
Abstract
Psychiatrists have long been charged with access and coordination of care for transgender persons. This is now challenged by the World Health Organization's removal of diagnoses of mental illness related to gender identity in the 11th revision of the International Classification of Diseases. Using French field experimentations based on informal and primary care and free and informed consent, we discuss key challenges for a new organization of mental health care respectful of human rights. Developing informal and primary care as well as peer support has emerged as promising. Mental health expertise should be transferred from tertiary to secondary care.
Introduction
Diagnoses associated with transgender persons have been officially removed from the chapter on mental and behavioral disorders after the adoption of the 11th revision of the International Classification of Diseases (ICD-11) by the World Health Assembly on May 25, 2019. This change represents the culmination of decades of activism1–4 and follows several political human rights stances.2,5–7 However, the World Health Organization (WHO) has decided to introduce two new diagnoses, devoid of mental health components, under the name of “gender incongruence” in a new chapter dedicated to sexual health.8,9
Although these changes are often presented as a “depsychopathologization” of transgender persons,3,4,8,10,11 two distinct mechanisms are at work. First, removing the initial diagnoses of mental disorders, and second, adding new diagnoses in the new chapter dedicated to sexual health. The removal of mental disorder diagnoses was motivated by several field studies carried out in collaboration with the WHO, notably in Mexico, 8 South Africa, 12 France, 11 and Lebanon. 13 They supported the decision by highlighting that the mental health component leading to distress or functional limitation was not linked to identity but experiences of discrimination,8,10–15 and violence.8,10,11,13,14
Although the decision is still debated,4,16 the addition of new diagnoses in the ICD is intended to support some transgender persons who use the health care system to medically transition.8,9 As a result, medical transition is no longer regarded as a mental health treatment. WHO's decision allows for a simpler understanding of transgender persons' medical needs and removes the justification for hyperspecialized tertiary care. However, this creates an incongruence between ICD-11, and the DSM-V or WPATH (under revision) 17 approaches of transition as a way to reduce “gender dysphoria,” itself a polysemic concept. 18
These shifts in concepts lead to substantial changes in the organization of care. In the old model, care was accessed through specialized tertiary care mental health services that acted as gatekeepers and coordinators of physical, mental, and social pathways. 14 The changes made by WHO shifted the medical authority for regulating access to hormonal treatment, surgery, or other care11,14 to primary health care providers, who often already assumed this coordinating role. 14 The changes in ICD-11 shift the position of mental health professionals from diagnosis and coordination of care11,19 toward a support role and a nonmandatory involvement in a now primary care pathway. 19 The person may access transition-specific health care after a self-diagnosis assisted by a primary care provider11,19 who will coordinate access to the health care system on the basis of free and informed consent.11,19
However, many studies showed the mental health of transgender persons is poor,7,8,10–12,14,20,21 partly as a result of discrimination,8,11–13 violence,8,11,13 and minority stress.11,14,22,23 The WHO also frames mental distress as a result of lack of access to information or proper care. 7 Independently of medical transition-related care (and, therefore, a diagnosis of “gender incongruence”), the transgender population as a whole is at risk of mental health problems and, therefore, justifies privileged access to mental health care. 7
Moreover, maintaining the old model to access mental health care would remain discriminatory and encourage microaggressions. 15 To prevent low or nonexistent access to mental health care, we need new effective organizations that respect people's rights.2,4,7,9,11
Experimentations in Lille
As part of ICD-11 field studies, the Lille-based research team was set up and brought together researchers, transgender service users, primary care professionals, and secondary mental health care professionals. This initiative was based on the meeting of two field experiments: the Collectif Santé Trans (CST, Trans Health Collective) and the EPSM Lille-métropole, a WHO collaborating center (WHOCC).
The CST is a collective of primary care professionals, organizations, and transgender persons based around the Maison Dispersée de Santé (MDS, Dispersed Health Center). The MDS is a primary care center providing support to transgender persons in their transition on the basis of free and informed consent, and without resorting to a psychiatric diagnosis. Since 2011, this initiative is based on a risk-reduction perspective derived from the experience of transgender persons who were self-medicating 7 after rejection by the tertiary care psychiatric system. 11 A collective was, therefore, set up to reflect on the organization of this new care system with a central focus on experiential knowledge. 3
The mental health service of the municipalities of Mons-en-Baroeul, Hellemmes, Lezennes, Ronchin, Faches-Thumesnil, and Lesquin (59G21) at EPSM Lille-métropole is an experimental community mental health care organization. 24 Its evolution toward full community integration motivated the implementation of a WHOCC, 25 working on developing and disseminating models of community-based mental health care. As part of ICD-11, it was tasked with involving stakeholders in the review of their diagnoses. Collaboration with the MDS was established and it was possible to carry out one of the WHO field studies in this depsychiatricized context, in collaboration with transgender service users.3,11
This bottom-up attitude toward research mirrors the clinical one based on consent. This includes involving transgender persons on the basis of human rights and principles laid down by authorities such as the Council of Europe.3,5 Recently, the Comité d'Usagers Trans (CUT, Trans Users Committee) was developed with the regional health agency to enable transgender persons to take part in the organization of health care on a larger scale. Figure 1 shows the model of community mental health developed by the WHO and Wonca, 26 and highlights the place of each stakeholder.
