
Abstract
Abstract
Introduction:
This systematic review assessed the impact of race/ethnicity, education, and income on transgender individual's lifetime experience of suicidal thoughts and behaviors (SITB) in gray and published literature (1997–2017).
Methods:
Sixty four research projects (108 articles) were identified in WorldCat, PubMed, and Google Scholar. Articles were included if they were published in Canada or the United States, included original quantifiable data on transgender SITBs, and had ≥5 participants, at least 51% of whom were ≥18 years.
Results:
Across all projects suicide ideation averaged 46.55% and attempts averaged 27.19%. The majority of participants were Caucasian, whereas the highest rate of suicide attempts (55.31%) was among First Nations, who accounted for <1.5% of participants. Caucasians, by contrast, had the lowest attempt rate (36.80%). More participants obtained a bachelor's degree and fewer an associate or technical degree than any other level of education. Suicide attempts were highest among those with ≤some high school (50.70%) and lowest among those with an advanced degree (30.25%). More participants made an income of $20–$50,000/year and less $10–$20,000 than any other income bracket.
Conclusion:
SITBs, among the transgender population, are both universally high and impacted by race/ethnicity, educational attainment, and income. These findings may be useful in creating culturally and factually informed interventions for transgender individuals experiencing SITBs and in informing future research on this topic.
Introduction
Transgender people—whose gender identity is incongruent with the sex assigned to them at birth—are increasingly publicly visible. 1 Despite, or perhaps because of this, they are extremely vulnerable to discrimination, violence, and marginalization, the experience of which has extremely negative impacts on their health and well-being. 2 Shockingly high rates of suicidal thoughts and behaviors (SITBs), previously identified as averaging 55% for ideation and 29% for attempts over the lifetime, are a clear indication of these negative impacts. 3 What relationship do race/ethnicity, educational attainment, and income have with SITBs among transgender adults? We address this question through a systematic review of 21 years of peer-reviewed and gray literature on the topic and, in doing so, update and provide an added analysis to the lead author's previous publication on the matter. 3 To do so, we used data on transgender participants from 64 distinct research projects i published in 108 articles between 1997 and 2017 (Table 1).4–110
Studies in This Meta-Synthesis
In all cases, the y-axis of each figure represents the proportion of the cohort population. The data sets are organized from left to right, by increasing suicidality figure found by each study.
These studies seem to have included intersex and/or cis gender respondents, without allowing for their suicidality data to be individually assessed.
EHR, electronic health record; FTM, female to male; GRS, gender reassignment surgery, alternatively known as gender affirming surgery; ICD, International Classification of Diseases; MTF, male to female; VA, veterans administration.
Historical trends
As previously noted, the scientific and clinical approach to transgender health has generally evolved from the use of a disease-based model, prevalent from the 1950s to the 1990s,6,111 to the one that uses an identity-based lens.3,112 Under this lens, transgender SITBs can be understood as significantly being influenced by anti-transgender discrimination and minority stress.22,28,53 Within the disease-based lens, however, transgender SITBs are attributed to individualized psychopathology or neurobiology.8,113 The literature on transgender health has, therefore, increasingly moved from viewing transgender people as aberrant and pathological, to affirming gender identity as part of a varied spectrum and, where appropriate, offering supportive interventions. In this context, practitioners provide medical and therapeutic interventions that affirm rather than “correct” an individual's gender identity. 114 Nevertheless, the disease-based lens continues to be employed in some cases.112,115
Meta-analyses and systematic reviews
There are 25 meta-analyses and systematic reviews summarizing the literature on transgender SITBs. However, 20 address the issue primarily among youth or children; as secondary or incidental to another issue (e.g., HIV), a single aspect of a larger topic (e.g., transgender health); or among sexual minorities writ large (e.g., LGBT). The five meta-analyses and systematic reviews that primarily assessed SITBs among transgender adults are Marshall et al., 116 Virupaksha et al., 117 McNeil et al., 118 Wolford-Clevenger et al., 119 and Adams et al. 3 Two116,118 account for review parameters (exclusion of gray literature) but fail to identify a number of studies and, in one case, count a single data set multiple times. One 117 includes gray literature, but only selects articles freely available online and relevant to the review title, without explaining how the latter was systematized. One 119 identifies factors (attempts, behavior, and deaths) correlated with transgender SITBs in literature published between 1991 and January 2017 but does not analyze data on SITBs in this literature. One 3 presents an earlier stage of this research, which excludes literature published since February 2016 and does not focus on the impact of ethnicity, income, or education on SITBs. Therefore, this systematic review provides a more robust synthesis and analysis of the available data on transgender SITBs.
Methodology
Eligibility criteria
As in the previous publication on this topic, 3 studies were included in the systematic review if they took place in Canada or the United States; published in English-language journals, theses, or project/institutional reports between 1997 and 2017; reported original participant research on transgender suicide attempts and/or ideation; and included quantitative data on SITBs among ≥5 participants, at least ≥51% of whom were 18 years or older at the time of participation. In addition, this systematic review incorporated studies on both clinical and nonclinical populations (Table 1). The former typically required participants to have a diagnosis of gender dysphoria 120 and/or be receiving transitional health care services (e.g., hormones and surgery). The latter, by contrast, tended to include participants based on self-identification as any of several transgender identities. Articles were excluded if they reported only on suicide deaths or nonsuicidal self-injury, single case reports, or subsumed transgender data into a larger population (e.g., LGBT). Although research published multiple times was only counted once, all reports were assessed for useful data. Nonwritten reports like poster presentations were excluded. The inclusion of gray literature helped to increase the data pool, reduce the impact of publication bias, and incorporate thesis research that may ultimately result in peer-reviewed publications. Note, however, that only 9%, or 14% of all studies, were non-peer reviewed by the end of the review inclusion period. Given the observed tendency for these publications to achieve peer review over time, it can be assumed that the majority will gain this status, particularly the 6 published since 2015.
