
Abstract
Purpose:
We examined health care experiences of transmasculine young adults to clarify factors contributing to mistrust in the health care system and identify tangible and modifiable means to address health disparities through improved patient–provider interactions. Thematic analysis highlights patterns within historical relationships between medical models and transmasculine embodiment, and provides guidance for health care clinicians, researchers, and policy makers to deliver competent services for transgender and gender diverse (TGD) individuals.
Methods:
The study team used qualitative methodology guided by interpretive phenomenological analysis. Semistructured interviews with 12 participants who self-identified as transmasculine were conducted, transcribed, and coded thematically.
Results:
Participants were a community sample of 12 young adults 18–35 years of age (M=23, standard deviation=3.74), who self-identified as transmasculine. Three participants identified as a racial/ethnic minority. Participants were highly educated, with most completing at least some college. The superordinate thematic domain Perspectives on Health Care emerged, under which three subthemes were nested: (1) an essentialist, binary medical model is inaccurate and oppressive, (2) consequences of medicalizing gender (i.e., gender as a diagnosis), and (3) recommendations to improve health care.
Conclusions:
Qualitative analysis revealed specific ways in which the relationship between transmasculine individuals and current health care systems are fraught with difficulties, including the impact of stigma, gatekeeping, and inaccuracies, in current diagnostic criteria. Participants shared lived experiences and offered innovative ideas to improve health care delivery, such as challenging socialized biases, increased education, and immersion in TGD communities to advocate for change in research, practice, and policy.
Introduction
Transgender people are estimated to comprise 1.4 million individuals within the U.S. population. 1 This is likely an underestimate, considering the stigma associated with reporting transgender and gender diverse (TGD) identities. Moreover, inadequate tracking omits TGD identity designation in research and practice. This stigma and omission may be based in essentialist assumptions, which hold gender identities and expressions as binary, fixed, and entirely derived from biological sex, rather than a diverse or socially constructed phenomenon. That is, the outward appearance of genitalia at birth determines one's sex, gender identity, gender expression, and sexuality.2–4 Although the essentialist paradigm can be useful for scientific classification, the application is restrictive when applied to the complexity of sex, gender identity, and expression. Consequently, essentialism disrupts TGD individuals' relationships within the health care system. 3
Data gathered from the 2010 National Transgender Discrimination Survey (NTDS) 5 revealed that TGD clients reported negative interactions with providers at staggering rates. Reports included lack of provider knowledge (50%), harassment (28%), refusal of care (19%), and violence in medical settings (2%). 5 These reports highlighted a substantial gap between best practice and current practice, and suggested that the health care system requires substantial training, transformation, and engagement with the increasing body of empirical literature supporting TGD health to provide competent care for this growing population.
These negative encounters in health care may be underpinned and exacerbated by essentialist assumptions.6–8 Furthermore, they exemplify what minority stress theory categorizes as “distal stressors,” 9 and may have physical ramifications. For example, when encountered, distal stressors can initiate a repeated triggering of autonomic nervous system and hypothalamic-pituitary-adrenal axis responses, 10 with cumulative effects leading to increased risk for chronic health conditions and accelerated aging (i.e., weathering). 11 Related to this, research suggests that TGD individuals experience chronic health conditions (e.g., hypertension, diabetes, obesity, stroke, depression, and post-traumatic stress disorder) at higher rates than cisgender peers.5,12–14
Effects also play out on a practical level, with 33% of TGD respondents in the NTDS postponing preventive care and 28% avoiding health care altogether for fear of discrimination and mistreatment based on their gender identity. 5 Another study found 40% of TGD elders feared accessing health care services due to discrimination and internalized stigma (both modifiable factors that intensify chronic stress). 13 Undoubtedly, health care providers are instrumental to reducing disparities and facilitating favorable health outcomes for TGD people.
