
Abstract
Although scrub typhus and murine typhus are well-described tropical rickettsial illnesses, especially in Southeast Asia, only limited evidence is available for rickettsia-like pathogens contributing to the burden of undifferentiated febrile illness. Using commercially available kits, this study measured immunoglobulin G (IgG) antibody seroprevalence for Coxiella burnetii, Ehrlichia chaffeensis, Bartonella henselae, Anaplasma phagocytophilum, and spotted fever group rickettsiae (SFGR) in 375 patients enrolled in undifferentiated febrile illness studies at Chiangrai (northern Thailand) and Mae Sot (Thai–Myanmar border). Ehrlichia and SFGR were the most common causes of IgG seropositivity. A distinct relationship between age and seropositivity was found in Chiangrai with acquisition of IgG titers against Ehrlichia, Bartonella, Anaplasma, and SFGR in young adulthood, suggesting cumulative exposure to these pathogens. At Mae Sot, high early IgG titers against Ehrlichia and SFGR were common, whereas Anaplasma and Bartonella IgG titers increased at 50–60 years. Q fever associated with low IgG positivity at both study sites, with significantly higher prevalence at 30 years of age in Chiangrai. These data suggest that other rickettsial illnesses could contribute to the burden of febrile illness in Thailand and possibly adjacent regions. Improved diagnostics and better understanding of antibody longevity and cross-reactivity will improve identification and management of these easily treatable infectious diseases.
Introduction
R
Febrile illness attributable to Coxiella burnetii and Bartonella henselae have been described in Thailand, including recent reports of infective endocarditis for both zoonotic pathogens (Suputtamongkol et al. 2003, Pachirat et al. 2011, 2012, Watt et al. 2014). Although Anaplasma phagocytophilum (causative agent of human granulocytic anaplasmosis) and Ehrlichia chaffeensis (causative agent of human monocytic ehrlichiosis) have been identified in ticks from the Thai–Myanmar border and in Bangkok, to date no human data on seroprevalence or clinical disease is available for these agents (Parola et al. 2003a, Foongladda et al. 2011). However, one report provides serological evidence of E. chaffeensis infections in a group of healthy volunteers in western Thailand (Heppner et al. 1997). Mammalian hosts include rodents, cats, and dogs for B. henselae and goats, sheep, and domestic cattle for Coxiella burnetii (Bhengsri et al. 2010, Yingst et al. 2013). Clinical and serologic recognition of canine ehrlichiosis among dogs in separated regions of Thailand is established (Davidson et al. 1975, Jirapattharasate et al. 2012).
These data are suggestive that other rickettsial illnesses could contribute to the burden of febrile illness in Thailand (and adjacent regions). Using commercially available kits, this study has determined the immunoglobulin G (IgG) antibody seroprevalence for C. burnetii, B. henselae, A. phagocytophilum, E. chaffeensis, and spotted fever group rickettsiae (SFGR) in human patients from well-characterized prospective undifferentiated febrile illness cohorts.
Materials and Methods
A total of 375 serum samples were collected from two febrile illness studies recently performed in Chiangrai (August, 2006, to August, 2007) and Mae Sot, Thailand (March to May, 2011) (Paris et al. 2011, Watthanaworawit et al. 2013). The Chiangrai study previously reported 34% cases with acute scrub typhus infections (n=161) and the Mae Sot study (n=180) previously reported 3.9% and 6.1% of patients with confirmed acute scrub or murine typhus, respectively (Paris et al. 2011, Watthanaworawit et al. 2013).
The first study recruited 188 hospitalized patients over 15 years old with acute fever of less than 2 weeks duration, no evidence of primary focus of infection, and three negative malaria blood smears. These patients provided written informed consent over one calendar year (August, 2006, to August, 2007) at Chiangrai Prachanukhru hospital. Ethical approval for this study was granted by the local ethics committee of Chiangrai Hospital, the Faculty of Tropical Medicine, Mahidol University, and the Thai Ministry of Public Health.
