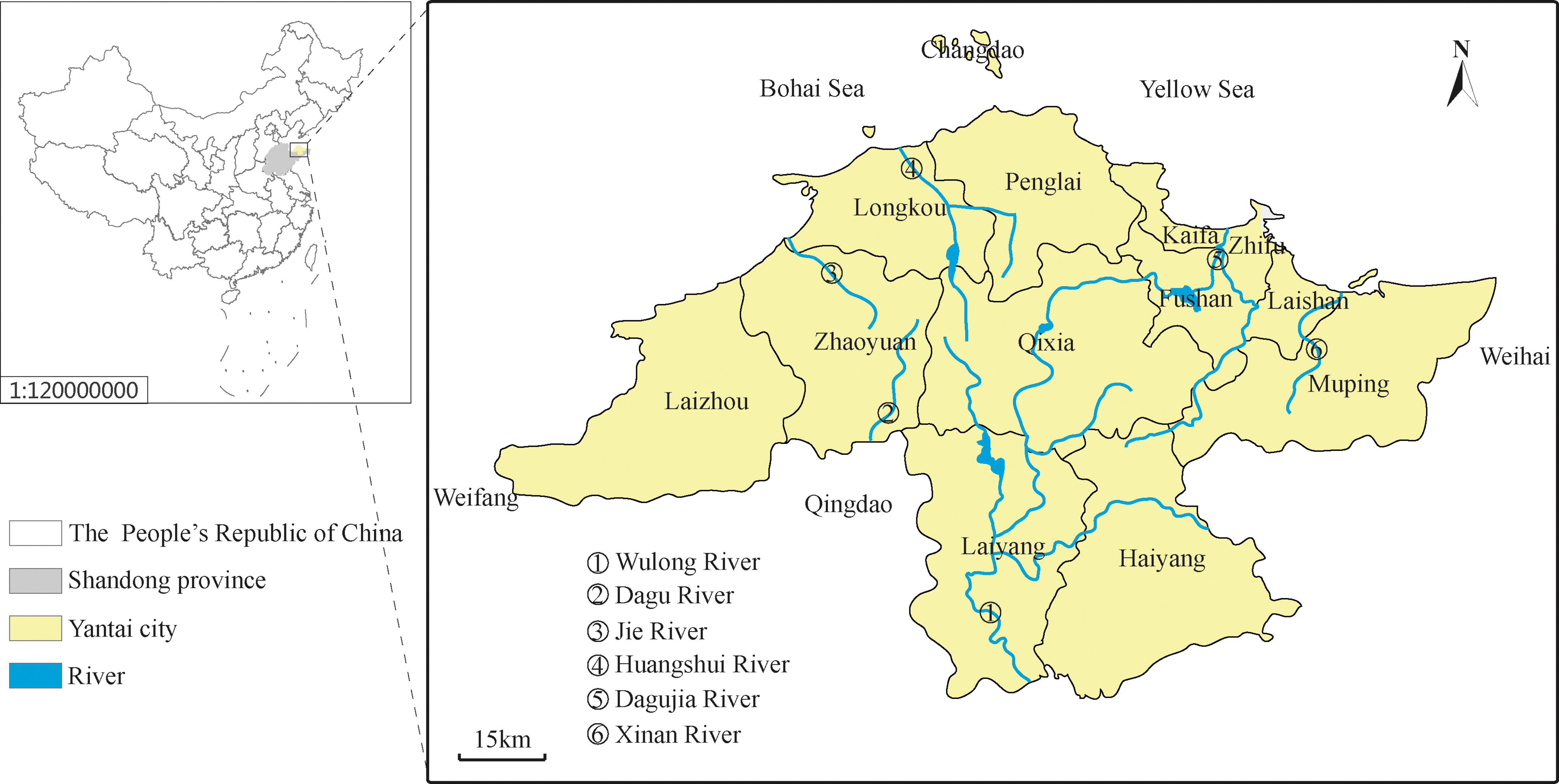
Location of Yantai in Shandong province, China. The names of 13 counties are labeled above, and the 6 major river systems associated with Anopheles sinensis breeding are marked in blue.
