
Abstract
Chikungunya virus (CHIKV) recently caused major urban outbreaks in central African countries such as the Democratic Republic of Congo (DRC), Cameroon, and Gabon. In Gabon, the tiger mosquito Aedes albopictus was shown to be the main CHIKV vector during the 2007 outbreak. This invasive Asian species was first identified in Gabon in early 2007, and was thought to be restricted mainly to coastal provinces where urban epidemic CHIKV foci were recorded. Here we report a CHIKV outbreak in a small cluster of villages isolated in the deep forest of southern Gabon, in which A. albopictus was the main vector. This observation indicates concomitant geographic and ecological spread of CHIKV activity and A. albopictus in remote environments in central Africa, as well as an enhanced risk of propagation of epidemic arboviruses.
Introduction
On April 12th, 2010 the local health authorities in Lastourville, the second largest town of Ogooué-Lolo province, southern Gabon, informed the Centre International de Recherches Médicales de Franceville (CIRMF) of numerous cases of a febrile arthralgic syndrome compatible with CHIKV infection in Ndangui, a cluster of small gold-washing villages. The Ndangui villages, located in the Mouloundou department of Ogooué Lolo province (L 13.0969-l 0.50131), are situated in deep rainforest 80 km north of Lastourville (Fig. 1), and are home to 640 people. Access to Lastourville is difficult, owing mainly to poor road conditions during the rainy season. In order to investigate this CHIKV-like outbreak, we conducted on-site medical and entomological surveys from April 21–29, 2010.
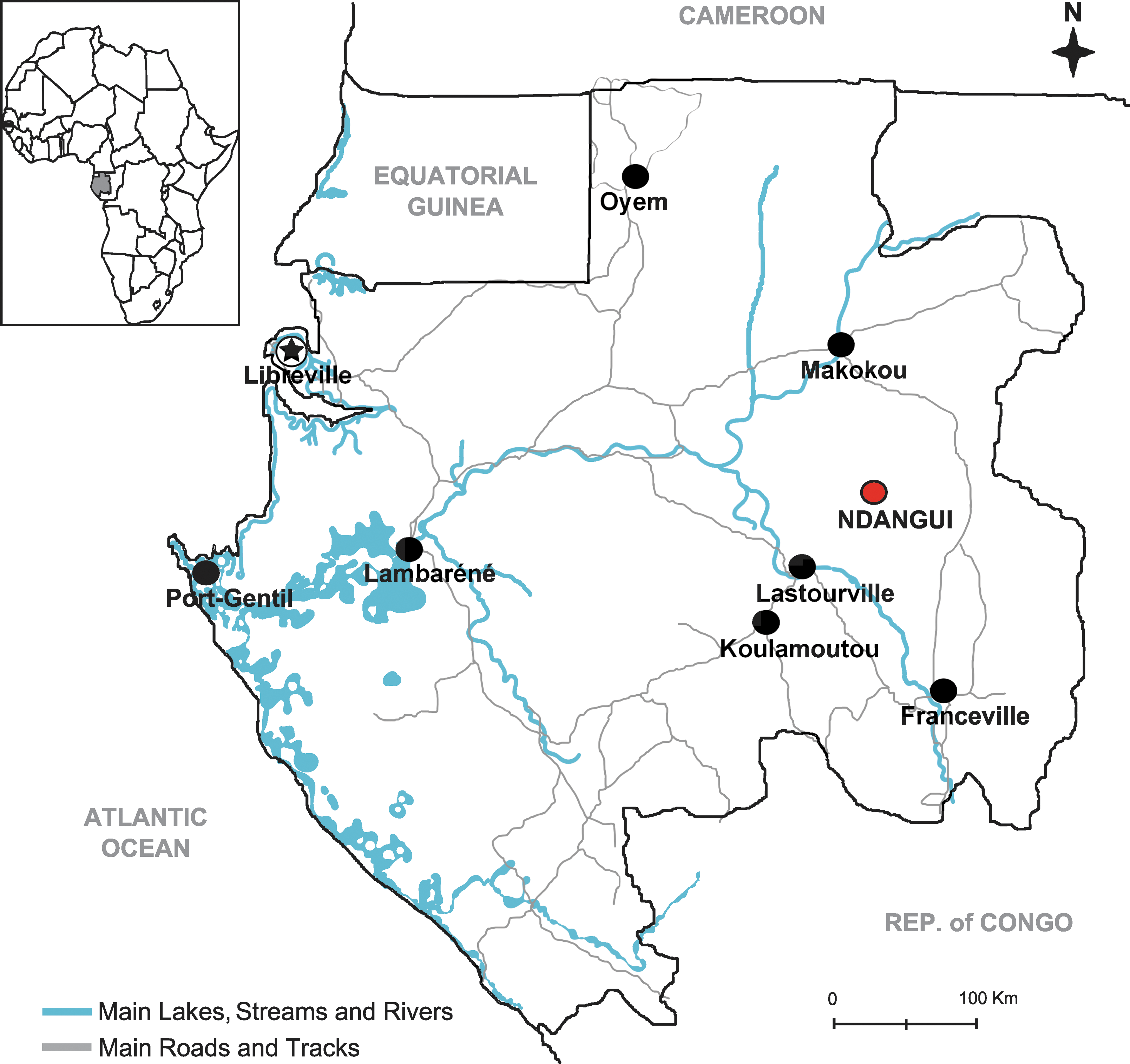
Map of Gabon, showing the location of Ndangui village.