Recent diagnostic changes reflect health care's shifting views of TGD identities. Particularly, TGD identities are no longer viewed as a pathological mental illness. Rather, in 2012, the World Professional Association for Transgender Health (WPATH) recommended that clinicians address psychological distress associated with stigma and discrimination when necessary, and ensure access to care based on an informed consent. 15 In addition, in its 2019 revision to the ICD-11, the World Health Organization (WHO) re-classified “gender identity disorder” as “gender incongruence” and moved it from “Mental and behavioral disorders” to a new chapter entitled “Conditions related to sexual health.”16,17 Despite acknowledged imperfections, the WHO posited this revision is a step toward de-pathologizing TGD identities, while allowing access to affirmative care.17–19
This project examined health care experiences of transmasculine young adults to clarify factors contributing to minority stress and resilience, and identify ways to improve patient–provider interactions. Researchers extracted data from a larger, overarching qualitative study that highlighted how transmasculine young adults defined the term “transition,” and made meaning around concepts like gender, intersectionality, and the process of transmasculine identity development. Here, themes regarding perspectives on health care are presented. Rather than proceeding with a preconceived hypothesis, we phenomenologically allowed themes to emerge.
Method
A qualitative approach was used for the overarching study, guided by interpretive phenomenological analysis (IPA). 20 IPA examines how people make meaning of significant life experiences on individual and group levels, and is based in three philosophical tenets: (1) phenomenology, (2) hermeneutics, and (3) idiography.20,21 All research activities were approved by the University of Wisconsin-Milwaukee Institutional Review Board.
Recruitment efforts included personal visits to Midwestern LGBTQ community centers, and outreach to various online social media groups. Overall, 15 people responded to postings, and 12 met inclusion criteria (e.g., 18–35 years of age, self-identifying as transmasculine). Data used in this study were derived from the same 12 participants (Table 1). Reasons for exclusion included not self-identifying as transmasculine, not meeting the age requirement, and interest in participation after data collection concluded. Participants were interviewed in safe settings, including library study rooms, university spaces, and secured online video conferences, such as Zoom.
Demographics
Data collection
Data were collected with semistructured, one-on-one interviews between the lead researcher and participants. We selected this approach for flexibility that allowed unexpected, meaningful dialogue to emerge. 22 Researchers developed an open-ended interview guide to facilitate explorative free-flowing narratives, while remaining focused on topics of inquiry. This format allowed for (1) seamless movement from one topic to another, as unexpected conversational shifts are noteworthy in IPA analysis, and (2) participants as experts, leading researchers to thematic illustrations of “the thing itself.” 20 Topics broadly explored included identity development, intersectionality, meaning making, and experiences in health care systems.
After obtaining informed consent, the interview process focused on building rapport, while gathering demographic data. Interviews were audio recorded and transcribed verbatim for analysis. After transcription, participants were asked to review their transcript and encouraged to provide feedback. Two participants responded with edits (e.g., elaborations and typo corrections). All approved their transcriptions. Participants received $20 cash remuneration.
Research team
Two advanced doctoral level counseling psychology students were hand-picked to assist with data analysis, as they had extensive multicultural training, which included issues relevant to TGD identities. In the spirit of reflexivity and transparency, the team discussed intersectionality of their own identities, and how they may shape the analytical lens, which included (but were not limited to) the following: transmasculine, cisgender, female, white, 30–40 years of age, and queer. All team members were experienced qualitative researchers. The lead researcher provided mentorship specific to the IPA approach, emphasizing a safe and open climate, wherein researchers were encouraged to express ideas and challenge one another on potential blind spots. Researchers unanimously agreed that reflexivity, respect, active engagement in difficult dialogues, and bracketing preconceived ideas in analysis were critical to the research process.
Data analysis
As per IPA principles, analysis was neither fixed nor rigid, but comprised a common procedures set and commitment to illustrating group-level themes with idiographic, individual experiences. 20 Because 12 participants was large for an IPA sample size, we developed an analysis plan adapted from Smith et al., 20 which adhered to core IPA principles (Fig. 1). The team repeated the steps until saturation was reached.