The second study recruited 187 patients into an undifferentiated fever study between March and August of 2011 at three medical clinics for Burmese migrants and refugees on the Thailand–Myanmar (Burma) border in rural Tak province of northwestern Thailand. Of the three clinics, Wang Pha and Mawker Thai clinics are the two largest and provide health care for the migrant population from Myanmar who live and work along the border. Wang Pha is approximately 30 km north of Mae Sot, whereas Mawker Thai is approximately 60 km south of Mae Sot. The third site was Maela temporary shelter and is the largest camp for refugees from Myanmar on the Thailand–Myanmar border housed in an area of 4 km2. This site is located in hills adjoining the Myanmar border, approximately 70 km north of Mae Sot. Patients aged at least 5 years old and presenting to these clinics with an undifferentiated febrile illness were eligible for inclusion in the study. Ethical approval for this study was granted by the Faculty of Tropical Medicine, Mahidol University and the Oxford Tropical Research Ethics Committee (OxTREC), UK.
Serology was performed for the detection of C. burnetii, E. chaffeensis, B. henselae, and A. phagocytophilum IgG antibodies using indirect immunofluorescence assay (IFA) following the manufacturer's instructions for sample testing and interpretation of results in the context of a seroprevalence study, with details provided below. IFA slides were read blinded by two experienced operators. In cases where there was disagreement, a third experienced operator was used to make a final diagnosis.
For the C. burnetii IgG IFA (cat. no. QG-120, Fuller Laboratories, Fullerton, CA), samples were screened at a 1:16 dilution against C. burnetii phase I and phase II antigens, and positive samples were diluted two-fold from 1:16 to1:256. Acute infection was characterized as samples positive at 1:16 with an end point titer ratio of phase II antigens greater than phase I antigens or a ≥1:256 phase II antigen titer. Chronic or previous infections were characterized by an end point titer ratio of phase I antigens greater than that against the phase II antigen. In this study, samples that met the chronic or previous infection criteria were considered positive.
For the E. chaffeensis IgG IFA (cat. no. ECHG-120, Fuller Laboratories, Fullerton, CA), samples were screened at a 1:64 dilution. Positive samples at 1:64 dilution or greater were considered to reflect infection at an undetermined time with E. chaffeensis or related organism and were considered positive in the context of this study. The manufacturer noted the limitation that antibodies against E. canis and E. ewingii can cross-react strongly in this test.
For the A. phagocytophilum IgG IFA (cat. no. EEG-120, Fuller Laboratories, Fullerton, CA), samples were screened at a 1:80 dilution and titrated further if positive. Serum titers from 1:80–1:320 suggested titers before or after peak titers associated with A. phagocytophilum infection or cross-reactivity with a related organism. In this study, samples with titers ≥1:80 were considered positive. The manufacturer noted the limitation that variable strength cross-reactions with E. chaffeensis may occur.
For the B. henselae IgG IFA (cat. no. BHG-120, Fuller Laboratories, Fullerton, CA), samples were screened at a 1:64 dilution and titrated further if positive. Serum titers from 1:64 or greater suggest recent or active infection and were considered positive in this study. The manufacturer noted the limitation that other Bartonella species may produce type-specific reactions.
Samples were tested for SFGR antibodies using an SFGR EIA IgG Antibody Kit (cat. no. SFG-96K, Fuller Laboratories, Fullerton, CA). Samples were screened at a 1:100 dilution. The manufacturer's recommended method for interpretation is as follows, “A Cutoff Calibrator is provided for discrimination between reactive and non-reactive sera. By dividing the OD values of test sera by the OD values of the Calibrator, an index value can be derived where the Calibrator is set at an index of 1.0. Indices from 0.8 to 1.2 may be considered equivocal (assumes %CV of 20%). Indices above 1.2 are then considered positive and those below 0.8 are considered negative.” Samples with indices ≥1.2 were considered positive in this study. The manufacturer notes, “This procedure detects group-specific antibody and is, thus, unable to differentiate between the reactivity to various members of the spotted fever group. Reactivity to typhus group or scrub typhus is, in general, not detected.”
Statistical analysis was performed using Stata/IC software (v. 13.0, Statacorp, College Station, TX). The command prtest was used to compare equality of positivity proportions for significant difference (p ≤ 0.05) between study sites. To compare equality of positivity at each age category (0–10 years, 11–20 years, and so on), the Kruskal–Wallis rank test was used.