Data collection
Of the 64 distinct research projects (and 108 articles) that make up this systematic review, 7 originated in Canada and 57 in the United States. Where possible we excluded participants <18 years; however, as data on SITBs was usually presented for the totality of participants, this was not always possible. Of these 64 projects, 55 were peer reviewed, 3 were theses, and 6 were project or institutional reports. We then extracted partial or complete data on transgender participants' race/ethnicity (n=56), education (n=49), and income (n=33). In some cases, we supplemented this through interviews with the study authors, which the first author conducted as part of his MSW thesis. Specifically, the first author interviewed 18 authors of publications on transgender SITBs and, in some cases, minor additional statistical information was reported in these interviews. We have not indicated where this occurred to ensure the confidentiality guaranteed in the initial research ethics board approval from Dalhousie University. 121
Literature review
This literature review is the culmination of three sequential reviews: the lead author's thesis, 121 an update 3 focused on 1997 to February 2016, and the one conducted for this article that focused on 21 years of research on transgender SITBs (1997–2017 inclusive). Literature was identified primarily by keyword searching WorldCat, Google Scholar, and Google Search. WorldCat, as one of the largest catalogs of cross-referenced and multidisciplinary academic literature, was the primary source of material. The following keywords were used: “transgender suicide”; “transsexual suicide”; “FTM suicide”; “MTF suicide”; “transsexual suicidality”; “transgender suicidality”; “transgender suicide attempt”; and “transsexual suicide attempt.” This was supplemented by hand searching the reference lists of identified articles and looking for new publications from previously identified research projects.3,121 The latter were identified by searching named projects (e.g., The Trans PULSE Project) 53 and checking the outputs of identified authors on Google Scholar, Google Search, PubMed, LinkedIn, and ResearchGate. We also reviewed Ramsay's collated list of publications on transgender SITBs. 122
We initially identified 3,881 articles, of which 2,481 duplicates were eliminated (Fig. 1). Upon reviewing titles and abstracts of the remaining 1,400 articles, we excluded a further 939 that failed to mention transgender SITBs, consisted exclusively of reference lists or audiovisual material, or were not in English. The full texts of the remaining 461 were reviewed and the following eliminations made: reported no original data on transgender suicide attempts and/or ideation (n=144), meta-analyses/reviews of transgender SITBs (n=24), no/unclear quantitative data (n=n=86), published before 1997 (31), not from the United States or Canada (n=55), the majority of participants were <18 years (n=9), and had ≤5 participants (n=4). The remaining 108 articles, representing 64 distinct research projects, were included in this systematic review.
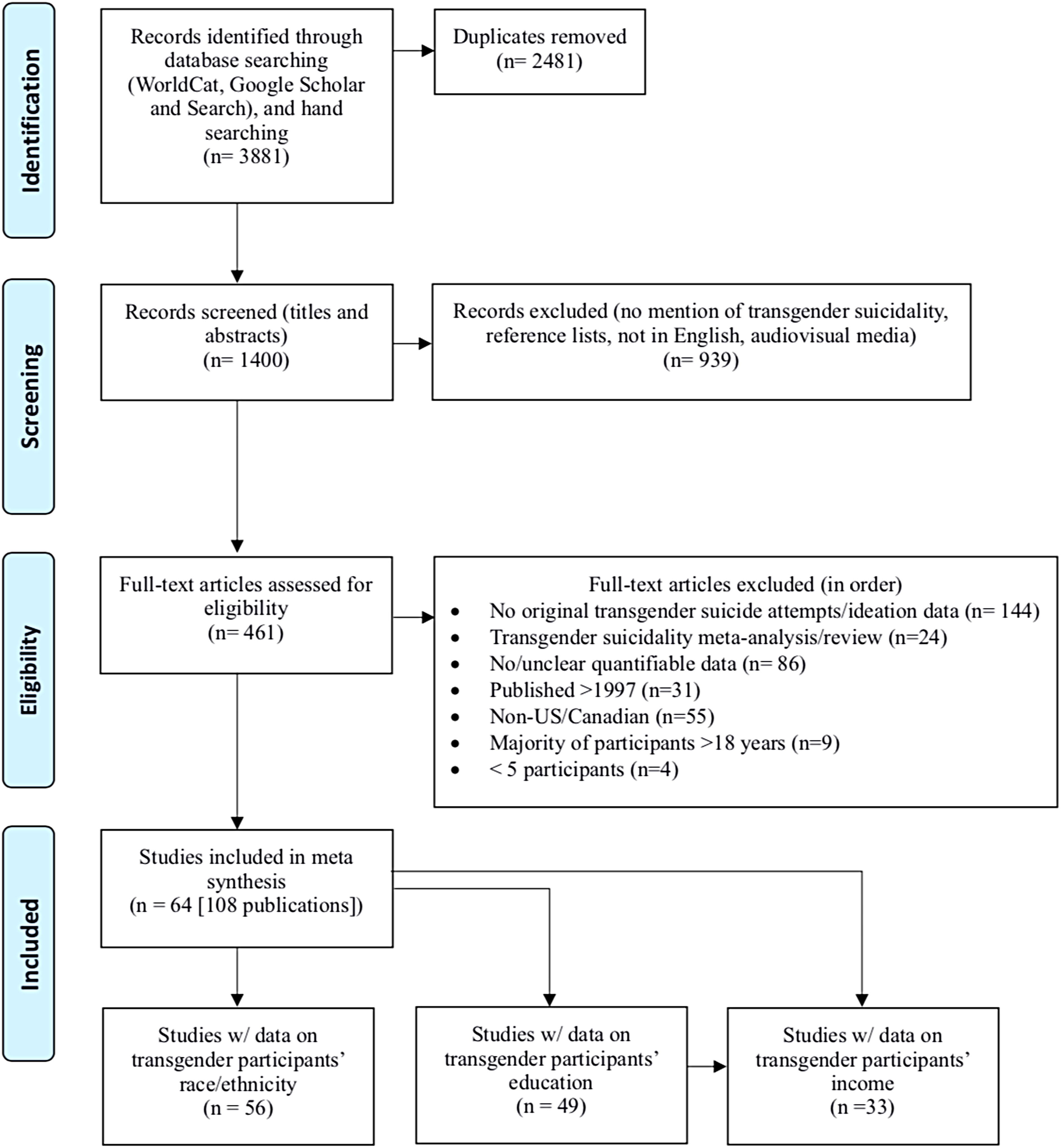
PRISMA Chart.