Data acquisition
In this study, the data before 2004 were collected from annual paper-based surveillance data and compilation of information on the elimination of malaria (Wang et al. 2010, Chen et al. 2015). Since 2004, each case that has been obtained through the Infectious Diseases Information Reporting Management System (IDIRMS;
Case types
Indigenous cases refer to malaria transmitted by mosquitoes in endemic areas of China (Chen et al. 2015). Imported malaria cases must meet all of the following criteria: a diagnosis of malaria and a travel history during the malaria transmission season and symptom development within 1 month after returning to China during the local transmission season (Kong et al. 2017, Zhang et al. 2018).
Diagnostic approach
Clinically diagnosed cases were defined as patients with typical malaria symptoms, including periodic chills, fever, and sweating, as well as suspected malaria patients with atypical attack cycles that were controlled by antimalarial treatment. Laboratory-confirmed cases were defined by the use of any laboratory test, including microscopic examination of Giemsa-stained thick and thin blood smears, rapid diagnostic tests, and polymerase chain reaction (Adah et al. 2018, Wogu and Nduka et al. 2018).
Malaria surveillance
Blood examination for fever patients
From 1951 to 1973, the outpatient clinics of medical institutions of various levels in Yantai mainly diagnosed malaria cases with clinical symptoms. During the period from 1974 to 1985, Yantai medical personnel carried out a Plasmodium examination for four kinds of fever patients (clinically diagnosed as malaria, suspected malaria, or fever with unknown causes, and cold) (Dian 2004). Since 1986, the city has focused on blood examinations for Plasmodium for three kinds of fever patients (clinically diagnosed as malaria, suspected malaria, or unexplained fever) (Xie et al. 2015). Since the initiation of malaria elimination activities in 2010, the blood examination procedure for fever patients has been further standardized.
Mosquito monitoring
The malaria elimination action plan was launched in 2010, and in accordance with the province's unified deployment of media monitoring points and the requirements of the Shandong Province Media Investigation Implementation Plan, Yantai conducted media investigation and monitoring in Longkou from 2010 to 2016. This required twice-per-month monitoring of the population structure and density of Anopheles mosquitoes attracted to light traps, and the interval between two adjacent monitoring events was 15 days. Monitoring started at the end of April and continued until two consecutive monitoring events failed to catch mosquitoes.
Statistical analysis
A retrospective analysis was performed using Microsoft Office Excel 2010 (Microsoft Corp., Redmond, WA) and SPSS Version 24.0 software for Windows (SPSS, Inc., Chicago, IL).
Results
Overall epidemiologic overview
From 1951 to 2017, a total of 81,286 malaria cases were reported in Yantai, with an incidence of 954.42/100,000. In the early days of the founding of the People's Republic (1951–1959), there were 1286 cases. From 1960 to 1979, the highest rate of malaria incidence was reported, with a total of 78,850 cases, and two peaks occurred mainly in 1966 (120.93/100,000) and 1970–1972 (366.12/100,000). The period from 1980 to 1985 was the period of basic malaria elimination, and the average incidence was 1.55/100,000 per year. The consolidation stage of the postmalaria prevention and treatment stage occurred from 1986 to 2009. During this period, the annual incidence of malaria remained below 10 cases, and the incidence was controlled at a low level of 0.00–0.12/100,000; most reported cases were imported cases. The last indigenous recurrence case was a case of P. vivax reported in Penglai in 2008, after which no indigenous cases occurred for 9 consecutive years. During the malaria elimination phase from 2010 to 2017, a total of 129 imported cases of malaria were reported, and one patient died of P. falciparum in 2014 (Fig. 2).