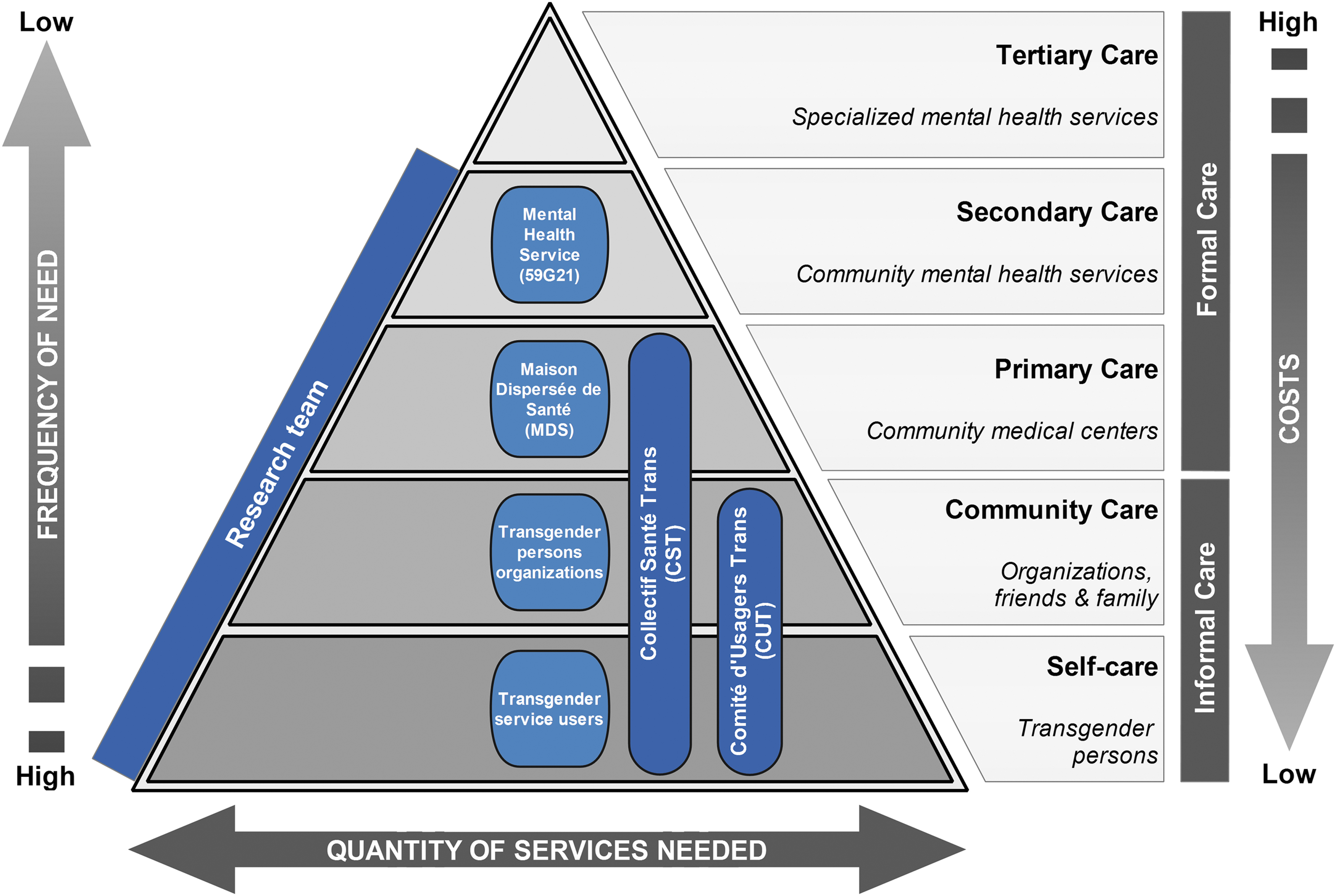
Place of each research stakeholder in the community mental health care. The gray-scale diagram illustrates the community mental health model developed by the WHO and Wonca. The superimposed color elements are the Lille stakeholders participating in the experiments. Each stakeholder is located at a distinct level of the care pyramid. In addition, there are two cross-cutting groups linking multiple levels and excluding secondary mental health care. This layout illustrates the bottom-up development of Lille's community health services. The research team connects all levels of care from self-care to secondary mental health care.