Data analysis
We extracted data on suicide attempts, ideation, and demographic details (race/ethnicity [n=56], ii education [n=49], iii and income [n=33] iv ) from 64 research projects. Whenever possible we recalculated these data using all study participants as the denominator, rather than only those that answered the given question, positioning nonrespondents as “negative cases' and our findings as conservative. SPSS v. 23 and Microsoft Excel 2016 were used to conduct two analyses. The first examined race/ethnicity, education, and income of transgender participants compared with US Census data. The US Census was used as a baseline because 89% of these projects originated in the US Census and, as a result, most took their demographic categories from it. The second analysis examined lifetime transgender suicide attempt statistics reported according to race/ethnicity and education. Other analyses (income and ideation) of SITBs were excluded for lack of sufficient data.
Of the 56 projects that reported data on race/ethnicity, four (7, 35, 59, 64) v were excluded from further analysis for reporting an amalgamation of ideation and attempts; three (9, 21, 60) for specifying SITBs over a nonstandard time period (e.g., when participants ‘first felt transgender’); six (19, 32, 38, 42, 52, 56) because race/ethnicity data were not collected using mutually exclusive categories, such that the proportions of each racial/ethnic group could not be considered in relation to the study's population size; and five (14, 44–45, 53, 57) for recording SITBs over participant's last year rather than their lifetime. The race/ethnicity data of the remaining 38 projects (n=26 for ideation, n=35 for attempts) was assessed. Our second race/ethnicity analysis began with the 19 projects that analyzed data on SITBs specific to participants' race/ethnicity. Seven of these (20, 36, 43, 48, 52–53, 56) were excluded because data were reported as a statistical analysis or model, one (42) because ethnic-specific data on SITBs were recorded differently than overall demographic data, and one (44) because SITBs were recorded over a fixed period. The ethnic/race-specific SITBs data of the remaining 10 (6, 11, 19, 26, 31–33, 41, 46–47) projects were compared.
Of the 49 projects that reported on participant educational data, eight (1, 2, 6, 14–16, 28, 52) were excluded for doing so in a manner (e.g., Hollingshead average) inconsistent with the majority, seven (3, 7, 44–45, 53, 57, 60) for recording SITBs during a fixed time, one (59) for conflating suicidal ideation and attempts, and one (18) because being a college student was a requirement. The education data of the remaining 32 projects (n=20 ideation, n=29 for attempts) were assessed. Our second educational analysis began with the 10 projects that analyzed SITBs with regard to participants' educational level. We eliminated five (20, 41, 43, 48, 52) that reported on this in a statistical model. The educational data of the remaining five (11, 19, 26, 31, 46) were assessed.
Of the 33 projects that reported on participant income, 16 (1, 2, 7–8, 11, 14, 28, 30, 32, 35, 40, 47–48, 53) were eliminated for doing so in a nonstandard format (e.g., relation to poverty line). The income data of the remaining 17 projects (10 for lifetime ideation and 16 for attempts) were assessed. Important to note, however; only five projects provided comparable income data for ideation and seven for attempts using the same five common income ranges from ≤ $10,000 to ≥ $100,000. Our analysis of income was, as a result, limited.
Results
Lifetime suicidal ideation was reported in 34 studies (average=46.55%; range=18.18–95.50%) and attempts in 46 studies (average=27.19%; range=8.57–52.40%). Average lifetime SITBs in the 38 projects that reported comparable data on both suicide and race/ethnicity was 45.44% for ideation (range=18.18–82%) and 27.88% (0–40.00%) for attempts. An average of 67.75% (3.70–96.73%) vi of these participants were Caucasian and 28.05% (0–95.63%) were nonwhite. Participants in 12.78% (0–21.74%) of the projects were Asian/Pacific Islanders; 11.03% (0–43.90%) Hispanics; 6.57% (0–28%) and 5.58% (0–69.43%) Black/African American and biracial/multiracial, respectively; and 1.46% (0–27.40%) First Nations. A final 0.79% (0.15–18.15%) were classified as “other,” whereas the ethnicity of 4.44% (0–68.52%) was unknown. In comparison with US Census data (Fig. 2), 123 our findings show fewer Caucasian (67.75% vs. 76.6%), Black/African American (5.58% vs. 13.4%), and Hispanic (11.03% vs. 18.1%), greater Asian/Pacific Islanders (12.78% vs. 6%) and biracial/multiracial (6.57% vs. 2.7%), and roughly equal First Nations participants (1.46% vs. 1.3%). Average lifetime suicide attempts using data on SITBs specific to race/ethnicity (Fig. 3) was 39.32%. First Nations reported the highest rate of lifetime suicide attempts (55.31%), followed by biracial/multiracial individuals (50.92%), Black/African Americans (45.47%), Hispanics (44.37%), Asian/Pacific Islanders (39.11%), and Caucasians (36.80%).