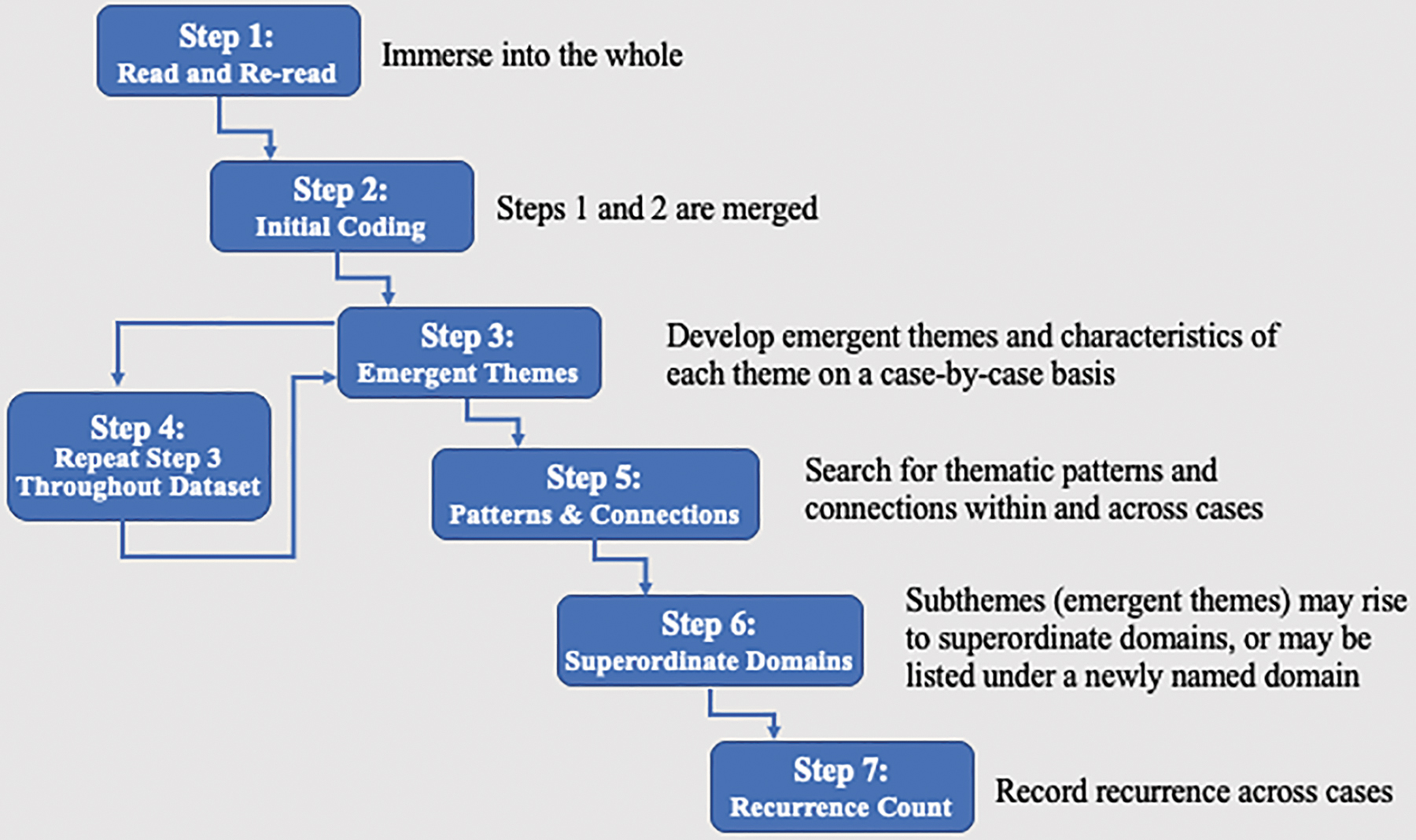
Steps to interpretive phenomenological analysis, adapted from Smith et al. 20 This figure illustrates the recommended steps researchers followed in the analysis of qualitative data collected for this study.
Our large sample allowed tabulation of cross-case thematic recurrence rates. Measuring recurrence supports the validity of findings, as it quantifies reports of a particular phenomenon across participants. 20 For this study, designation of superordinate domain was set at a stringent 100%, meaning that subthemes must have appeared in all 12 narratives to meet criterion. The recurrent designation for subthemes was set at a rate of >50%, that is, for a subtheme to become recurrent, it must have appeared in at least 7 of 12 transcripts (Table 2).