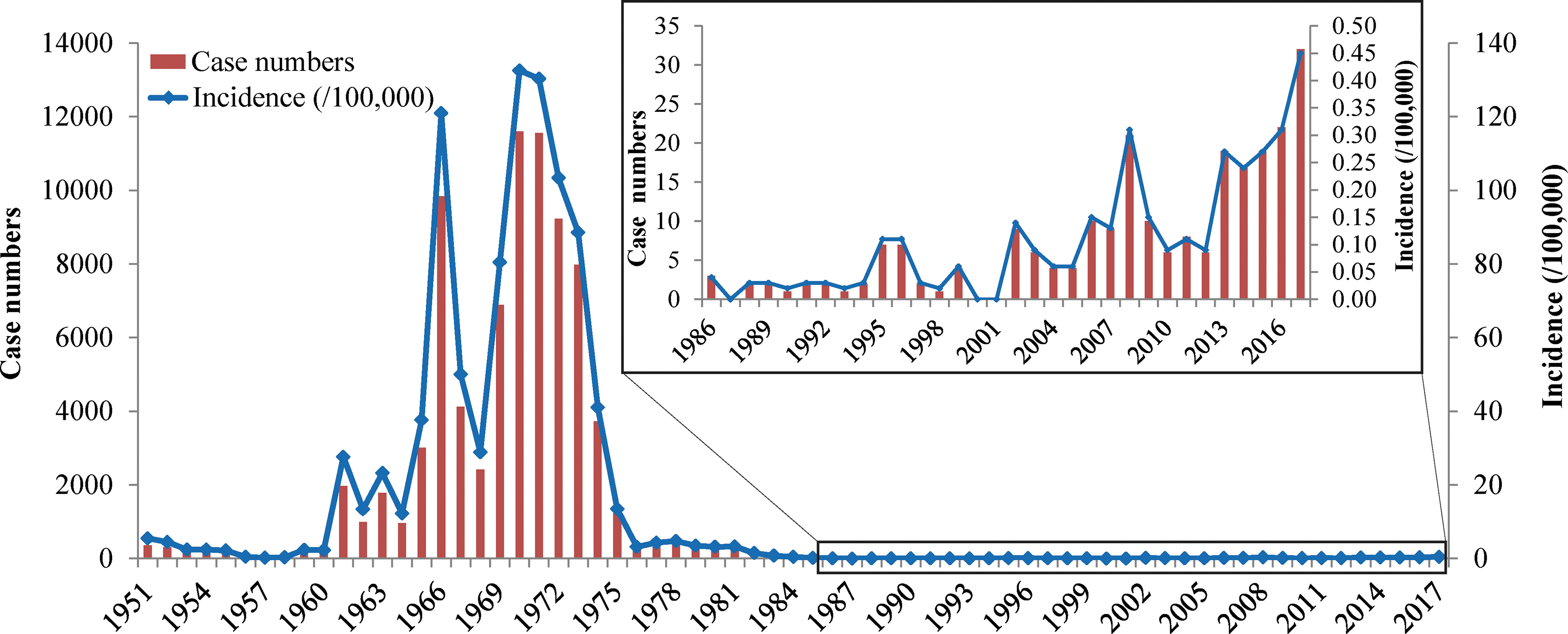
Malaria case numbers and incidence reported between 1951 and 2017, Yantai.
Plasmodium species composition
From 1951 to 2017, four species of Plasmodium (P. vivax, P. falciparum, P. ovale, and P. malariae) were identified from 81,286 malaria cases. Before 2004, all cases of malaria were caused by P. vivax infection and accounted for 99.80% (81,099/81,286) of the total cases. Since 2004, cases of P. falciparum infection have been reported, and their proportion has increased annually. From 2010 to 2017, 80.60% (104/129) of cases were reported as P. falciparum, and it became the main infective agent of malaria cases. Furthermore, one case of P. ovale and one case of P. malariae were reported for the first time in 2013; P. malariae has not been reported since, and nine cases of P. ovale were reported from 2014 to 2017 (Table 1).