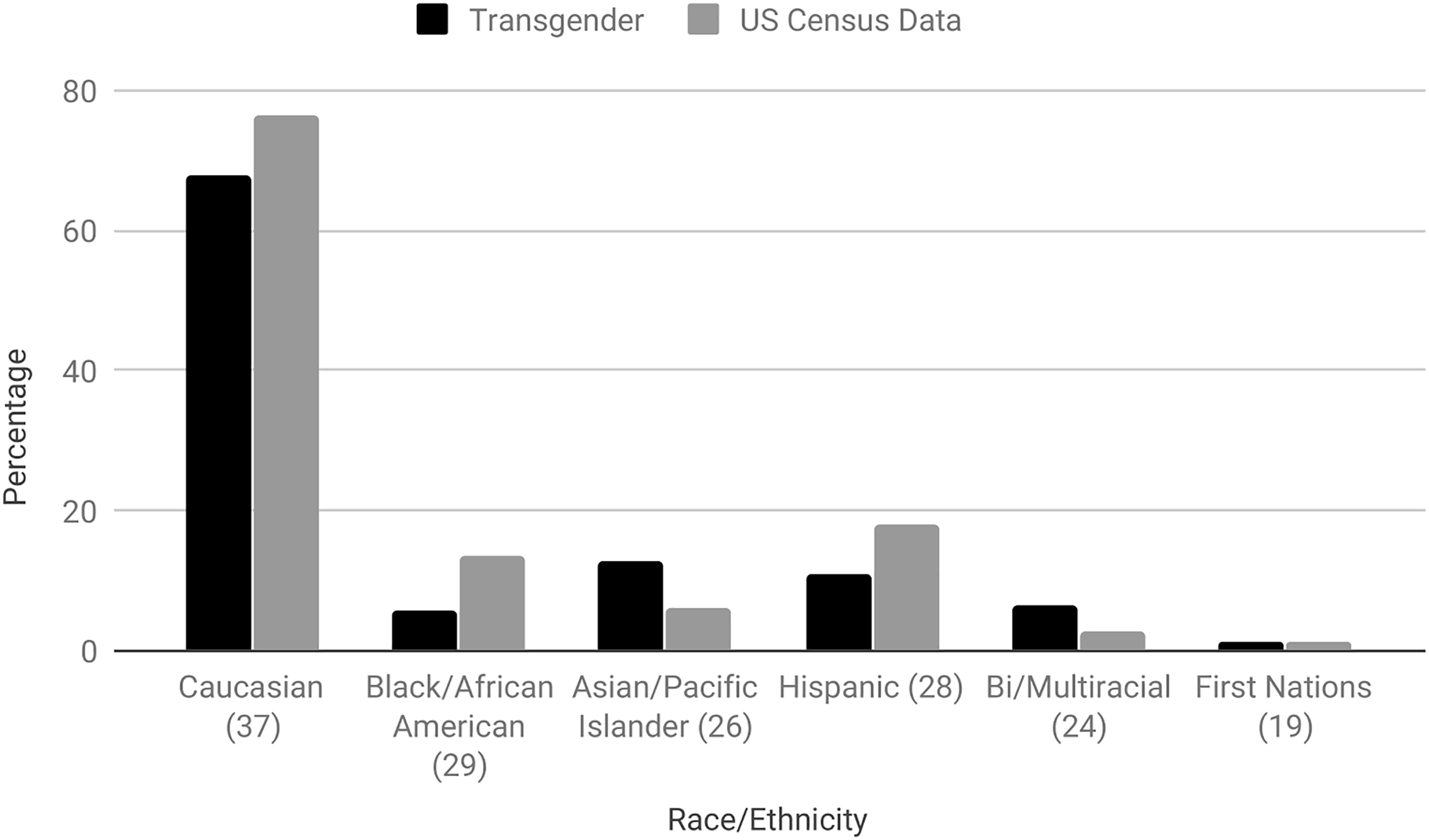
Transgender race/ethnicity versus US Census data. Figures in parenthesis specify the number of individual studies used in the calculation of transgender race/ethnicity.
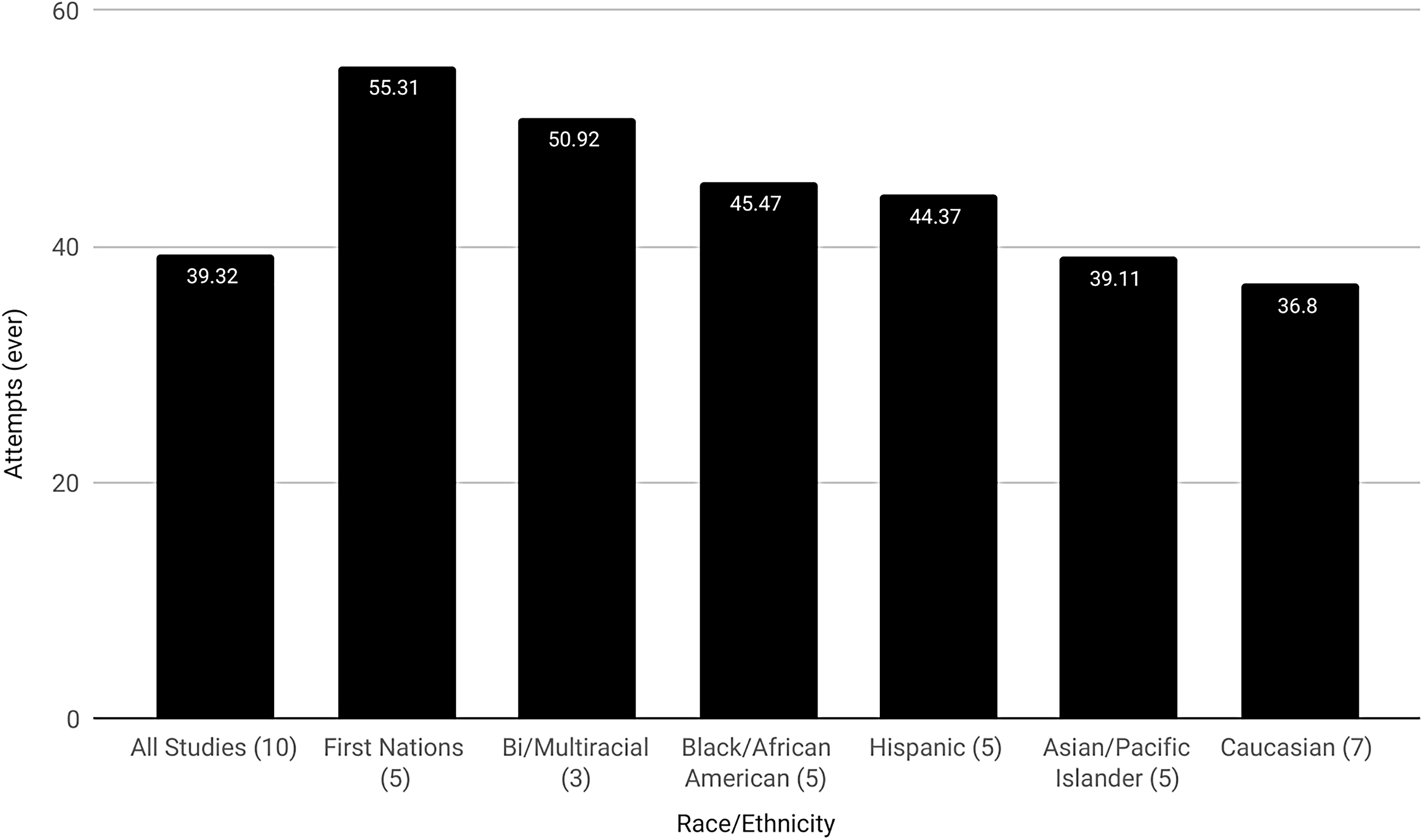
Lifetime transgender suicide attempts according to race/ethnicity. Figures in parenthesis specify the number of individual studies used in the calculation of suicide attempts specific to transgender race/ethnicity.