Thematic Recurrence
Data trustworthiness
To broaden trustworthiness (i.e., validity), 23 individual quotes substantiated themes at the group level. Participant feedback was encouraged to ensure accuracy of data, interpretations, and representativeness of experiences. Researchers continually balanced reflexivity and subjectivity throughout the analytic process. Frequent research meetings allowed expression of multiple viewpoints, expectations, and preexisting notions. Differing narratives on the same topic were examined, with emergent subthemes and superordinate domains calibrated accordingly. Transparency guided the analytic process, and researchers followed steps to demonstrate credibility and applicability 23 (Fig. 2).
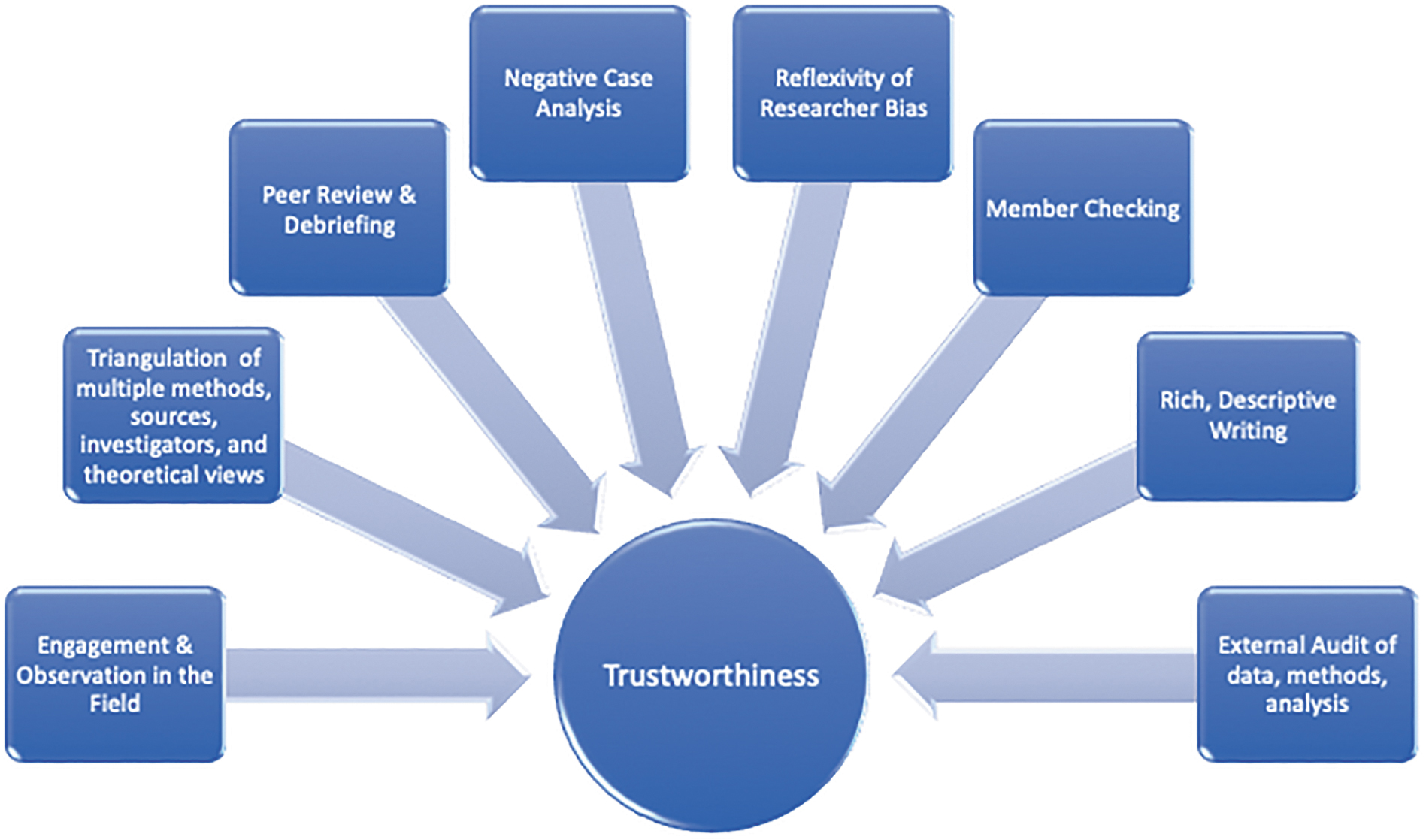
Trustworthiness strategies, adapted from Creswell. 23 This figure illustrates steps and procedures researchers followed to ensure trustworthiness (i.e., validity) in data collection, analyses, and interpretation.