The medical survey included a first active phase to identify patients with febrile arthralgic syndromes in order to identify the causative virus. Persons who presented with compatible symptoms (fever, arthralgia, and/or rash) during the investigation were examined by our team's doctors, and were sampled with their oral informed consent, as recorded by Ministry of Health (MoH) and CIRMF teams. The patients then received symptomatic treatment and care at home. One blood sample per suspected case was collected by arm venipuncture in EDTA tubes and kept at 4°C until their return to the CIRMF laboratory. At CIRMF, plasma samples were tested for several arbovirus RNA genomes, including CHIKV, Dengue, Yellow, West Nile, Zika Rift Valley Fever, and O'nyong nyong virus, using specific TaqMan qRT-PCR assays (Leroy et al. 2009). A total of 24 blood samples from febrile and arthralgic patients were collected during a 4-day period. Specific CHIKV TaqMan qRT-PCR (De Lamballerie et al. 2008) was positive in 12 samples, while all assays for other viruses were negative.
In order to assess the extent and duration of this CHIKV outbreak in Ndangui, we conducted epidemiological investigations during the same period, based on household interviews. A probable case of CHIKV was defined as an individual who declared having suffered fever and multiple arthralgias for at least 4 days within the previous month. Interviews were conducted in 90 of 137 households, representing 453 of the 640 Ndangui inhabitants. Seventy percent of the interviewees (n=325) declared having experienced a syndrome compatible with CHIKV infection, indicating a massive CHIKV outbreak in Ndangui. Moreover, such a percentage indicated that our intervention probably took place at or near the end of the epidemic, and also suggested that the major period of transmission occurred over 4–5 weeks. The high attack rate and explosive nature of the outbreak suggested that the population of Ndangui was largely naïve to CHIKV.
In order to identify a potential vector species involved in this outbreak, mosquitoes were collected outdoors during daytime after landing on volunteers vaccinated against yellow fever and taking malaria prophylaxis. Informed consent was obtained from every volunteer prior to their inclusion in the study, and institutional clearance was granted by the Health Ministry of Gabon. Mosquito collections were carried out by 5 volunteers during 2 days at the rate of two sessions per day (8:00–10:15
n Sampled, number of female mosquitoes sampled; n Pools, number of mosquito pools per species; n and %, number and percentage of CHIKV-positive pools per species; MLE, maximum likelihood estimate of mosquito infection rates, using the MLE-IR program (Gu et al. 2003).
Overall, these findings suggest that CHIKV massively infected the population living in the isolated villages of Ndangui. They also highlight the spread of A. albopictus in Gabon, even in isolated villages located in the deep rainforest. Most Ndangui villagers are gold miners who travel frequently between Ndangui and Libreville, always via Lastourville, a town located on the only rail line and the main road through Gabon. Thus, CHIKV and its vector were probably introduced, directly or indirectly, between 2007 and 2010, following the 2007 Libreville outbreak. The main potential human consequence of the growing geographic range of A. albopictus and its ability to colonize new ecosystems in Gabon, is the spread of epidemic pathogens, as exemplified here by Chikungunya virus. As A. albopictus also feeds on other animals (Gubler, 2003), there is a clear risk of human emergence of zoonotic viruses circulating in forest wildlife, and monitoring programs in central Africa need to be encouraged.
Footnotes
Acknowledgments
CIRMF is supported by the Government of Gabon, Total-Fina-Elf Gabon, and Ministère de la Coopération Française. This work was also funded by Institut de Recherche pour le Développement.
Author Disclosure Statement
No competing financial interests exist.