The average rate of lifetime SITBs in the 32 projects that reported comparable data on both suicide and education was 46.26% (18.18–95.50%) for ideation and 27.16% (11.11–43%) for attempts. An average of 24.79% (2.87–36.90%) of participants completed a bachelor's degree, 21.5% (7.32–100%) some college, 21.06% ≤ (0.47–40.08%) some high school, 17.59% (6.40–63.06%) high school, 13.53% (7.32–100%) ≥ an advanced degree, vii and 8.58% (1.15–27.27%) an associate or technical degree. The educational achievement of 33.55% (0–80.80%) of participants was unknown. Compared with the US Census (Fig. 4), 124 transgender participants had lower rates of high school (17.59% vs. 28.89%) completion and higher attainment of ≤ some high school (21.06% vs. 11.04%), some college (21.5% vs. 18.86%), a bachelor's degree (24.79% vs. 20.04%), and ≥ an advanced degree (13.53% vs. 11.4%). Associate or technical degree attainment was comparable with the general population (8.58% vs. 9.77%). Average lifetime suicide attempts using SITB data on SITBs specific to education (Fig. 5) was 39.53% and appears to drop with the level of education achieved. Specifically, attempts peak among those that had ≤ some high school (50.7%), followed by completed high school (48.73%), some college (45.59%), an associate or technical degree (42.43%), a bachelor's degree (33.35%), and ≥ an advanced degree (30.25%).
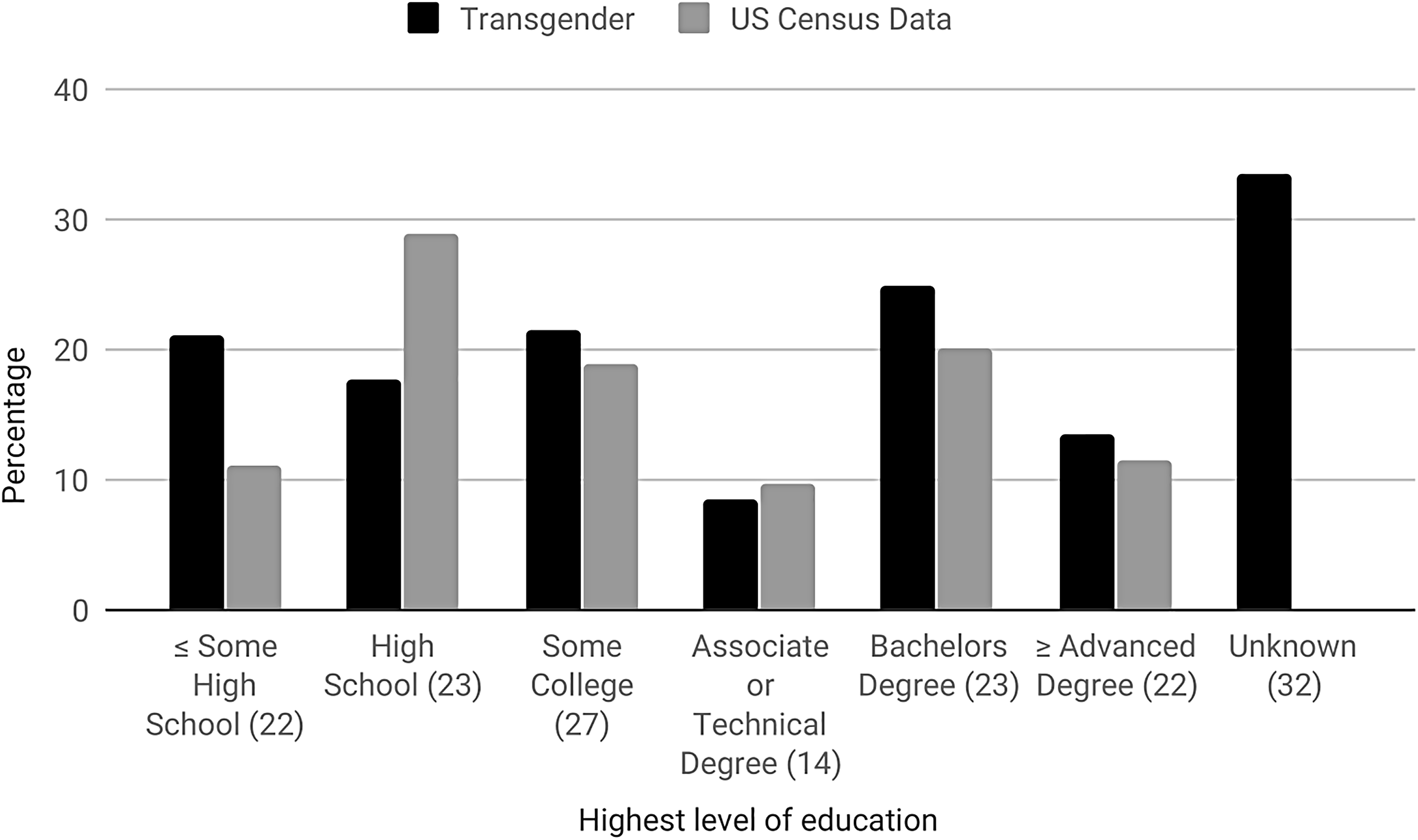
Transgender educational attainment versus US Census data. Figures in parenthesis specify the number of individual studies used in the calculation of transgender educational attainment.