Results
Demographic characteristics
A community sample of 12 young adults self-identifying as transmasculine and between 18–35 years of age (M=23, standard deviation=3.74) participated in the study (Table 1). Three participants identified as a racial ethnic minority (mixed race/ethnicity, Brown/Latinx, or Black/African American). Participants were highly educated, with most completing at least some college.
Thematic outcomes
From the full analysis, Perspectives on Health Care arose as a superordinate domain and is the focus of this article. Three subthemes comprise this domain: (1) an essentialist, binary medical model is inaccurate and oppressive, (2) consequences of medicalizing gender (i.e., gender as a diagnosis), and 3 (3) recommendations to improve health care.
Subtheme 1: An essentialist, binary medical model is inaccurate and oppressive
Participants described experiences with a health care system that largely reifies an essentialist, binary sex/gender framework, and found case conceptualization through an essentialist framework to be inaccurate and contrary to affirmative health care. For example, participants found binary categorizations of sex and gender erroneously simplistic, leading to the common, fundamental mistake of muddling constructs of sex and gender. These limitations resulted in negative experiences with providers, often leaving participants in the position of educating providers, vulnerable, invalidated, and cautious. In addition, when seeking physical transition-related care (e.g., hormones), participants often received messages that they were “not trans enough” and would be denied care if they did not meet cisgender expectations of men/masculinity. Moreover, participants viewed transition as a lifelong process encompassing many psychosocial facets, rather than a “one and done” treatment. Participants illustrated the impact of systemic oppression (e.g., binary only options on clinical forms), representing a large misalignment between the current health care system and TGD well-being.(Table 3).
Perspectives on Health Care
TGD, transgender and gender diverse.
Subtheme 2: Consequences of medicalizing gender (i.e., gender as a diagnosis)
Participants discussed the diagnosis “gender dysphoria,” and resultant stigma around TGD identities. Externalizing stigma was taxing and ongoing. Participants did not view all transmasculine experiences as dysphoric, yet they felt pressure to placate providers by emphasizing dysphoria and/or identifying with cisgender binary standards to access care. Contrary to revised standards of care, 15 participants reported being “forced” to accept a diagnosis, with practitioners wielding “gatekeeping” power to withhold care. Notably, while the applied effects of gatekeeping emerged in this subtheme, thematic roots of gatekeeping as inextricably tied to essentialist assumptions are captured in the previous subtheme (Table 4).
Perspectives on Health Care
Subtheme 3: Recommendations to improve health care
Participants offered practical suggestions for providers. Foremost, participants wanted to trust, and urged providers to listen and challenge personal biases. Providers would garner trust by informing themselves rather than placing that onus on the individual in their care. One suggestion to facilitate self-guided learning included active immersion in TGD communities, and conducting affirmative research in multiple fields of study (e.g., endocrinology, public health, mental health, neuropsychology, and primary care). Interestingly, participants commented that binary constructs also harm cisgender people, restricting variation in identity and expression, and suggested approaching topics of transmasculinity and TGD health with the same respect, curiosity, and fervor as any scientific inquiry. Thus, continual self-reflection, developing TGD-centric frameworks, and challenging socialized biases were described as essential to competent research and practice.