Results
Ehrlichia and SFGR were the most common causes of IgG seropositivity at both study sites. The percentages of IgG-positive samples against the specified zoonotic pathogens are presented in Table 1. The highest prevalence documented was for E. chaffeensis in Mae Sot (60.4%), which was significantly higher (p≤0.001) than in Chiangrai (11.7%). Significant differences in antibody prevalence between the study sites were found for B. henselae (p=0.007; Chiangrai 18.1% cf. Mae Sot 8.6%) and C. burnetii, (p=0.002; Chiangrai 6.4% cf. Mae Sot 0.5%). SFGR positivity was relatively high at both sites (Chiangrai 33% cf. Mae Sot 27.3%) and not significantly different. A. phagocytophilum positivity was similar and relatively low at both sites (Chiangrai 5.3% cf. Mae Sot 3.7%).
Values in
IgG, immunoglobulin G.
Multiple positivity or evidence of IgG antibody for more than one infection per person was found in 15% and 25% of cases with multiple seropositivity at Chiangrai and Mae Sot, respectively, and 3% of all cases with evidence for triple seropositivity (Table 2). The most common multiple positivity (Table 3) in Chiangrai was SFGR/B. henselae (8.5%) and in Mae Sot SFGR/E. chaffeensis (20.2%).
This table summarizes the multiple seropositivity results found at the two study sites. The upper right triangle of data represents positive results from Mae Sot, whereas the lower left triangle represents Chiangrai. Data are actual numbers, with percentages shown in parentheses.
A distinct relationship between age and seropositivity was found in Chiangrai, with acquisition of IgG titers against E. chaffeensis, B. henselae, A. phagocytophilum, and SFGR rising rapidly between 30–40 years of age. At Mae Sot, seroprevalences manifested similarly with high early IgG titers against E. chaffeensis and SFGR positivity peaking around 40 years, but B. henselae and A. phagocytophilum IgG titers rising later at 50 years of age (Fig. 1). Mae Sot SFGR seropositivity per age group demonstrated a significant difference at 20–30 years, the age of peak rural activity, when compared to Mae Sot (p≤0.001).
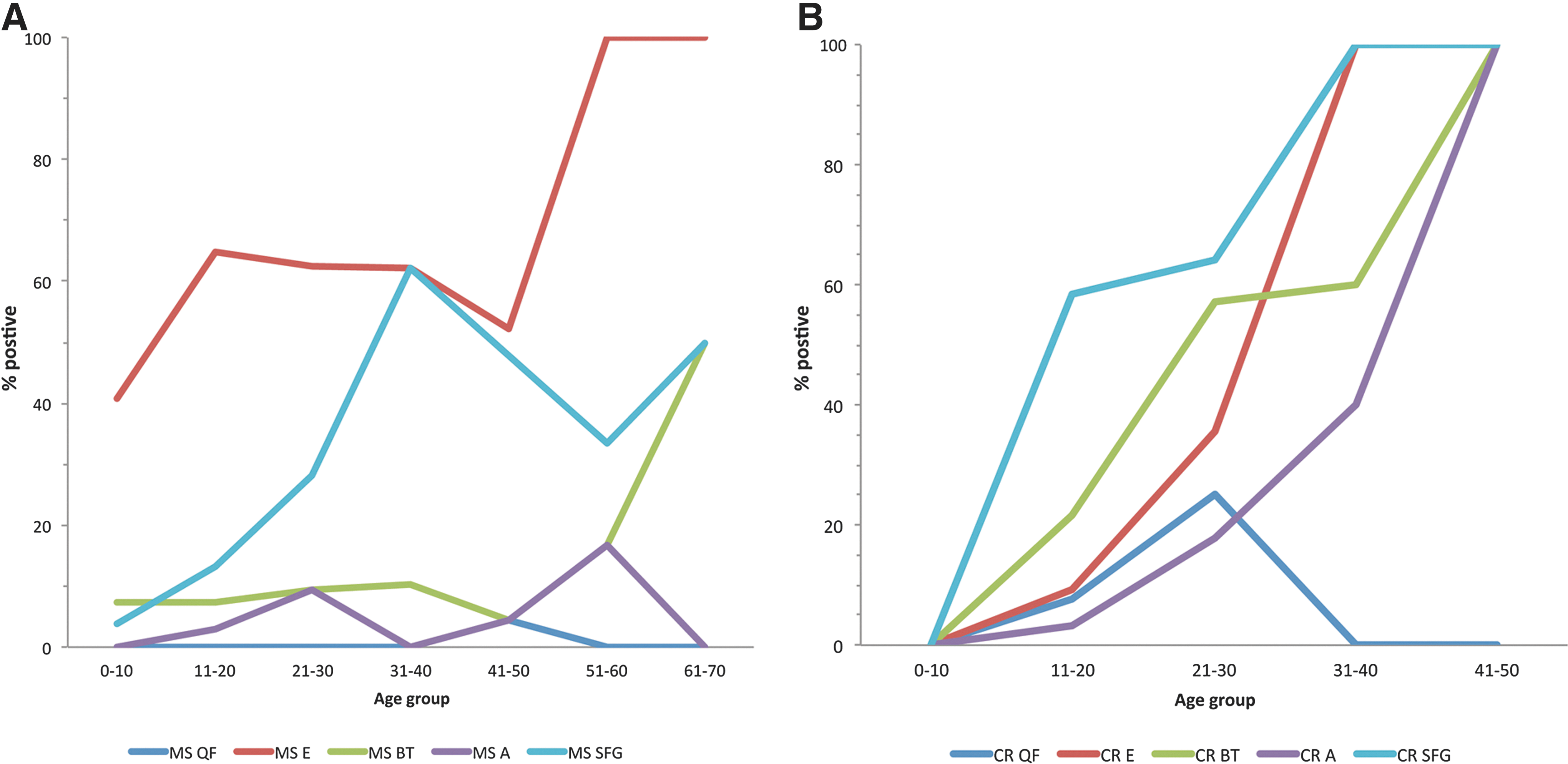
Age group seroprevalence of C. burnetii, E. chaffeensis, B. henselae, A. phagocytophilum, and SFGR IgG titers in patient samples from Mae Sot (