Statistics on Different Plasmodium Species Between 1951 and 2017, Yantai
Malaria surveillance
Blood examination in fever cases
From 1951 to 1973, 73,868 cases of malaria were diagnosed mainly with clinical symptoms. A total of 293 malaria microscopy stations were established from 1974 to 1985, and 120,612 patients with four kinds of fever were diagnosed. A total of 7180 patients with P. vivax were diagnosed; 5866 cases were pathologically diagnosed, and 1314 cases were clinically diagnosed. A total of 582,297 patients with three kinds of fever were tested for Plasmodium between 1986 and 2009 and 109 of which were diagnosed as positive. From 2010 to 2017, the city's cumulative blood tests for three kinds of fever patients were administered 116,034 person-times, and the positivity rate was 0.46%.
Mosquito monitoring
From 2010 to 2016, a total of 14,255 mosquitoes belonging to three genera and four species were collected from Longkou, including Culex pipiens pallens, Culex tritaeniorhynchus, Aedes albopictus, and An. sinensis. Among the collected species, the predominant species collected was Cx. pipiens pallens, accounting for 65.06% (9275/14,255) of the total number of mosquitoes, followed by An. sinensis, accounting for 20.09% (2949/14,255). The capture rates of Ae. albopictus and Cx. tritaeniorhynchus were similar and accounted for 6.78% (967/14,255) and 6.58% (938/14,255) of the total number of mosquitoes, respectively. In addition, some other mosquito species were captured, accounting for 0.88% (126/14,255) of the total (Table 2).
Number and Categories of Mosquito-Borne Monitoring Between 2010 and 2016, Longkou
Distribution of imported cases
Geographic distribution