Inclusive clinical forms and environmental cues were important, including diverse décor, competent front-line staff, and witnessing an array of practitioner identities reflecting those of participants. Language was named as a significant catalyst for changing or maintaining the status quo. Participants offered suggestions to expand language, thereby social constructions. For example, abandon binary forced-choice options (e.g., boxes for male/female), add space for pronouns in use, and/or include write-in options for identities in clinical and research demographics (Tables 5 and 6).
Perspectives on Health Care
Recommendations for Health Care Clinicians, Researchers, Staff, and Systems
Participants highly valued positive patient–provider interactions, which included the following: active listening, demonstrating competencies in TGD health, using correct name and pronouns, and welcoming spaces. Informed providers understood limitations and advocated for change in TGD health care. They were knowledgeable about informed consent versus gatekeeping models, and did not pathologize identity. They listened, rather than pushing a specific trajectory or treatment plan, and did not assume TGD identity as the core of presenting concerns. In fact, informed providers understood transmasculine identity as an individualized process and a source of immense resilience and strength.
Discussion
Participants provided insights regarding transmasculine experiences in health care systems, revealed factors causing mistrust, and recommended measures to improve interactions. Subthemes included the following: (1) an essentialist, binary medical model is inaccurate and oppressive and (2) consequences of medicalizing gender (i.e., gender as a diagnosis). A third subtheme highlighted steps to improve TGD health care.
Medical model in context
Understanding how sex and gender are governed through societal forces requires examining the historical relationship between medicine and TGD embodiment, including advancements in endocrinology, surgical interventions, and unethical experimentation. Extensive interdisciplinary review documents this history.3,24–30 Stryker explained how medicine's social authority and influence on TGD health have grown, potentially surpassing that of religion. 29 Stryker 29 acknowledged the positive impact of modern medicine in everyday life, but asserted medicine maintains and regulates normative standards, posing substantial obstacles for TGD individuals.
Likewise, Johnson explained, “Transgender identity and experience has been formally claimed and defined by medical authority since the introduction of a psychiatric diagnosis for gender variance in DSM-III.” 31 Indeed, diagnostic classification in the DSM was revised from Gender Identity Disorder (DSM-III, 1980) to Gender Dysphoria (DSM-5, 2013).32,33 Revisions represented a shift in ideology focused on treating psychological distress rather than labeling TGD identity a disorder. However, the individual and their embodiment remain the crux of distress. 31 Notably, our data indicated that gender-related psychological distress stemmed predominantly from external sources of transphobia and cissexism. Finally, the current diagnosis acknowledges not all transgender individuals experience dysphoria, but presumes medical intervention is the next step for those who do, 31 and diagnostic language reifies an essentialist binary (e.g., diagnostic criterion: “A strong desire to be of the other gender”). 33
Overall, standards of care have progressed, as evidenced by those set forth by WPATH. 15 However, gatekeeping persists. For example, as noted, 31 WPATH 15 included a revision stipulating that individuals 18 years of age and older should be granted access to care based on informed consent. However, providers are not mandated to uphold these practices, and maintain great power in governing TGD identities. In addition, despite revisions to the DSM-533 and ICD-11,16,17 reframing systemic policies, cultural norms, and health professionals' perspectives will be a process that requires insight and time.
Tangible inlets for reducing health disparities
Participants' negative experiences could be understood through the Minority Stress Model, which Meyer 9 characterized as (1) unique and additive, (2) chronic, and (3) socially devised/maintained. Marginalized people must continually adjust to additive and pervasive stressors not experienced by nonstigmatized individuals. Embedded in a sociocultural context, the stress is chronic and unrelenting, and may lead to negative biopsychosocial health outcomes. Finally, marginalization and resultant stress are perpetuated through socially derived institutions and systems (e.g., health care) outside of one's control, devised to maintain existing power hierarchies.