Seroprevalence of IgG against C. burnetii results was demonstrated following variations of antibodies associated with infection phase; one, nine, and five patients showed evidence of antibodies against phase I, phase II, and both phases antigens, respectively, at Chiangrai and a single patient at Mae Sot was positive for both infection phases. These findings are suggestive that approximately 5% (9/190) of febrile patients in Chiangrai could have presented with active infections. Q fever was generally associated with low IgG positivity across the age groups at both study sites; however, a significantly higher prevalence was observed at 30 years of age in Chiangrai (p=0.025).
Discussion
This study provides human seroprevalence data on hitherto poorly described zoonotic pathogens at two study sites in Thailand. The finding of E. chaffeensis, SFGR, and also B. henselae as the most common causes of IgG seropositivity in this study suggests that these pathogens should be considered in the differential diagnosis of undifferentiated febrile illness. In view of the easily treatable nature of these diseases, further clinical investigations of these potentially serious infections are warranted, and future studies addressing “causes of illness” attributable to these pathogens should consider diagnostics with a high level of confidence, such as culture, molecular tools, and/or paired serology, if possible, combined with subsequent molecular characterization (Phommasone et al. 2013).
Significant differences in antibody prevalence between the study sites were found for B. henselae, C. burnetii, and E. chaffeensis. Furthermore, there was a distinct relationship between age and seropositivity for A. phagocytophilum, B. henselae, E. chaffeensis, and SFGR in this study (Table 1 and Fig.1). The stratification of IgG titers into age groups highlighted that patients increased their exposure to these pathogens and acquired IgG antibodies over time. The humoral responses to SFGR and E. chaffeensis dominated in early adulthood in the Mae Sot region, when exposure to rural activities is highest. However these titers remained high, suggestive of either continuous exposure and/or high longevity of antibodies. In contrast, low positivity rates were followed by a distinct increase in anti–B. henselae IgG seropositivity in the oldest age group. A. phagocytophilum and C. burnetii titers were generally low in the Mae Sot samples, whereas in Chiangrai A. phagocytophilum responses increased early, but not C. burnetii, which after a seropositivity peak at 20–30 years of age, dropped to zero in older patients. In the Chiangrai population all patients had previous exposure to A. phagocytophilum, E. chaffeensis, B. henselae, and SFGR by the age of 40, which is suggestive that these pathogens are more common than previously assumed.