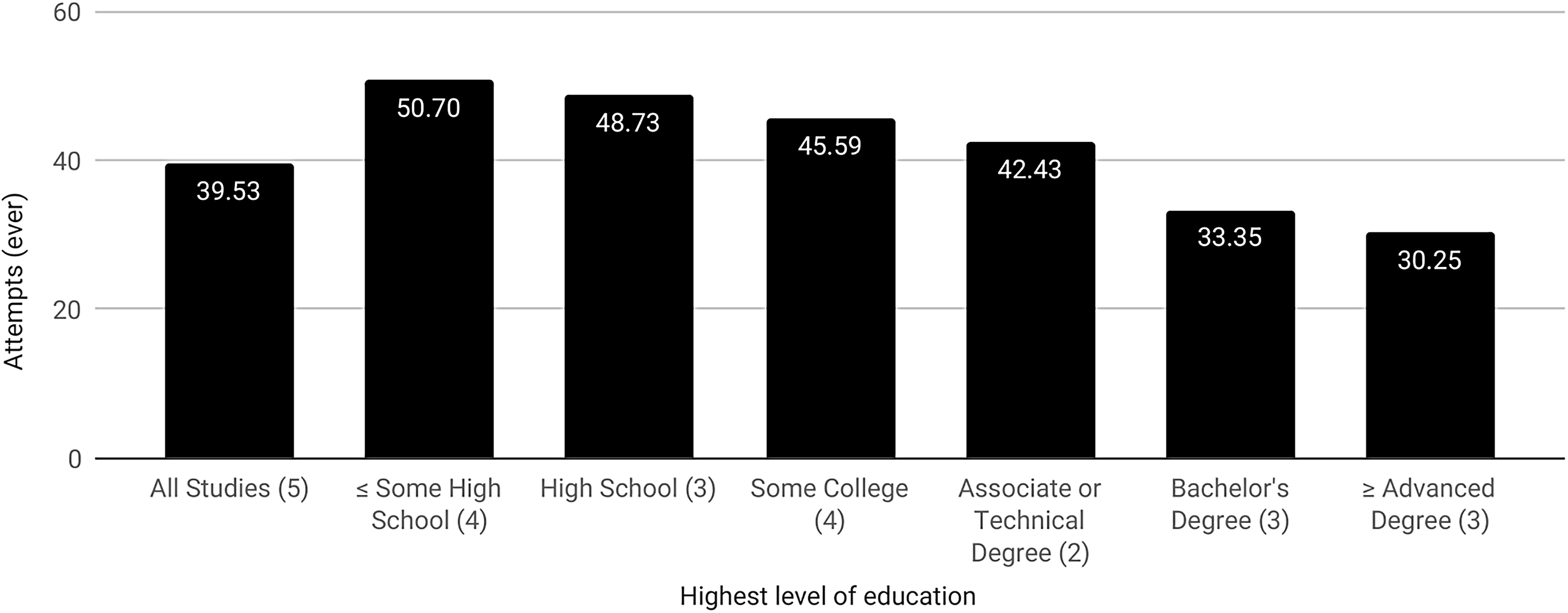
Lifetime transgender suicide attempts according to educational attainment. Figures in parenthesis specify the number of individual studies used in the calculation of suicide attempts specific to transgender educational attainment.
The average rate of SITBs in the 17 projects that reported comparable data on both suicide and income was 80.76% (34.92–82%) for ideation and 39.25% for attempts (16.27–45.80%). About 26.98% (19.96–40.74%) made $20–50,000, 22.72% (8.45–32.53%) made $50–100,000, 16.14% (8.43–60.32%) made ≤$10,000, 14.17% (2.32–15.21%) made ≥$100,000, and 12.67% (11.68–29.63%) made $10–$20,000. The income of 12.78% (0–89.18%) was unknown. Compared with the US Census (Fig. 6), 125 transgender participants reported lower overall income. Specifically, more made ≤$10,000 (16.14% vs. 6.05%) and $10–$20,000 (12.67% vs. 9.38%), whereas fewer made $50–$100,000 (22.72% vs. 28.97%) and ≥$100,000 (14.17% vs. 29.25%). The proportion of the transgender and general population making $20–$50,000 was roughly equal (26.98% vs. 26.35%).
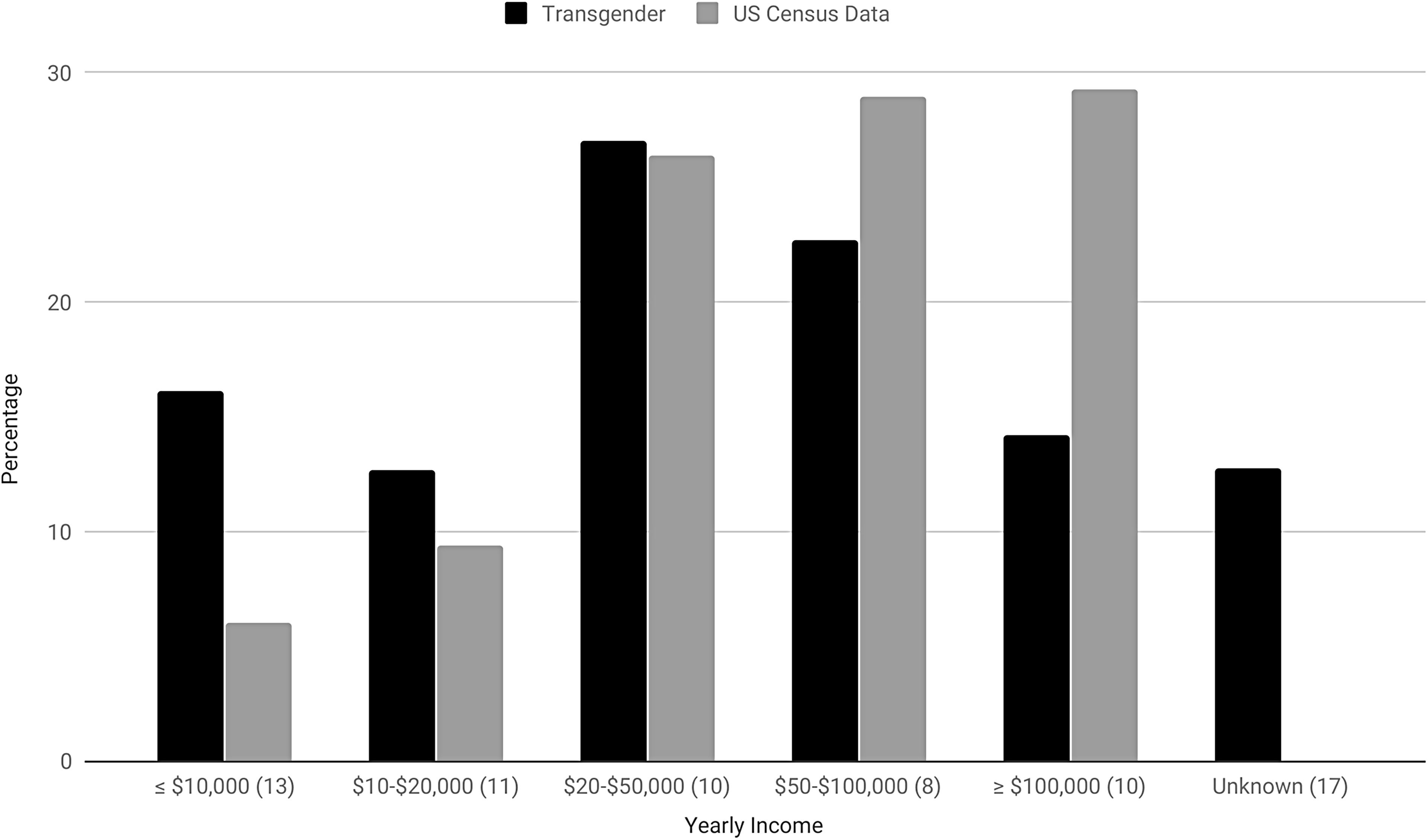
Transgender yearly income versus US Census data. Figures in parenthesis specify the number of individual studies used in the calculation of transgender income.