In addition, the Weathering Hypothesis 11 proposes that accumulated burden from confronting multiple, on-going psychosocial stressors manifests as accelerated aging. The related theories of minority stress and weathering have been independently tied to adverse health effects (e.g., allostatic load, diabetes, cardiovascular disease, depression, and post-traumatic stress disorder) in people with marginalized identities.34–43 Researchers are beginning to include TGD individuals in studies exploring the mental and physical health effects of minority stress and weathering.5,34,35,44
Our data illustrate how minority stressors and weathering ensue through patient–provider interactions, offering tangible inlets to reduce health disparities. For example, consistent with NTDS 5 findings, our participants described having to repeatedly educate providers steeped in ciscentric, binary views. They described this process as physically and emotionally taxing, exemplifying minority stress 9 and potentially invoking the weathering process. 11 Despite pleas for competent health care, essentialism in the medical system reflects an inherent bias toward caring for cisgender individuals, prompting TGD individuals to avoid health care rather than risk invalidating oppressive and unsafe interactions.
In addition, marginalization and subsequent minority stressors and weathering processes are perpetuated through medicalizing gender and gatekeeping practices (i.e., requirement of a pathological, stigmatizing diagnosis and multiple letters of support to access care).34,45 Ciscentric and essentialist reference points in the medical approach link interventions to diseases and disorders,24,28,31,46 perpetuate social expectations that cisgender identity is the normal and valid standard, and serve as bedrock for participants' fears around being perceived “not trans enough.” For example, Benjamin 47 was among the first physicians to offer hormonal and surgical options for trans-identified people. However, consistent with the medical zeitgeist, he labeled “true” trans people as those who desire medical intervention to “align” their physical bodies with their gender identity. 48
This message persists today, as our participants experienced repeated stressors and unrelenting pressure to align with cisgender conceptions of male/masculine to appease gatekeepers.45,49 For our transmasculine participants, “not trans enough” centered around expectations to conform to socially constructed standards of masculinity to be deemed valid. Moreover, participants reported a double standard in following prescribed cisgender trajectories. For example, feminine cisgender men may be targets for discrimination; however, their gender identity and sex are not questioned as is common with transmasculine people who demonstrate similar qualities. 50
Entwined with the Benjamin standards, 47 “not trans enough” is steeped in essentialism and perpetuated through authoritative frameworks, such as multiple iterations of the Diagnostic and Statistical Manual of Mental Disorders (DSM).32,33,51 Davis et al.8 characterized the Institute of Medicine's influence in creating and disseminating ideologies around sex, gender, and sexuality as such, “… they not only perpetuate but produce the notion that a healthy body is identifiably male or female, masculine or feminine, and heterosexual.”
This creates tension, as providers have the power to bestow sex and gender, as well as reify the status quo. In sum, the consequences of essentialism in medicine are fundamental to participants' negative experiences, resulting in minority stress, inaccurate diagnostic assessment and treatment, increased vulnerability, distrust, and avoidance of health care. Thus, it is imperative that practitioners and researchers examine socialized biases. In doing so, we have power to minimize deleterious effects of compounding distal minority stressors and weathering processes on TGD people, and maximize outcomes in TGD health.
More than half of participants described burdensome nuances of minority stress associated with viewing TGD identities as a pathology, and subsequent gatekeeping practices. To elaborate, letters from physicians and psychologists are often required to begin legal processes of amending identity documents (e.g., driver's license, and passport). Many U.S. states require a surgeon's letter to amend assigned sex on birth certificates45,49 In other words, some form of binary-based surgical intervention must be performed, regardless of individual preferences or socioeconomic access. Interestingly, the process of gatekeeping may inflate or misrepresent rates of TGD individuals seeking psychotherapy, their presenting concerns, and rates of gender dysphoria diagnoses. 49
In addition, some participants who desired medical intervention(s) sidestepped gatekeeping (i.e., adapting to minority stress) by finding clinics offering services based on informed consent. Participants understood this access as a privilege, closely tied to other facets of identity (e.g., socioeconomic status, race, and geographic location). While participants were not specifically asked about their level of access to health insurance coverage, disclosures were intertwined in many participant responses. Overall, participants demonstrated a high level of insight and awareness regarding privileges they benefitted from, including access to health insurance and/or any degree of gender-related service coverage. However, despite most participants having access to health care, most expressed added burdens, such as facing discrimination, while having to navigate a complicated system on their own, or repeatedly educating providers around gender identity and sex. For this reason, trust may be difficult to establish in a variety of settings, including educational settings that frequently rotate providers (e.g., hospital residents and interns).