A total of 129 malaria cases were reported in Yantai from 2010 to 2017, and all cases were imported from other countries. Approximately 93.80% (121/129) of patients had travelled to African countries; 117 cases were associated with 17 countries, and the source countries of 4 imported cases have not yet been identified. The six source countries with the most imported cases accounted for 66.94% (81/121) of the total cases from Africa, with 35.54% (43/121) from Equatorial Guinea, 9.92% (12/121) from Ghana, 8.26% (10/121) from Tanzania, and 6.61% (10/121) cases from Angola and Congo. The remaining eight cases were imported from four countries in Asia; three patients were infected in Indonesia, two cases were infected in Pakistan, two cases were infected in Myanmar, and one patient was infected in Cambodia (Fig. 3).
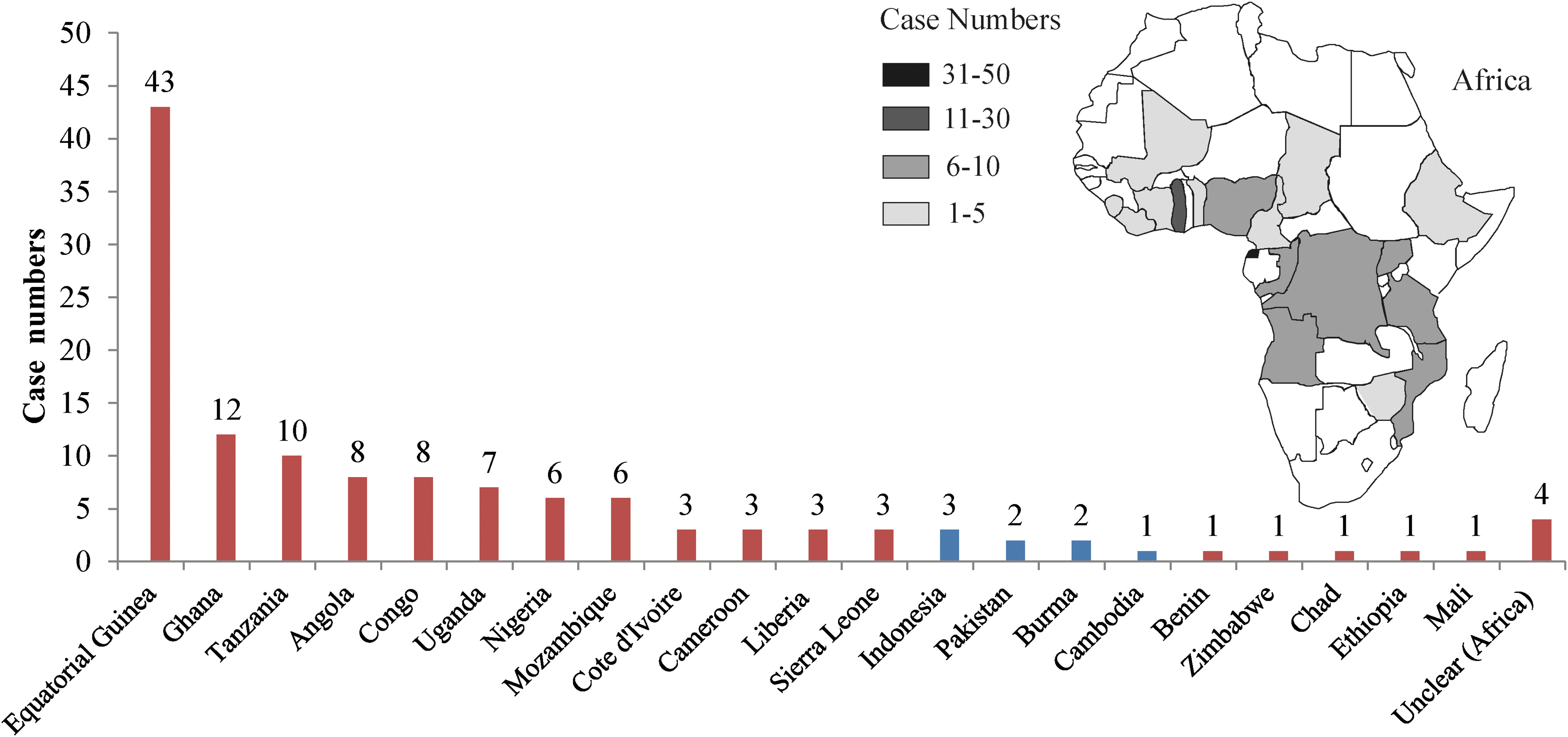
Regional origin of imported malaria cases from 2010 to 2017 in Yantai. The red and blue columns represent malaria cases from Africa and Asia, respectively. Geographical map shows the distribution of imported malaria cases from Africa, 2010–2017. Gray scale difference represents the level of imported malaria from different areas in Africa.
Temporal distribution
From 1962 to 2009, the peak incidence occurred from June to September, accounting for 78.85% (61,212/77,629) of the total cases. According to the monthly imported case reports from 2010 to 2017, there were no obvious seasonal characteristics for the onset time. The number of cases was the highest from November to January of the following year, accounting for 28.68% (37/129) of the total cases. The number of cases from May to July accounted for 27.91% (36/129) of the total cases. Thirty-two cases were reported from August to October, accounting for 24.81% (32/129) of the total cases, and the number of cases in February to April was small, accounting for 18.60% (24/129) of all cases (Fig. 4).