Discussion
Findings
The methodological rigor of studies on transgender SITBs continues to increase and, although cross-sectional studies are most common, a small but increasing number utilize the more rigorous case–control design. The amount of research on this topic is also increasing, with 14 projects first published from 1997 to 2007 and the remainder since. In fact, following the authors' previous study on this subject, which included studies published to February 2016, 3 22 projects, or 34% of the total, have been added. We can expect this trend, which may partially result from the heightened profile of transgender issues and civil rights, to continue. Similarly, although 49 of the studies included fewer than 500 participants, there has been a trend toward exceptionally high cohorts in more recent studies; for instance, n=1,250, 51 n=6,456, 43 n=5135, 65 n=27,715, 78 and n=92,000. 108
Our findings of an average rate of 46.55% lifetime suicidal ideation and 27.19% attempts among transgender participants are similar to those found in the authors' previous study (56% ideation, 29% attempts), although obviously lower with regard to ideation. 3 The preponderance of evidence suggests that high rates of SITBs, rather than being inherent to transgender individuals, result from barriers to transitional care, stigma, and discrimination.11,44,59,126 In addition, by definition, lifetime experience of SITBs is cumulative and while a person may cease to be actively suicidal they will still have had the experience of being suicidal.
It is difficult to make any strong statements on the recruitment and representation of diverse populations in research on transgender SITBs and the relationship between the racial/ethnic diversity of these projects and that of the general population. It is, however, possible to make some basic observations. Online recruitment, although often unable to incorporate the cultural and situational needs of African American participants, 127 is increasingly seen as an ideal way to access hidden populations like the transgender community. 128 Employment of key informants and snowball sampling, addressing reluctance to participant in research, and the use of incentives and in person recruitment may help to counter African Americans and other marginalized groups' suspicion of research (p. 3). 129
Our observation that relatively low rates of suicide attempts occur among Caucasian participants is inconsistent with previous research demonstrating higher rates in this population (Fig. 3). 130 There is, however, variation in the research literature on this point131,132 and evidence exists that capture of Black/African American SITBs, in particular, suffers from data disparities and misclassification.132,133 Indeed, we noted relatively high rates of SITBs among Black/African American participants, a group for which SITBs, where police are involved, are sometimes miscategorized as “suicide by cop.”133,134 This is one potential explanation for the observation that low rates of SITBs among Black/African American is at odds with other findings of negative comparative race-based health outcomes. 134 Our findings may suggest that Black/African American transgender individuals are less likely to attempt suicide in a manner that invites misclassification, or possibly that their transgender status itself causes their SITBs to be correctly classified. It should also be noted that we are discussing attempted suicides in which, by definition, the individual has survived and can clarify their intent. However, it should be noted that self-report is not without its limitations, as participants often give different responses to this question depending on the presence of and definition of “attempt” and whether a single question is used. 135
Our observation of higher rates of SITBs among First Nations individuals 136 is consistent with other findings that attribute this to colonization-based trauma.137,138 Likewise, we observed comparatively low rates among Hispanics and Asian/Pacific-Islanders. 132 However, there is evidence that SITBs vary greatly within ethnic categories. Puerto Ricans, for instance, have been noted to experience a greater incidence of SITBs than other Hispanics. 132 Nevertheless, there is comparatively little research on SITBs within racial/ethnic groupings and, depending on the study, conflation of existing categories (e.g., Asian Americans and American Indians). Variable racial/ethnic definitions are also a problem. 132
Consistent with the rapid increase in biracial/multiracial people in the United States, several studies include information on this population, although few report findings on SITBs specific to them. This is also the case in research on SITBs among nontransgender individuals.139,140 Research that does exist tends to focus on youth which, like our own observations, show heightened attempts among biracial/multiracial compared with monoethnic groups. 141 This may result from experiencing racial discrimination from multiple locations and the stress caused by conflict between one`s internal self and external world. 142 Nevertheless, the lack of data makes it difficult for us to compare our observations with others and future research into SITBs among biracial/multiracial transgender adults is clearly called for.