Practitioners' assumptions and pathology-based framework contribute to an essentialist, gatekeeping model that imposes minority stressors detrimental to TGD health.28,52 However, consistent with the literature,24,28,31,46,53 our participants challenged pathological notions of TGD identity by reporting ways transmasculine identity serves as a source of pride, well-being, and resilience that can buffer the negative effects of minority stress and weathering. 35 Moreover, participants rejected the idea that one must be dysphoric to benefit from medical intervention. As one participant explained, one who is “euphoric” may also desire medical options. Participants challenged the “one and done” conceptualization of transitioning, explaining that transition is a multifaceted psychosocial developmental process that may or may not include any number of medical interventions.
In response, TGD health experts consistently advocate for nonpathological frameworks to conceptualize gender identity development, evidence-based care, and access to affirmative care, including informed consent.15,28,52 Revisions to the ICD-1116,17 will inevitably bring changes on an international scope, but the directions of change have yet to be seen, and shifting the landscape to a non-pathological framework will take time.
In the meantime, providers can take practical steps to reduce the significant and cumulative burden of minority stress, as reported by participants in this study (Tables 5 and 6). Providers can acknowledge and challenge socialized biases, educate themselves, immerse themselves, and work with TGD communities to advocate for change in research, practice, and policy. Providers can be transparent with patients, acknowledging strengths and limitations of current systems. Providers can be knowledgeable in TGD health research, pass this information along to patients, and collaboratively support them as they make informed decisions around their health care.
Strengths and limitations
Strengths of IPA methodology included the ability to develop research questions relevant to transmasculine health, and recruit participants accordingly. The idiographic focus enabled detailed themes and patterns to emerge across participants. 22 However, given this research was based on the experiences of 12 self-identified transmasculine young adults 18–35 years of age from urban and rural areas in the Midwest, most with access to health care and some degree of college education, caution must be used when generalizing insights. Twelve participants generated an extraordinarily large data set for IPA, and the richness of idiographic analysis may have been compromised in favor of thematic group interconnectedness. However, the benefits of IPA outweighed the limitations, and future research will enable wider generalizations over time. 22
Conclusions
This research illustrated and honored the lived experiences of transmasculine individuals. In this study, we focused on one superordinate theme, Perspectives on Health Care, with three subthemes: (1) An essentialist, binary medical model is inaccurate and oppressive,(2) consequences of medicalizing gender (i.e., gender as a diagnosis), and(3) recommendations to improve health care.
To access health care, transmasculine individuals need not invoke a narrative that is linear, binary, and reflective of cisgender standards. In addition, practitioners wield great power to address miseducation, such as transition being synonymous with a one-and-done medical cure for a pathological condition. Moreover, validating TGD identities decreases stigma, inevitably influencing positive mental and physical health outcomes. Participants' gender identity can be a substantial source of strength, just as it can for anyone. Thus, it is imperative practitioners examine their own power and biases, and broaden conceptualizations in research and clinical practice. Neglecting to do so denies TGD people the dignity and care they deserve, and perpetuates health disparities. Active engagement will positively impact people of all genders, and help build frameworks that promote the well-being of TGD people. This is within our ethical code in research and practice, as we must first do no harm.
Footnotes
Acknowledgments
We thank Outreach LGBT Community Center and Madison Area Transgender Association of Madison, WI for their collaboration in this project. We also thank Shannon Chavez-Korell, PhD, and Marty Sapp, PhD, for their contributions and guidance, and Sarah Morgan, PhD for insight regarding the history of medicine and TGD health. Finally, we are incredibly grateful for the courageous and resilient participants who offered their time and trust to advance research benefitting TGD health today, and in generations to come. This is GRECC article number 002-2020.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
We also appreciate the mentorship of Dr. J.D.F., who was supported by grant # K01AG056669.