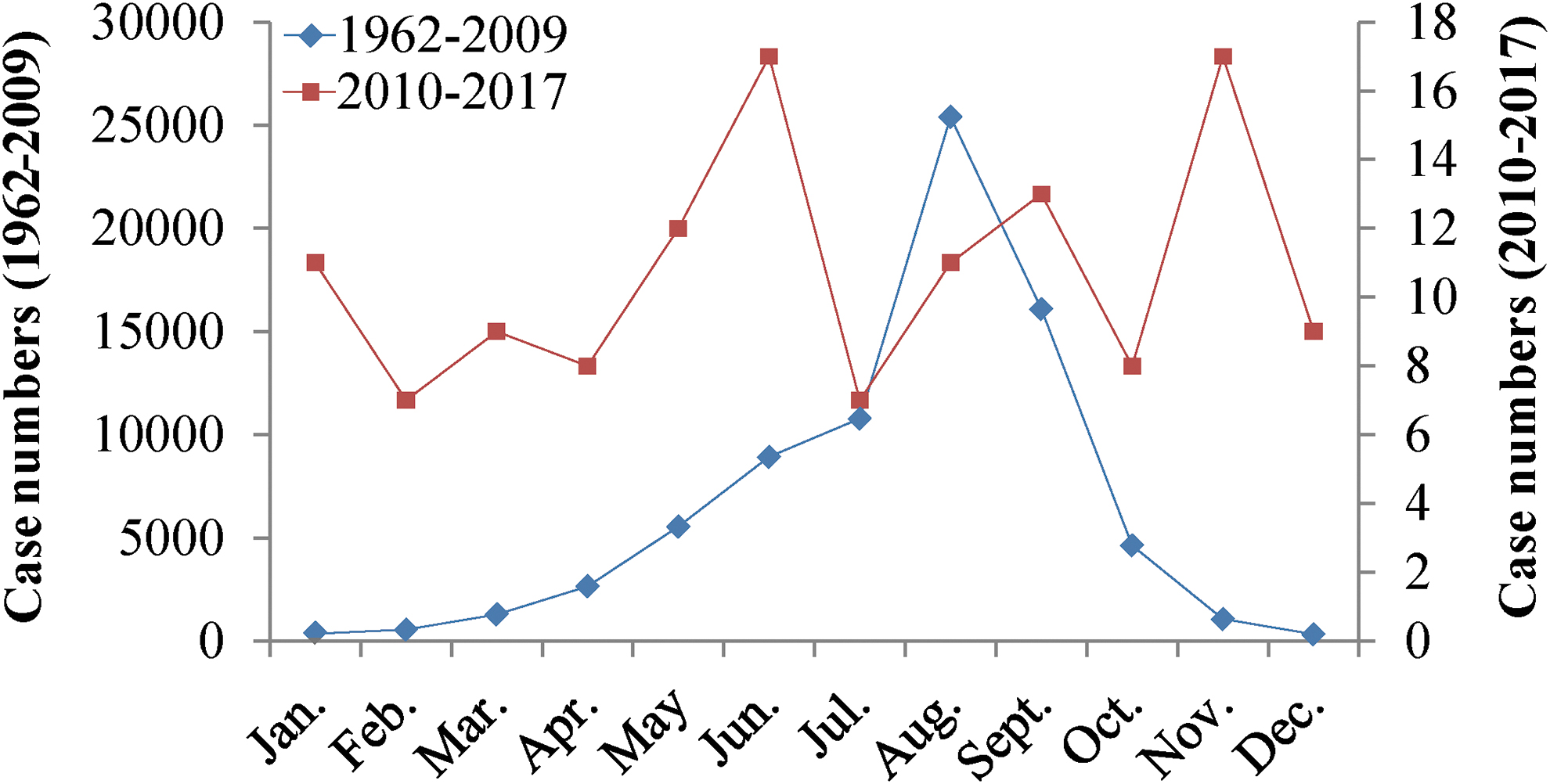
Monthly distributions of imported malaria cases. Different colors of fold line show the change trend of case numbers monthly in the two periods (1962–2009/2010–2017).
Demographic features
From 2010 to 2017, males accounted for the vast majority of imported malaria cases (127/129, 98.45%); women accounted for only 1.55% (2/129). The youngest patient was 19 years old, and the oldest patient was 60 years old. A total of 68.28% (88/129) of the cases occurred in patients aged 30–49 years. Furthermore, the main types of patients were migrant workers and farmers, accounting for 34.10% and 31.80% of all patients, respectively.
Discussion
Malaria remains an important parasitic infectious disease that threatens the health of residents in many developing communities. Therefore, it is extremely important to explore the characteristics of the current malaria prevalence situation and to make reasonable malaria control and elimination measures. Yantai used to be a high P. vivax-malaria-endemic area in Shandong Province with An. sinensis as the single vector due to the numerous small- and medium-sized rivers in the territory. The warm, temperate continental monsoon climate and the influence of the marine climate, compared with the inland areas of the same latitude, result in moderate rain, humid air, and a mild climate, which are very suitable for mosquito growth (Gouagna et al. 2011).