Previous studies have examined the seroprevalence of rickettsial illnesses in Malaysia and provide evidence for murine typhus and SFGR exposure to be very common (Tay et al. 2000, Tay and Rohani 2002, Tay et al. 2003). Age groups under 21 years old had a lower seroprevalence of SFGR compared with the other age groups, similar to our observations, and very high seropositivity rates for SFGR were associated with rubber estate workers (Tee et al. 1999). In addition, other studies have also identified spotted fever group organisms in fever patients and vectors in similar locations, and therefore our results confirmed that SFGR are likely to contribute to the disease burden of undifferentiated fevers and should be a concern to people who live or visit these areas (Tay et al. 2003, Parola et al. 2003b, Parola et al. 2003c, Pickard et al. 2004, Jiang et al. 2005).
Patients with multiple seropositivity results to the evaluated pathogens were common and underline the cumulative exposure over time (Table 2). There was no statistically significant difference in the rates of IgG acquisition status between the sites (χ2 p=0.465). Overall, 30.5–47.3% of patients were seronegative at both sites for antibodies against the agents of the arthropod-borne diseases tested, whereas the majority of patients had either one (34.6–41.7%) or two (14.9–24.6%) seropositive results. Seropositivity was rare for either three (2.7–3.2%) or four diseases (0.5% in Chiangrai) (Table 2).
Although the longevity of IgG antibodies is not well established in these regions and reversion rates to seronegativity remain to be determined, it is likely that the increasing seropositivity rates across the age groups reflect a high level of cumulative exposure, as the IgG antibodies for these infections are normally long-lived and probably get “boosted” intermittently in endemic areas. In contrast, a high seroreversion rate would mean that the data represent an underestimation, due to the proportion of “false negatives” resulting from reversion to seronegativity. Interestingly, the seropositivity rates for anti–C. burnetii IgG antibodies in Chiangrai and the anti-SFGR IgG antibodies in Mae Sot declined in older age groups. Whether this phenomenon is attributable to increased seroreversion and whether loss of antibody over time occurs need to be investigated further (Fig. 1). In contrast, E. chaffeensis infections seem to be more prevalent from an early age in Mae Sot and tend to stay high into adulthood (Fig. 1).
Although this study was based on two well-characterized prospective patient cohorts, some limitations must be considered. First, the inclusion of febrile patients from hospitals may not accurately represent the typical cross-sectional findings of healthy populations because the active treatment–seeking behavior associated with hospitalized patients could associate with bias, i.e., a significant proportion of infections result in subclinical disease with manifestations that do not warrant seeking medical care. Second, the populations enrolled may not represent well the populations found throughout the northern and northwestern regions or that of Thailand as a whole. Third, serological cross-reactions between and within genera should be considered when interpreting results. The manufacturer clearly states in the product literature that the possibility of cross-reaction (false positivity) caused by E. chaffeensis antibodies in the A. phagocytophilum IFA, and the manufacturer highlighted that E. chaffeensis and B. henselae IFAs are not species-specific and positivity may be due to other members of the genera.
The data presented here highlight that etiologies of tropical rickettsial illnesses need to be considered beyond O. tsutsugamushi and R. typhi; however, the contribution of these pathogens to the burden of undifferentiated febrile illness in Thailand and potentially adjacent regions requires further clinical studies.
Conclusion
Our seroprevalence data suggest that other zoonotic pathogens could contribute to the burden of tropical rickettsial illnesses in Thailand and possibly adjacent regions. Improved diagnostics and better understanding of antibody longevity and cross-reactivity are necessary and will improve identification and management of these easily treatable but potentially serious infectious diseases.
Footnotes
Acknowledgments
We thank the Chiangrai Prachanukhao Hospital and Shoklo Malaria Research Unit (SMRU) teams for their assistance during the collection of specimens for this study. This work was supported in part by the Global Emerging Infections Surveillance and Response System, a Division of the Armed Forces Health Surveillance Centre, work unit number A1402, and the Wellcome Trust of the United Kingdom.
Author Disclosure Statement
No competing financial interests exist.
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, nor the US Government.
A.L.R. is an employee of the US Government and this work was prepared as part of his official duties. Title 17 U.S.C. §105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. §101 defines a US Government work as a work prepared by a military service member or employee of the US Government as part of that person's official duties.