Goals for Field Practice
Surprisingly, no consensus exists on implementing human rights for transgender persons,2,7,16 even though the Yogyakarta Principles 6 represent increasingly shared standards.2,4,16 In the field of health, the WHO defines four criteria for information—availability, accessibility, acceptability, and quality—and three criteria for accessing services—respect, dignity, and nondiscrimination. 7
The organization through tertiary mental health care contradicts a significant number of these criteria, although it varies between regions. 7 More importantly, after the removal of mental health diagnoses in ICD-11, it seems difficult to justify why mental health entry or coordination would not be discriminatory. Such an approach should instead be based on the mainstream mental health system, with increased accessibility for as long as the undue risk associated with the social context remains.8,11–13
Increasing accessibility requires removing existing barriers and implementing facilitating actions. Field reports identify numerous barriers such as cost of medical procedures, stigmatization, bad personal and peer experiences, non-LGBTQI friendly services, or ineffective services, often due to a lack of training.20,21 Instead, training of professionals, adjustments to care services, employment of peer workers, employment of LGBTQI friendly people, and increased resources are seen as facilitating access to mental health care.20,21
These field observations join global issues of effective inclusion of stakeholders in organizing health systems to embrace their experiential knowledge and address issues of discrimination and intersectionality. Although these measures are known, few examples of implementation are described. 7
Future Developments in Lille
In France, the health care system is socialized, and formal care, both private and public, is fully reimbursed for medical transitions, even if difficulties in asserting these rights may arise, as is regularly the case for surgeries. A particular feature of the system is that public outpatient mental health care, although very heterogeneous throughout the territory, is free of charge. Thus, the prohibitive cost of care, regularly cited as a major barrier, is not taken into account in our analysis.
All experiments in Lille offer the advantage of being bottom-up initiatives starting from field operators, especially transgender persons. It was emphasized that their low representation in research contributes to poor applicability and a growing gap between research and practice.3,5 The research team initially set up for the ICD-11 field study intends to continue documenting these initiatives based on free and informed consent, which remain rare at the international level. The possibility of introducing a feedback loop through action research remains possible. Table 1 lists current dynamics for each stakeholder.
Research Stakeholders in Lille, France
Their synthesis and an analysis of field components are presented in Figure 2. The current Lille system is still far from the ideal community model. However, stakeholder dynamics are moving in its direction with four main areas of development:
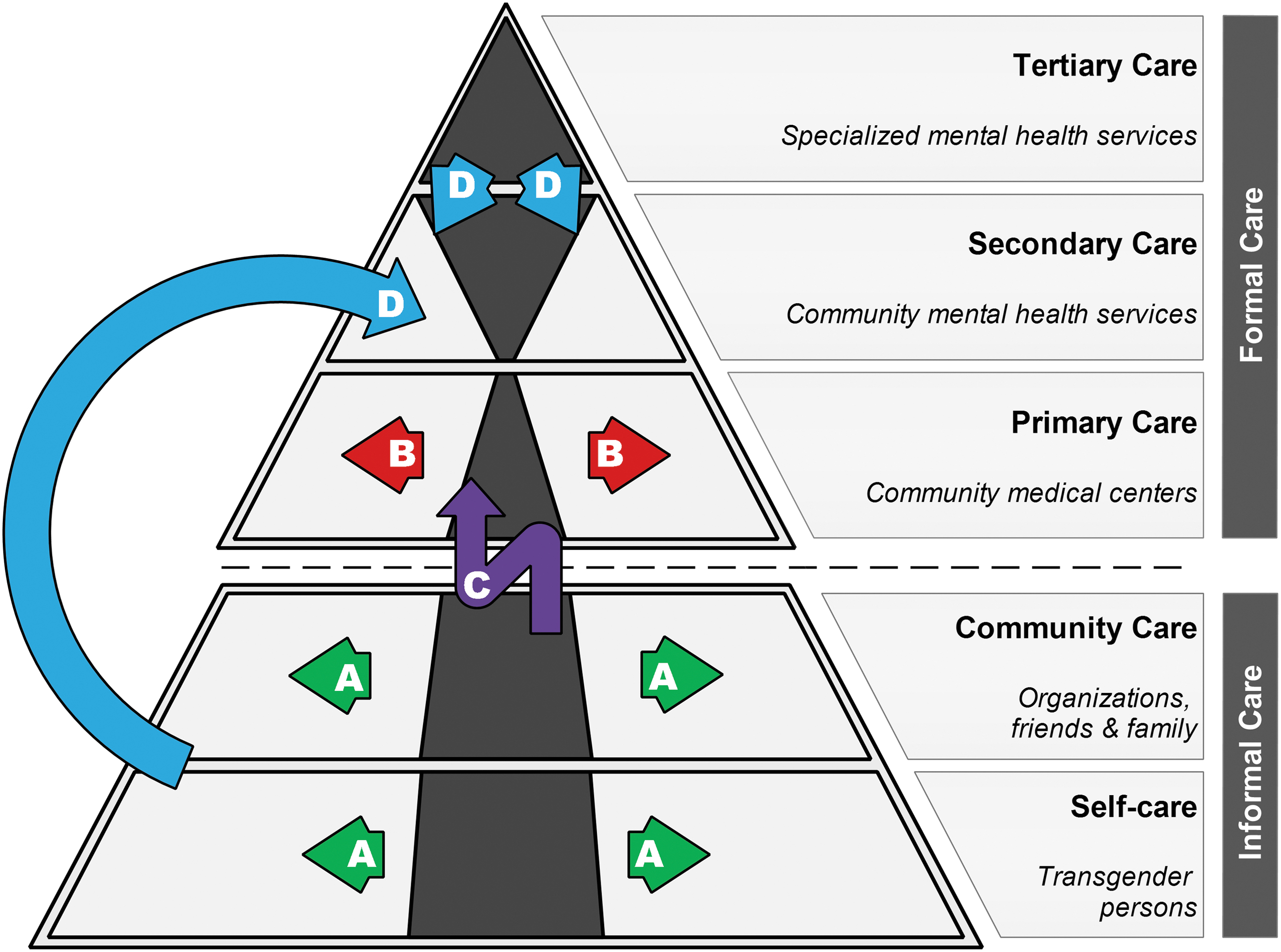