Research on transgender individuals' educational attainment is relatively scarce, highly variable, and lacking a clear consensus. As a result, the findings in these projects cannot be presented as typical or generalizable. Comparison of our observations to data from the US Census is made more difficult by variation in the categorization of education within these research projects and with the US Census (Fig. 4). For instance, recent US Census data does not record the category of ‘some high school.’ 143 Nevertheless, the categorization of US Census educational data more closely mirrors the projects in this systematic review than Canadian Census data, 144 and our own observations grossly compare with the general population. This systematic review also suggests that lower rates of SITBs may be associated with higher levels of educational attainment (Fig. 5), which is largely consistent with other findings of fewer SITBs among individuals with at least a college degree and more among those with less.145,146
Many transgender students experience a hostile educational environment that can jeopardize or even disrupt their education. Students so affected may opt out of or be refused access to education because of, for instance, their gender presentation.147,148 Although a number of transgender individuals return to school and achieve advanced education later in life, it can be difficult after early and often traumatic disruption, 43 which may explain some findings of low educational achievement.147,149 Given the high number of convenience samples, this may particularly be the case in research that is overrepresented by especially vulnerable participants. 148 Addressing gender diversity in education and increasing scholarship on this subject will help to challenge the disparities that prevent transgender people from full educational participation and, given the protective effect of educational achievement, may lead to a reduction in their experience of SITBs. 150
The lack of individual project data on transgender SITBs according to income, and a complete absence of research into lifetime income among transgender individuals, limits our ability to comment on the relationship between these factors. It should also be noted that, although this systematic review found a lifetime suicide ideation rate of 80.76%, it also included a single study that had 27,715 participants and high suicidal ideation. We did, however, observe that several studies noted a relationship between transgender SITBs and high rates of poverty or un/underemployment and,43,151 within the literature, transgender individuals were observed to be four times more likely than the general population to make <$10,000/year.44,151 This is consistent with the observations of our systematic review that transgender participants are almost three times more likely to make ≤$10,000 (Fig. 6). Similarly, transgender unemployment, discrimination, and poverty are also strongly associated with workplace discrimination and, in turn, lack of education and self-harm. 114 Another key consideration is that poverty curtails a transgender individual's access to medical transition, which is a known protective factor. 59 This is especially true in environments, like the United States and some parts of Canada, without transgender-inclusive universal health care.
Implications for future research
The myth that transition leads to SITBs continues to be used to deny transgender health care access and legislative rights, despite a lack of empirical support for this position and repeated research debunking it.3,152–159 A more productive avenue for addressing the phenomenon of transgender SITBs might be to investigate the protective factors inherent in transgender health care,33,160–163 and the negative impacts of denied access.40,57,126 In particular, research is needed on the impact of resiliency, minority stress, 164 and culturally protective factors on transgender SITBs. An exploration of syndemic factors, particularly with regard to interrelated issues like racism, poverty, and education, would also be a fruitful avenue for research. For instance, only one study has reported on SITBs among transgender refugees. 105 We recommend that researchers explore transgender SITBs among various ethnicities, rather than flattening it into a comparison between whites/Caucasians and people of color, ethnic minorities, or racialized individuals. Methods of gathering these data include asking participants to write in their race/ethnicity, reporting on ethnicity and race separately, 124 using census categories, and/or allowing for the selection of multiple ethnicities.165,166 Regardless, the choice should be clearly explained and rationalized in the resulting publications.
We further recommend that, where practical, participants be allowed to write in their actual or estimated income, which will allow comparison across a variety of monetary brackets. Where participants are asked to self-report SITBs, we suggest that a definition be provided of the item being measured and, where possible, multiple questions be asked. 135 Finally, the creation of project websites will allow findings to be collected and disseminated from a central location. In revising the literature review from the previous publication, 3 these websites were invaluable in helping us identify project updates and data published across multiple studies. Giving the project a unique and distinct name, ideally with an available website URL, and using it in promotion and branding will assist in making them easily locatable (e.g., The Trans PULSE Project 53 ).
Limitations
These findings are preliminary and lack generalizability for several reasons. The included studies rely heavily on self-reported SITBs and individual definition of “attempt” and “ideation” can vary a great deal, particularly when a definition is not provided and only a single question is used. 135 Second, because the majority of the 64 projects that make up this systematic review use convenience samples, which do not tend to result in representative or easily replicable data. 147 There is also a high degree of heterogeneity between these projects; for instance, the categorization of race/ethnicity, education, and income and the size of cohorts (n=5–92,000 participants), the latter of which obscures the impact of small samples and overemphasizes the representativeness of large ones. Studies 46 (n=27,715) and 62 (n=92,000) have a particularly disproportionate impact on the results presented here. 167 Another concern is the small-study effect, whereby small cohort studies of lower methodological rigor report different effects than larger ones.167,168 To some degree, concerns of heterogeneity are mitigated by aggregating these projects into a systematic review, although caution should still be taken in interpreting and applying findings. Indeed, the fact that this is a systematic review is itself limiting, as it is bound to exclude unpublished results because of publication bias, 167 although this is also mitigated by our inclusion of gray literature.
In addition, income, educational attainment, and race/ethnicity are also often correlated. For instance, one's race/ethnicity directly impacts their income and access to education. 169 It is, therefore, difficult to observe or discuss these factors in isolation of one another and our findings should be interpreted in light of this limitation. We suggest that future research on the subject of transgender SITBs, in relation to race/ethnicity, education, and income, collect discrete data on each of these factors and subject them to statistical tests, like stepwise regression, to determine the impact of each factor alone and together on SITBs.
Participation bias, particularly in mental health research, is also an issue in recruitment and reporting of participants. 170 Other research has demonstrated that men and individuals with a substance abuse or dependence history are more likely to participate in research on suicide attempts. 171 More broadly, people who have experienced SITBs, or are in greater distress generally, may be more likely to participate in studies on this subject. Likewise, research undertaken on clinical populations, or only those with specific presenting issues, may find higher rates of SITBs than population or community-based samples. This is mitigated somewhat by our inclusion of both clinical and nonclinical samples, the latter of which often used population and community-based recruitment. On the contrary, stigma related to SITBs and/or gender identity may prevent individuals from participating in or accurately reporting on their experiences in research on this subject.
As noted in the lead author's previous study, 3 gender identity definitions and terms are in flux, 172 differ among individual projects, and documentation of nonbinary genders continues to be limited. 173 The way individual projects inquire into SITBs is also a concern. It has, for instance, been noted that yes/no questions like “have you ever attempted suicide” tend to overestimate SITBs by combining self-harming behavior with and without suicidal intent (p. 3). 44 There is some evidence that in-person interviewing reduces reports of attempts among adults, although this is an uncommon methodology within research on transgender SITBs, possibly because of cost and privacy concerns.3,174,175
Conclusion
This systematic review supports findings of high, if heterogeneous and widely variant, rates of SITBs among transgender adults in the past 21 years. With regard to transgender individuals, it observes that Caucasians experience lower rates of SITBs than other groups; that high levels of educational achievement seem to protect against SITBs; and that they may be at risk of higher SITBs because of relatively low income. Research on the topic of transgender SITBs would be improved by greater consistency in data collection and improved research methodology.
Footnotes
Acknowledgment
The authors thank Dr. Laura Kuper, Cheri Moody, and Maaya Hitomi for their comments on early versions of this article.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
No funding was received for this article.