In 1966, Yantai experienced the highest amount of rainfall since the founding of the People's Republic of China, and the flood area was 1.18 million mus. Because the river had not been effectively modified in time, mosquito larvae multiplied rapidly during the warming season after the water source was contaminated (Shi et al. 2017); in addition, the reduction of livestock population was caused by the decline in living standards of residents, coupled with the summer and autumn, most residents have the habit of sleeping outdoors to enjoy the cool, and the protection rate of mosquito nets is low, the exposure of human mosquitoes increased substantially, and the incidence of malaria increased significantly, which triggered the first malaria pandemic (Fu et al. 2002). Since the first malaria outbreak, the city has organized a strong antimalaria team to control malaria transmission. Therefore, the incidence of malaria has decreased dramatically since 1967. However, most of the antimalaria teams were disbanded during the political movement, and the malaria control measures were not well implemented. Coupled with population movement and the spread of infectious sources, the incidence of malaria increased again in 1970–1972, resulting in the second malaria pandemic (Fu et al. 2002). Thus, the entire city actively carries out prevention and treatment activities after malaria outbreaks, including the initiation of a large number of patriotic health campaigns, elimination mosquito breeding spots, administration of timely treatments for current patients, and implementation of national preventive drug treatment programs. In addition, with the improvement of rural economic conditions, the cultural level and medical and health conditions of the masses have been greatly improved, housing conditions have improved significantly, and the protection rate of mosquito nets has also increased substantially. There is basically no habit of sleeping outside, which has significantly reduced mosquito contact opportunities. Moreover, the city has been increasing the number of malaria microscopy stations to actively carry out blood malaria examinations, and thus, the incidence of malaria has decreased significantly since 1974. Until August 1985, Yantai passed the expert assessment of the Health Department of Shandong Province and reached the “Basic Malaria Elimination Standards” of the Ministry of Health. The case of P. vivax malaria in Penglai reported in December 2008 was the last indigenous recurrence.
After 2010, with the increase in international trade and the number of people going abroad, especially to Africa and Southeast Asia, the number of imported cases gradually increased. Demographic features of imported malaria indicate that males who were 30–49 years old were at a high risk for malaria infection. The main occupations of imported malaria patients were migrant workers and farmers since they frequently engage in activities such as construction, logging, mining, and farming in Africa and Southeast Asian countries where malaria is endemic, and they are vulnerable to female Anopheles mosquitoes at peak biting times, which can result in disease and even death (Wang et al. 2016).
The temporal distribution of cases suggested that the main peak incidence of previous indigenous cases was from June to September, and the seasonal activity of An. sinensis in Shandong Province ranged from June to September due to suitable rainy and hot weather conditions. However, cases from 2010 to 2017 do not show obvious seasonal characteristics. The incidence was relatively concentrated from May to January of the following year, which may be because migrant workers and farmers usually return to China from malaria-endemic countries during holidays such as the Spring Festival, May Day, and the Mid-Autumn Festival (Wardrop et al. 2013, Wang et al. 2018).
In this study, indigenous cases were caused by infection with P. vivax, and most of the imported cases were caused by infection with P. falciparum, which is the most pathogenic type of malaria with the highest incidence in sub-Saharan Africa (Kevin Baird 2013). Since P. vivax vectors can survive at lower temperatures and higher altitudes, P. vivax has a broader geographic range than P. falciparum. Compared to these two dominant species, the relative numbers of P. malariae and P. ovale are relatively few and have not been fully studied. P. ovale is mainly distributed in sub-Saharan Africa (Collins and Jeffery et al. 2005), and P. malariae is found in tropical Africa, where it sometimes occurs as a coinfection with P. falciparum (Autino et al. 2012). Compared to the life-threatening P. falciparum, P. vivax and P. ovale are seemingly much less virulent. However, P. vivax and P. ovale commonly lead to the recurrence of malaria, meaning patients with this parasite have a risk of complications and possible mortality (Kevin Baird 2013, Lawpoolsri et al. 2019). Therefore, clinicians and public health workers should strengthen the follow-up treatment regimen for P. vivax and P. ovale (Zhang et al. 2018).