Axes for modifying the current organization of mental health care compared with theory. The gray-scale diagram shows an estimated proportion of real care (dark) over the theoretical proportion (light), based on the model developed by the WHO and Wonca. The superimposed color elements reflect the four trends (A–D) identified among ongoing actions by field actors. They aim at filling the gaps in the real care system and bring it closer to the theoretical care system. Concrete actions in these four trends are developed in the core text.
(A) Development of informal care. This axis is based on developing support networks through organizations, involving users, and disseminating information to promote self-care. Emphasis on organizations to the detriment of families seems linked to a cultural rejection phenomenon.8,11–13
(B) Spread of transgender care based on free and informed consent within primary care medicine. Recently, the MDS initiated the creation and implementation of a local network already including two additional medical centers. Fundamental ideas, beyond improving access to care, are avoiding the development of a new parallel specialized system, and spreading developed knowledge in the form of coconstruction.
(C) Linking informal care and primary care. To this end, the CST is working to develop professional training for transgender peer workers to reflect on care pathways in complementarity with primary care professionals.
(D) Transfer of mental health competence to secondary care. This area also includes knowledge transfer from tertiary care, but also informal care where it was developed for people excluded from mainstream care, often gender nonconforming or not meeting psychiatric medical criteria.3,11 However, considering particularities of transgender persons in secondary mental health care remains marginal worldwide. 7
Conclusion
ICD-11 appears an appropriate justification for changing care organization in favor of transgender persons' rights. The community mental health model and primary care initiatives show that such changes are possible. Future efforts should focus on developing tools to assess organizational transformations and their impact on the health and social inclusion of transgender persons. Defining consensual indicators for evaluation would be a first step to global transformation of health care.
Footnotes
Acknowledgments
The authors thank field actors, both service users and professionals for their ongoing work toward a fairer world. This includes members of the Comité d'Usagers Trans; Camille Cau and other members of the Association Nationale Transgenre; Bérangère Donnet, Anna Menissez, Nassir Messaadi, Bertrand Riff, and members of the Collectif Santé Trans and professionals from the MDS; Laurent Defromont and professionals from the mental health service of the municipalities of Mons-en-Barœul, Hellemmes, Lezennes, Ronchin, Faches-Thumesnil, and Lesquin (59G21), especially those working to reduce discriminations in mental health care (Saliha Ahmed-Ali, Fabien Diakite, Émeline Galet, Angélique Lecomte, Florian Owczarczak, Lydia Pereira, Calogero Piazza, Marianne Ramonet, and Samantha Robin); and members of the research team from the WHO Collaborative Centre for research and training in mental health (Françoise Askevis-Leherpeux, Patrice Desmons, and Jean-Luc Roelandt).
The authors also thank Sabine Bayen for reviewing the final draft.
Authors' Contributions
Design of the study was taken care of B. A. and de la C. M.; initial draft was prepared by B.A.; and article was reviewed by de la C.M., D.C., and M.M. -J.
All authors have approved the final version.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no specific funding for this work.