In China, migrant workers and farmers form a large proportion of the population. With the awareness of population health and the promotion of antimalaria education, this population has a better understanding of malaria transmission and infection symptoms, but the application of preventive measures, the use of antimalarial drugs, and the implementation of antimalarial behavior (the use of mosquito nets with insect repellents and the use of repellents for exposed sites) are low, which is related to weak cultural standards, limited economic conditions, and low medical compliance. Therefore, the coverage of malaria prevention education should be expanded subjectively to provide economical, effective, and easy-to-use health education for migrant workers. Objectively, labor service companies should be urged to increase their input in malaria prevention and fulfill their corresponding responsibilities for the protection of labor personnel against malaria.
Since the launch of the Malaria Action Plan in 2010, Yantai has strictly followed the China Malaria Eradication Action Plan (2010–2020) and Shandong Malaria Implementation Plan requirements and has achieved progress with respect to the prevention and control of malaria. The collective measures are as follows: (1) establish a sound malaria prevention network and conduct epidemiological training for malaria prevention personnel on a regular basis; (2) increase the number of malaria microscopy stations that actively carry out blood tests for fever patients, improving pathogen diagnosis; (3) standardize the treatment for malaria patients to control and eliminate sources of infection; (4) promote mosquito-borne prevention, investigation, and monitoring strategies to eliminate malaria transmission routes; (5) vigorously promote antimalaria knowledge; and (6) strengthen the management system of the mobile population.
There was one P. falciparum malaria patient from Africa who died from multiple organ failure due to their critical condition. This incident has undoubtedly sounded the alarm for us. Although Yantai has achieved a certain success in eradicating malaria, there are still many deficiencies and difficulties in the process.
Yantai needs to strictly follow the “1-3-7” malaria epidemic management mode to further strengthen the management of the epidemic and standardize the investigation and eradication strategies associated with the epidemic (Li et al. 2016, Wang et al. 2017), such as strengthening health education before people depart from the region and border screening for malaria after people enter the region. (Riddle et al. 2017, Xu et al. 2017). In addition, the early accurate detection of malaria and timely clinical treatment play a crucial role in reducing malaria morbidity and mortality and drug resistance and improve malaria control, so it is important to ensure universal diagnostic testing procedures for all suspected malaria cases (Chen et al. 2012), provide quality-assured treatment for all patients, monitor the safety and efficacy of antimalarial drugs, and manage antimalarial drug resistance. Furthermore, to optimize the national malaria response, it is essential to strengthen the health system as a whole and improve the health care environment, which is essential for reducing the burden of disease and reducing the potential for the further spread of these parasites.
Conclusions
Although there are no indigenous malaria cases in Yantai, the increase in imported malaria cases from Africa and Southeast Asia remains a major threat. If targeted precautions are not taken, the potential risks of imported malaria could cause an unpredictable disaster in the city of Yantai. Therefore, it is necessary to eliminate potential malaria reservoirs, block malaria transmission routes, and prevent malaria outbreaks caused by imported pathogens. Subsequently, the government should continue to emphasize the elimination of malaria and guarantee effective funding. Furthermore, understanding the risk factors for malaria infection is critical to formulate a reasonable strategic planning program. Attention should be given to strengthening capacity building in malaria monitoring, emergency response, diagnosis, and treatment. Finally, while eliminating malaria, multisectoral research and cooperation, especially international cooperation mechanisms in the border areas, should be strengthened and encouraged.
Footnotes
Acknowledgment
The authors thank all of the professional staff involved in malaria surveillance activities in China for their valuable support.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Natural Science Foundation of China (grant no. 81672059, 81871685, and 81702034), Shandong Province Key Research and Development Projects (grant no. 2018GSF118040), and the Innovation Project of Shandong Academy of Medical Sciences.